Journal of Hematology & Thromboembolic Diseases
Open Access
ISSN: 2329-8790
ISSN: 2329-8790
Review Article - (2016) Volume 4, Issue 4
Evidence based guidelines for the neonatal transfusions are still emerging. It is always a conundrum for a pediatrician, to decide when to give packed red blood cells to a growing premature infant with or without signs and symptoms of chronic neonatal anemia. It is further complicated, as some of that clinical picture can be explained by co-morbidities like neonatal sepsis, apnea of prematurity and caffeine therapy. So, that physician needs to weigh the risks and benefits for such seemingly benign procedure and also rule out conditions that can mimic the signs and symptoms of anemia of prematurity.
Here, an attempt was made to provide suggestions for giving neonatal transfusion, using an algorithm approach. A review of recent literature was done and a short review was provided.
Keywords: Neonatal anemia; RBC transfusion; Transfusion dilemma
A neonatal intensive care unit (NICU) stay can be very complex and prolonged, especially for infants with birth weights of less than 1000 grams (Extremely Low Birthweight-ELBW). Before they graduate from the NICU, they end up receiving at least one, and frequently several blood transfusions [1]. Because of lack of evidence- based transfusion guidelines, the indications for transfusions are often not clear to the health care team. This knowledge gap encourages variation in transfusion practices [1]. Almost daily, a neonatologist faces the question of whether to transfuse packed red blood cells (PRBC) or not. These patients are often growing preterm infants with no evidence of acute blood loss, but have a low hemoglobin and hematocrit (Hb/Hct), with or without symptoms. The purpose of this short review article, is to explain the current understanding and management of neonatal anemia, focusing on anemia of prematurity (AOP), and to suggest an algorithm for the approach to its management (Figure 1).
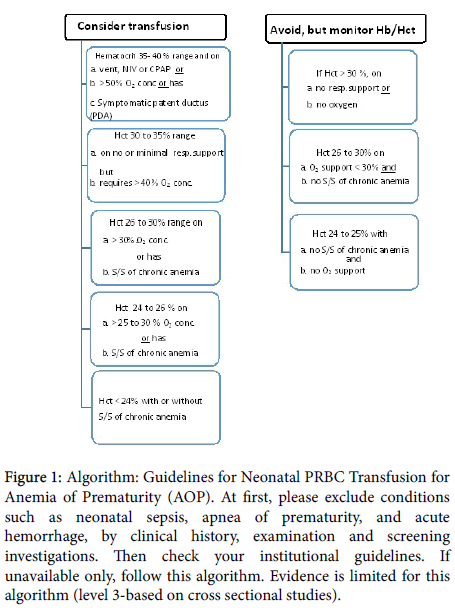
Figure 1: Algorithm: Guidelines for Neonatal PRBC Transfusion for Anemia of Prematurity (AOP). At first, please exclude conditions such as neonatal sepsis, apnea of prematurity, and acute hemorrhage, by clinical history, examination and screening investigations. Then check your institutional guidelines. If unavailable only, follow this algorithm. Evidence is limited for this algorithm (level 3-based on cross sectional studies).
Cord blood hemoglobin (Hb) at term ranges between 14 and 20 g/dl. Following birth, in both term and premature infants, Hb falls in the first 8 to 10 weeks [2]. It can fall from the range of 14.6 to 22.5 g/dl at birth, to 10 to 12 g/dl by 8 to 10 weeks, among infants born at or more than 37 weeks. This fall in the oxygen carrying capacity does not result in clinical signs among term infants, who are otherwise healthy. But, that is not the case in preterm infants, even without much phlebotomy losses. The fall in Hb for this vulnerable population tends to be more pronounced with a nadir of 7 to 8 g/dl, and usually result in clinical signs (symptomatic). This non-pathologic early anemia is referred to as the “physiologic anemia” in term infants, and in preterm infants as “anemia of prematurity” (AOP). In other words, AOP can be considered as an exaggeration of the physiologic anemia in a preterm infant. Interestingly, for the degree of anemia, these infants have inappropriately low reticulocyte count and low Erythropoietin (EPO) levels (decreased production and increased catabolism of EPO) [3,4].
There are two groups of factors that contribute to AOP, a) developmental (physiologic) factors and b) non-developmental (nonphysiologic) factors.
When the infant starts breathing immediately after the delivery, there is a sudden and significant increase in arterial PO2, resulting in saturation of hemoglobin with oxygen. That results in improved oxygen delivery to the tissues, secondary to optimal myocardial contraction. Within the first 7 days of life, it is followed by the declining levels of plasma EPO, reticulocyte count, nucleated RBCs, and bone marrow erythroid precursors. Other developmental factors that contribute to the AOP are a) short Neonatal RBC life span of 60 to 70 days [3], b) increase in adult hemoglobin with a decreased affinity to Oxygen, c) an increase in red cell 2,3-DPG and d) low EPO levels [2] etc.
Non-physiologic/non-developmental factors that can contribute to neonatal anemia, can give an “early start” or exacerbate AOP. These factors can be further divided into two groups, a) congenital anemias such as those resulting from occult blood loss prior to birth, blood loss from obstetric causes, internal hemorrhage such as head bleeds, hemolytic conditions, and decreased RBC production [3], and b) acquired conditions like phlebotomy loss from frequent laboratory (lab) tests, non-lab blood loss, nutritional factors such as iron deficiency, chronic illness, inflammation, and sepsis [2,3].
1. Family history is very important, especially for all anemias that are a) atypical or unexplainable, b) congenital, c) associated with dysmorphic features or malformations, d) associated with bone dysplasia, d) with abnormal peripheral smears, and e) with evidence of hemolysis. In addition to inquiring about specific diseases, it is suggested to obtain family history of G6 PD deficiency, gall stones, splenomegaly, and blood transfusions.
2. Obstetric history [3] is essential to focus on growth restriction, intrauterine infections and the placenta.
3. Physical examination might show pallor, poor weight gain, signs of acute anemia (tachycardia, cardiac failure, and respiratory distress), “blue berry muffin” skin, jaundice, hepatosplenomegaly, edema, cephalo-hematoma, etc. For chronic anemia, the commonly associated signs and symptoms are pallor, increased number of apneic episodes, increased base line respiratory rate, bradycardia, tachycardia, inadequate weight gain despite adequate caloric intake, feeding problems, etc.
4. Laboratory tests include complete blood count (CBC), reticulocyte count, peripheral blood smear, Coombs test and metabolic panel with liver enzymes. As sepsis can mimic any neonatal condition, screening tests for sepsis such as CBC, inflammatory markers like C-reactive protein (CRP) and a blood culture need to be considered in early hemolytic anemia or in an anemic infant with signs of sepsis. Urinary tract infections in a growing preterm infant can present with anemia, jaundice (neonatal cholestasis) and failure to gain weight despite adequate caloric intake.
RBC transfusion: The purpose for PRBC transfusion is to maintain optimal oxygen transport and delivery to the target tissues. Transfusions have the potential to induce immunological responses, and transmit infections. They can also cause volume overload and iron over load. For neonatal transfusions, it is recommended that transfusion products should be leucocyte depleted and irradiated when given to infants weighing less than 1200 grams [5]. Many centers use selected donors to limit donor exposure [3].
Blood loss or shock, are obvious and strong indications for PRBC transfusions, and are needed in order to maintain optimal blood volume and adequate cardiac output. Most of the current transfusion guidelines are not evidence based. Many institutions have designed protocols using a combination of criteria such as infant’s health status, physiological needs, need for oxygen, respiratory support, clinical signs, and laboratory parameters [6]. Two published trials [7,8] showed conflicting results, which added to the physician’s dilemma. The study done by Bell et al. [7] showed worse neurological deficits and neurocognitive scores, with liberal transfusion groups. Kirpalani’s study [8] showed more grade 4 intra-ventricular hemorrhage (IVH), periventricular leukomalacia (PVL) and apneic episodes, with restrictive transfusion group. Currently, two multi center trials are in progress (Transfusion of Premature (TOP) and Effects of Transfusion Thresholds on Neurocognitive Outcome of Extremely Low Birth- Weight Infants (ETTNO), which might provide critical information regarding thresholds for PRBC transfusions [9].
As mentioned earlier, EPO levels in anemic infants could represent a normal physiologic response. The primary site of EPO production is in the liver during the first 3 to 4 months of postnatal age, then it switches to the kidney [3]. Premature delivery does not speed up this transition and the transition happens at 3 to 4 months, starting from 40 weeks post-conceptional age (PCA). In addition to that, the hepatic response to hypoxemia is much less when compared to that of the kidneys. That results in decreased production of EPO, followed by decreased production of RBC precursors. It is also noted that when compared to adults [2], EPO clearance is increased in neonates (another reason for low EPO levels).
Regarding routine administration of EPO for the prevention of AOP, Cochrane reviews [10] concluded, that “early administration of EPO reduces the use of one or more red blood cell transfusions, the volume of red blood cells transfused, and the number of donors and transfusions the infant is exposed”. But, “EPO does not significantly reduce or increase any of many other important adverse outcomes including mortality, IVH and NEC. In view of the limited clinical benefits and the possible increase in ROP (stage greater than/or equal to 3), the administration of early EPO is not recommended”. Darbopoietin, is a long lasting Erythropoietin, and can be administered less frequently [11], showed that infants that were treated with Erythropoietin or Darbopoietin during the neonatal period had better cognitive outcomes and less developmental impairment at 3.5 to 4 years of age, compared with placebo-treated infants.
During the last decade, there seems to be a resurgence of interest in the relation between PRBC transfusions and necrotizing enterocolitis (NEC). In 2006, Mally et al. coined the term “Transfusion Associated Necrotizing Enterocolitis (TANEC)”, to describe the onset of signs and symptoms of necrotizing enterocolitis (NEC), within 48 hours of receiving PRBC transfusion in preterm infants [12]. Many theories were put forth to explain the relation between transfusion related acute gut injury (TRAGI, similar to TANEC) and NEC, ranging from immunologic factors, to physiologic dynamics governing dilation or constriction of the mesenteric arteries during and after the blood transfusion [12,13]. Based on their data, Singh et al. [14] speculated that in preterm infants who are anemic, the ischemic mucosal injury is aggravated by factors associated with RBC transfusions, which might result in NEC. They further speculated that strategies to maintain a certain critical hematocrit might decrease the incidence of NEC.
In their study, they noted that iron supplementation, another therapeutic intervention for treatment of anemia, was associated with lower risk for NEC. Lawrence et al. [12], showed that there is no association between acute rise in hematocrit (blood volume) and onset of TANEC. Evidence for the practice of holding the feedings during the transfusion and also for the use of smaller aliquot transfusions (2 aliquots of 10 ml per kilogram (kg) weight at 6 to 12 hour intervals) versus larger transfusions (20 ml per kg over 3 to 4 hours) is limited and it varies between various NICUs.
If a preterm neonate starts life with a higher hemoglobin and hematocrit (Hb/Hct) at birth, and if the health care team takes precautions and minimizes phlebotomy loss, one can postulate that the nadir at 8 to 10 weeks can be higher (less deep) and may result in less number of PRBC transfusions. Some of the proven strategies for higher Hb/Hct at birth are, delayed cord clamping [15], milking or stripping [16], and drawing all base line lab tests from fetal blood in the placenta [3]. Strategies for controlling phlebotomy losses include, returning the dead space volume after sampling an arterial catheter, use of microcontainers and micro techniques, development and use of noninvasive monitoring, etc [3]. Strict adherence to the institutional transfusion criteria may be beneficial. Use of Iron fortified formulas, and in selected circumstances the use of EPO or Darbepoietin (Dapopoietin) [11] may decrease the number of PRBC transfusions.
Neonatal blood transfusions are frequent, but there are no evidence based transfusion guidelines for neonates. Following the prevention strategies that include using well researched and formulated hospital based transfusion guidelines, may at least decrease the number of PRBC transfusions. Before proceeding with each transfusion, a health care professional needs to assess the risks (known, proven and emerging) and benefits, rather than depending on some arbitrary numbers for the Hb/Hct. Because of physiologically low levels, routine monitoring of reticulocyte count and EPO levels are rarely helpful in taking transfusion decisions. Use of an algorithm approach may help to streamline the therapeutic strategies. Family members and other health care professionals especially nursing staff, need to be included in the decision making team.