Journal of Hematology & Thromboembolic Diseases
Open Access
ISSN: 2329-8790
ISSN: 2329-8790
Case Report - (2013) Volume 1, Issue 2
The subject is a 45-year old female who visited the hospital due to irregular vaginal bleeding. Her white blood cell count was 170400/ uL and LDH level was 2099 iU/L. The subject was diagnosed with acute myeloid leukemia type M2 by bone marrow examination. The chromosomes were 46, XX, add(3)(p21), add(8)(q22), and add(21)(q22). The PCR (Polymerase Chain Reaction) examination confirmed that the positive AML1/ETO. Although one course of idarubicin hydrochloride (IDR: 12 mg/m2 for three days) plus cytarabine (AraC: 100 mg/m2 for seven days) was conducted as remission induction therapy, remission was not achieved. Since the bone marrow examination also observed meningeal infiltration, a second course of IDR plus AraC was combined with intraspinal administration of antitumor drugs, aiming for reremission induction. Although the meningeal infiltration disappeared, non-remission status remained. We then conducted two courses of FLAG-M (AraC 2 g/m2 twice a day for four days, fludarabine 15 g/m2 twice a day for four days, mitoxantrone 10 mg/ m2 for three days, and granulocyte colony-stimulating factor: G-CSF 75 μg) and one course of MEC (AraC 1 g/m2 for six days, etoposide 80 g/m2 for six days, and mitoxantrone 6 mg/ m2 for six days). These regimens did not lead to a complete remission.
The subject is a 45-year old female who visited the hospital due to irregular vaginal bleeding. Her white blood cell count was 170400/ uL and LDH level was 2099 iU/L. The subject was diagnosed with acute myeloid leukemia type M2 by bone marrow examination. The chromosomes were 46, XX, add(3)(p21), add(8)(q22), and add(21)(q22). The PCR (Polymerase Chain Reaction) examination confirmed that the positive AML1/ETO. Although one course of idarubicin hydrochloride (IDR: 12 mg/m2 for three days) plus cytarabine (AraC: 100 mg/m2 for seven days) was conducted as remission induction therapy, remission was not achieved. Since the bone marrow examination also observed meningeal infiltration, a second course of IDR plus AraC was combined with intraspinal administration of antitumor drugs, aiming for reremission induction. Although the meningeal infiltration disappeared, non-remission status remained. We then conducted two courses of FLAG-M (AraC 2 g/m2 twice a day for four days, fludarabine 15 g/m2 twice a day for four days, mitoxantrone 10 mg/ m2 for three days, and granulocyte colony-stimulating factor: G-CSF 75 μg) and one course of MEC (AraC 1 g/m2 for six days, etoposide 80 g/m2 for six days, and mitoxantrone 6 mg/ m2 for six days). These regimens did not lead to a complete remission.
On December 21st, 2010, cord blood transplantation (CBT) was performed following pretreatment with busulfan (BU) 3.2 mg/kg for four days plus cyclophosphamide (CY) 60 mg/kg for two days plus total body irradiation (TBI) at 12 Gy. For prevention of acute graft versus host disease (GVHD), FK506 and short-term methotrexate (MTX) were used. A summary of the course after transplantation is shown in figure 1.
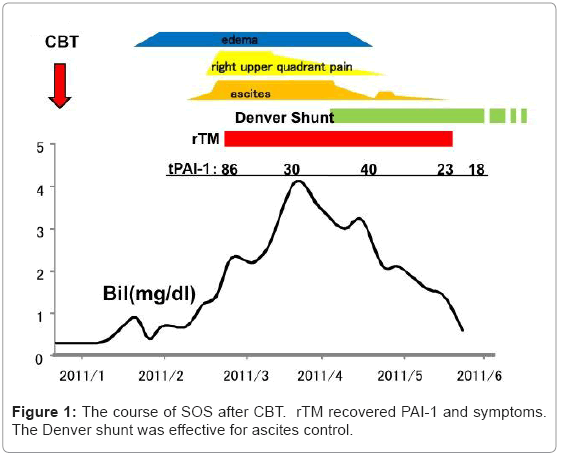
Figure 1: The course of SOS after CBT. rTM recovered PAI-1 and symptoms. The Denver shunt was effective for ascites control.
On January 11, 2011, the neutrophil count exceeded 500 uL and we determined that the transplanted cells had engrafted. After the engraftment, the subject’s body weight started to increase. A diuretic was used, but the ascites retention became worse. On January 18 (Day 28), a pain in the right hypochondrium appeared. We started tolvaptan on January 23; however, it had little effect. On January 28, the cytomegalovirus antigenemia assay was found to be positive and, therefore, valganciclovir treatment was started. Cytomegalovirus was negative on February 7 and the valganciclovir treatment was terminated. However, even during the treatment, the body weight and ascites remained out of control. The creatinine level increased up to 1.6 on February 16 and the FK506 treatment was halted (concentration of FK506 was 7.6 ng/ml). On February 20 (Day 61), the bilirubin level rose up to 2.0 mg/dL, thus meeting the Jones standard and McDonald SOS diagnosis criteria. The subject was therefore diagnosed with delayed sinusoidal obstruction syndrome (SOS). At this point, the fibrinogen level was 283 mg/dl, D-dimer was 2.3 μg/dl, and the plasminogen activator inhibitor-1 (tPAI-1) level had risen to 86 ng/mL. Thus, on Day 62, we began treatment with 380 U/kg of recombinant soluble thrombomodulin (rTM). In addition, fresh frozen plasma (FFP) was administered for abnormal coagulation. Antithrombin III (AT III) was also administered in order to maintain the antithrombin level over 70%.
On March 5, the pain in the right hypochondrium disappeared. Kidney function improved by March 15 (Day 84). Although the bilirubin level stayed around 3-4 mg/dL without rising after around Day 90, intractable ascites remained. The PAI-1 level dropped to 30 ng/ mL by Day 95. The bilirubin stabilization and creatinine recovery, along with the PAI-1 level decrease after administration of rTM, suggested that the SOS was fixed. On the other hand, the ascites was due to portal hypertension by minute hepatic vein obstruction. Thus, we determined that a peritoneovenous shunt (Denver shunt) could effectively control the ascites.
The Denver shunt was inserted on Day 107 for ascites control. After insertion of the Denver shunt, the ascites dramatically decreased and we reduced, then halted, the diuretic treatment. Although ascites retention was occasionally observed due to occlusion of the Denver shunt, the ascites decreased rapidly once the occlusion was removed. The bilirubin level gradually decreased and reached below 2 mg/dL on Day 139, indicating that the SOS had resolved. Since that time, there was no recurrence of leukemia or ascites retention. The Denver shunt was removed on Day 315.
Both the McDonald’s and Jones’s criteria for SOS require that it occur within three weeks of transplantation. However, SOS has occurred without transplantation or even after three weeks of transplantation. These SOS-like cases that meet all the criteria except for the timing of the occurrence have been reported as delayed SOS [1-3]. Toh et al. reported a case of delayed SOS in a patient over 40 on whom they used BU. The authors speculated that the use of ursodeoxycholic acid in the early stage of treatment could have prevented SOS; on the other hand, it also could have been involved in the delayed SOS [2]. Hasegawa et al compared 21 cases of delayed SOS to 17 cases of early SOS [3]. They found no correlation between the timing of the onset of SOS and its severity.
The risk factors for SOS are currently thought to include hepatitis virus, method of transplantation, method of graft-versus-host disease (GVHD) prevention, use of CY after BU, high dose radiation, oral BU administration, transplantation long after diagnosis, and more. In the case reported here, we administered BU, although by intravenous injection, expecting an effect on the central nervous system. We also performed systemic radiation and used ursodeoxycholic acid. These regimens could have been involved in the SOS development. On the other hand, during the period from the onset to the cord blood transplantation, five courses of chemotherapy were performed for eight months. In two out of the five courses, over 2 g per body surface area of AraC was used, and IDR and AraC were used two weeks prior to the transplantation. These regimens might also have been related to the SOS development.
Conservative therapies are generally performed for SOS. Although AT III is used on a trial basis in some cases, it is not thought to be effective. Defibrotide has also been reported to have some efficacy for delayed SOS. Nevertheless, it is not available in Japan and is expensive, and hence difficult to use [4,5]. rTM is on the market in Japan and previous reports have shown the effectiveness of this protein on SOS [6,7]. Also, in the case reported here, the PAI-1 level decreased and the pain in the right hypochondrium improved after the use of rTM. rTM may have some anti-inflammatory mechanism, such as the suppression of HMGB-1, which may prevent the development of SOS [8]. Some patients obtained CR of SOS only through supportive therapy [2]. There is a possibility that this case was a spontaneous remission and that rTM had contributed to the improvement of the SOS. On the other hand, there was difficulty in controlling the ascites and kidney function worsened even with the use of diuretics and tolvaptan. After we confirmed that the PAI-1 level remained low (SOS was successfully treated and the symptom had stabilized) and that no bacteria were detected in the ascites, the Denver shunt was inserted.
Treatment of SOS using a transjugular intrahepatic portosystemic shunt (TIPS) has been reported, but its effectiveness has been discredited [9]. TIPS can be used only when portal pressure is increased and portal pressure is not necessarily increased in SOS. In addition, the treatment was performed at an early stage after the onset of SOS when the SOS was not yet stabilized, resulting in a susceptibility to complications, such as bleeding. In the case reported here, the ascites was shunted directly into the vein. Therefore, a certain level of effect could be expected irrespective of the portal pressure. Moreover, the PAI-1 level was monitored during the treatment in order to confirm that the SOS condition was stabilized. These factors made the treatment effective without any severe complications.
The rTM effectiveness and mechanism of action have shown not only improvement of coagulation abnormality through protein C, but also anti-inflammatory effects. Nomura et al. reported that rTM suppresses inflammatory substances, such as high mobility group box (HMGB) 1 protein, interleukin 6 (IL6), and tumor necrosis factor alpha (TNFα) [8]. Suppression of these inflammatory substances may contribute to the inhibitory effect of weight gain due to the inhibitory effect on capillary leak [6]. However, more case reports must be accumulated in order to clarify the effectiveness and mechanism of action of rTM against SOS. Furthermore, the shunt can be effective for ascites control in SOS when the right timing and type of shunt are selected.