Medical & Surgical Urology
Open Access
ISSN: 2168-9857
ISSN: 2168-9857
Review - (2018) Volume 7, Issue 3
Introduction: Urinary and Fecal Control depends on two factors, the first is an inherent, and the second is an acquired. The inherent factor is the presence of an intact sound IUS and IAS. The acquired factor is, through toilet training, having and maintaining high sympathetic tone at the IUS and the IAS. This keeps the sphincters contracted and the urethra and the anal canal empty and closed all the time.
Laceration of the collagen chassis of the IUS leads to its weakness and subsequent stress urinary incontinence (SUI) and/or over active bladder (OAB).
Similarly, lacerations of the collagen chassis of the IAS lead to its weakness and subsequent fecal incontinence (FI).
The lacerations in one/or both sphincters are mainly caused by childbirth trauma (CBT). The pelvic collagen is hormone dependent and drop in the estrogen level causes further weakness of the sphincters.
In men senile prostatic enlargement compress the upper part of the urethra leading to irregular dilatation of the bladder neck allowing some urine to enter the urethra on increases of abdominal pressure causing frequent desire to void. The start of voiding may take some time (hesitancy) because of the effort to open the urethra which is compressed by the enlarged prostate.
Reconstructive surgery: In women the commonest cause of incontinence is traumatic lacerations of the collagen chassis of the IUS and/or the IAS from CBT. Reconstructive surgery is to restore the normal anatomy and it will restore the function. A new operation “urethra-ano-vaginoplasty” is introduced where mending the torn collagen chassis of the IUS and overlapping the anterior vaginal wall flaps over the mended IUS; and mending the torn chassis of the IAS, overlapping the posterior vaginal wall flaps over the mended sphincter, approximate the two levator ani muscles and repair of the perineum is done.
Keywords: IUS-Internal urethral sphincter; IAS-Internal anal sphincter; SUI-Stress urinary incontinence; FI-Fecal incontinence; Collagen; Chassis
The storage organs and the expulsion channels for both the urine and the feces embryo logically develop from the cloaca. They share the same neuro-vascular supply. Voiding and defecation have two stages. The first stage for both excreta is controlled by the pelvic parasympathetic system (S. 2-4). The second stage after toilet training which induces and keeps high sympathetic tone (T.10-L.2) at the internal urethral sphincter (IUS) and the internal anal sphincter (IAS) keeping them contracted and the urethra and the anal canal empty and closed all the time until there is a need/or a desire to evacuate. Both the IUS and the IAS are collagen-muscle tissue cylinder that surrounds the urethra and the anal canal. The IUS extends from the bladder neck to the perineal membrane in both sexes. Sometimes distension of the rectum with flatus and/or feces gives an urgent need to void.
Before toilet training the first stage of micturition is controlled by the pelvic parasympathetic nervous system (S.2-4) (Figures 1-3) [1-6]. The second stage of micturition, after toilet training, is controlled by the thoraco-lumbar sympathetic nervous system (T. 10-L. 2) harmonized by a healthy alert CNS. The acquired behavior is gained by toilet training that keeps high sympathetic tone at the internal urethral sphincter (IUS) and maintains the IUS contracted and the urethra empty and closed all the time until there is a need and/or a desire to void at suitable social circumstances. The IUS is a collagen-muscle tissue cylinder that extends from the bladder neck to the perineal membrane in both sexes. The collagen is a very strong tissue that gives the IUS the strength and constitutes its chassis. The muscle is plain muscle fibers that lie on and intermingle with the collagen chassis. It is innervated with sympathetic nerve fibers from the thoraco-lumbar sympathetic nerve plexus (T10-L2) through inferior hypogastric plexus. The neuro-transmitter of the sympathetic nerve terminals is nor-epinephrine. Patients with nocturnal enuresis suffer from either total absence or partial defiance of the neuro-transmitter norepinephrine. About 10- 15% of patients with nocturnal enuresis suffer as well from diurnal enuresis [3]. Giving patients with nocturnal enuresis ephedrine tablets will cure them. Ephedrine acts on the nervereceptors on the IUS as sympathomimetic and it also acts on the sympathetic nerve endings stimulating them to produce norepinephrine [3].
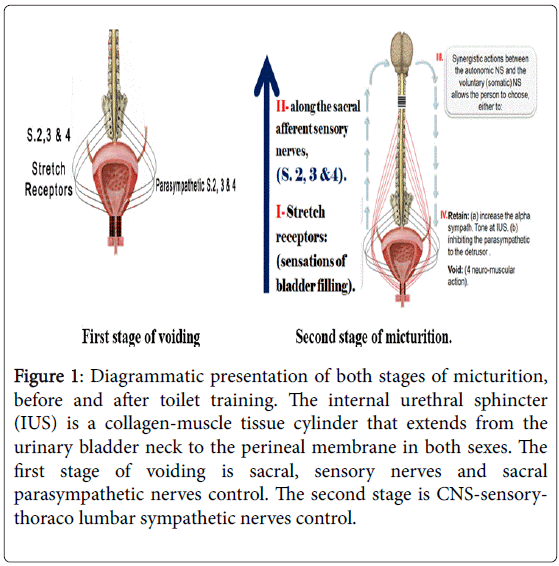
Figure 1: Diagrammatic presentation of both stages of micturition, before and after toilet training. The internal urethral sphincter (IUS) is a collagen-muscle tissue cylinder that extends from the urinary bladder neck to the perineal membrane in both sexes. The first stage of voiding is sacral, sensory nerves and sacral parasympathetic nerves control. The second stage is CNS-sensorythoraco lumbar sympathetic nerves control.
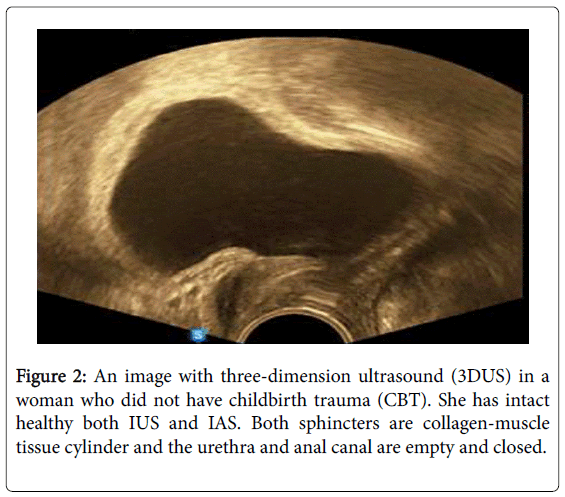
Figure 2: An image with three-dimension ultrasound (3DUS) in a woman who did not have childbirth trauma (CBT). She has intact healthy both IUS and IAS. Both sphincters are collagen-muscle tissue cylinder and the urethra and anal canal are empty and closed.
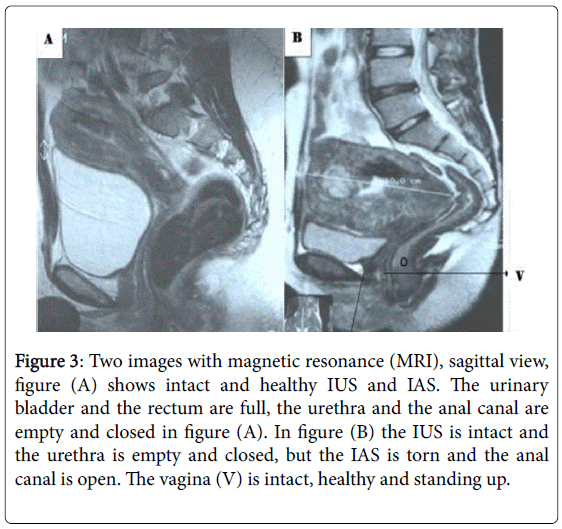
Figure 3: Two images with magnetic resonance (MRI), sagittal view, figure (A) shows intact and healthy IUS and IAS. The urinary bladder and the rectum are full, the urethra and the anal canal are empty and closed in figure (A). In figure (B) the IUS is intact and the urethra is empty and closed, but the IAS is torn and the anal canal is open. The vagina (V) is intact, healthy and standing up.
The IUS in women lies intimately on the anterior vaginal wall. Vaginal delivery (child birth trauma, CBT) especially if the delivery is swift, accelerated, difficult or instrumental will cause invisible damage to the strong collagen chassis of the vagina that leads to its redundancy and its prolapse. It also damages the strong collagen chassis of the IUS leading to its damage, weakness and loss of its ability to act its normal function as a closing tap for the storing reservoir (the urinary bladder UB), It will not be able to resist sudden rise of abdominal pressure allowing some urine to enter the urethra which leaks (stress urinary incontinence SUI) or gives compelling sensations of the desire to void (over-active bladder OAB) (Figures 4-7) [7,8].
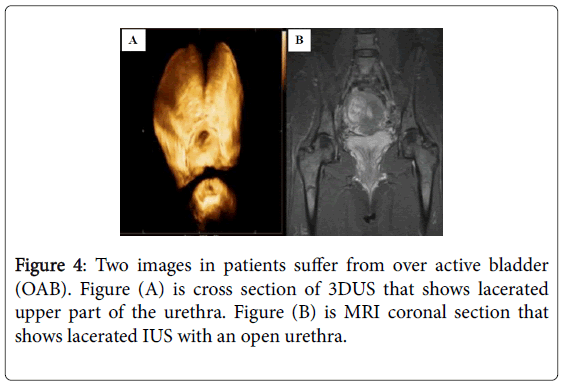
Figure 4: Two images in patients suffer from over active bladder (OAB). Figure (A) is cross section of 3DUS that shows lacerated upper part of the urethra. Figure (B) is MRI coronal section that shows lacerated IUS with an open urethra.
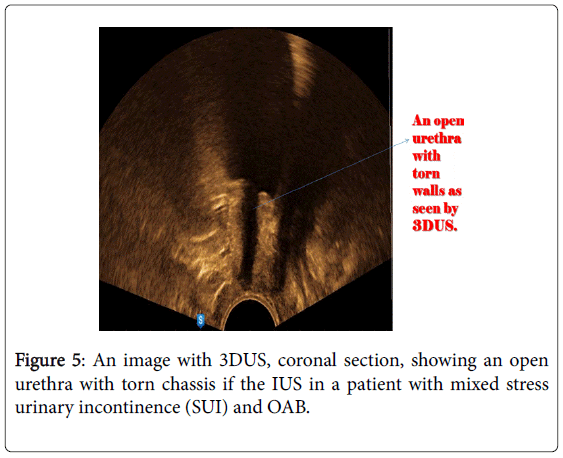
Figure 5: An image with 3DUS, coronal section, showing an open urethra with torn chassis if the IUS in a patient with mixed stress urinary incontinence (SUI) and OAB.
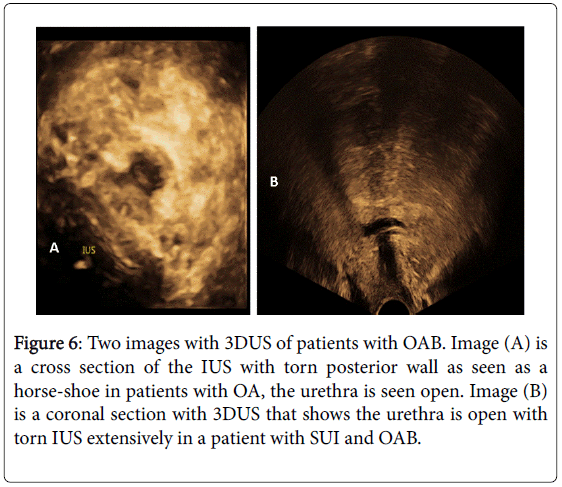
Figure 6: Two images with 3DUS of patients with OAB. Image (A) is a cross section of the IUS with torn posterior wall as seen as a horse-shoe in patients with OA, the urethra is seen open. Image (B) is a coronal section with 3DUS that shows the urethra is open with torn IUS extensively in a patient with SUI and OAB.
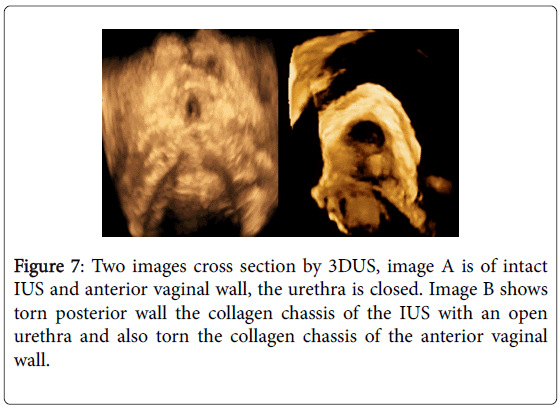
Figure 7: Two images cross section by 3DUS, image A is of intact IUS and anterior vaginal wall, the urethra is closed. Image B shows torn posterior wall the collagen chassis of the IUS with an open urethra and also torn the collagen chassis of the anterior vaginal wall.
In men the prostate surrounds the upper part of the urethra, not its top, so in prostatic hyperplasia and enlargement it will compress and constrict the upper part of the urethra causing irregular dilatation of the bladder neck leading to escape of some urine into the urethra. This will induce the desire to void. Voiding will be difficult and there will be prolonged delay time more than 10 seconds in the start because of the bulk of tissues constricting the urethra. There will be also hesitation, weak stream, interrupted stream and OAB.
Defecation
The rectum is the reservoir for feces (stool and gases) and the anal canal is the tap that controls the passage of the feces (Figures 8 and 9) [4-9]. Sensations of full rectum travel to the spinal cord and higher CNS centers through sensory nerves sacral 2, 3 & 4. The rectum is innervated with the pelvic para-sympathetic exciter nerves (S. 2, 3 & 4). The anal canal is surrounded by two sphincters the internal anal sphincter (IAS) and the external anal sphincter (EAS). The IAS is a collagen-muscle tissue cylinder that surrounds the entire length of the anal canal. The EAS is a voluntary striated muscle has three subdivisions (subcutaneous, superficial and deep parts) surrounds the lower part of the plain involuntary IAS and the lower part of the anal canal. Toilet training initiates and maintains high sympathetic tone (T. 10-L. 2) at the IAS that keeps it contracted all the time and the anal canal empty and closed until there are sensations of desire and/or need to evacuate at suitable social circumstances. The person will inhibit the high sympathetic tone at the IAS, controlled by sound intact high CNS centers, thus relaxing the IAS allowing the passage of feces into the anal canal. The individual will voluntary relax the EAS and the pelvic floor muscles to straighten the acute ano-rectal angle. The person voluntary contracts the abdominal muscles and the diaphragm to increase the abdominal pressure to help in the expulsion. At the end of expulsion, the EAS will contract rhythmically, the deep then the superficial and the subcutaneous parts to expel any fecal residues in the anal canal to leave it empty and closed.
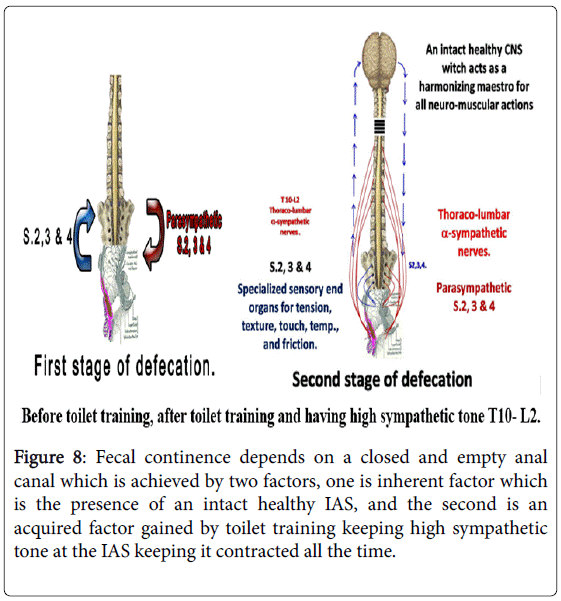
Figure 8: Fecal continence depends on a closed and empty anal canal which is achieved by two factors, one is inherent factor which is the presence of an intact healthy IAS, and the second is an acquired factor gained by toilet training keeping high sympathetic tone at the IAS keeping it contracted all the time.
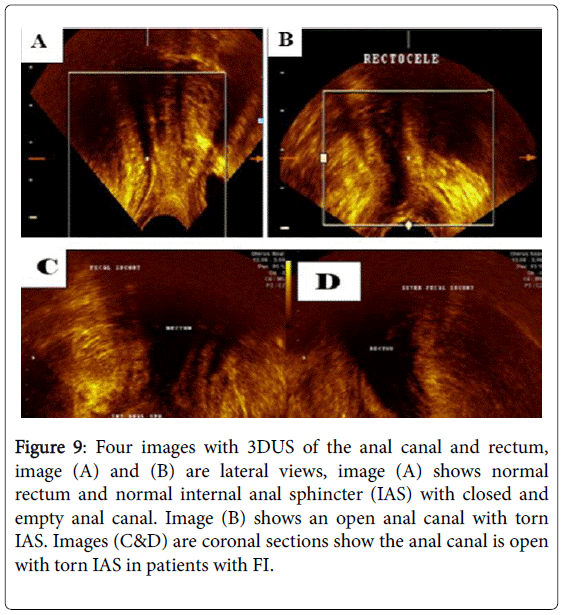
Figure 9: Four images with 3DUS of the anal canal and rectum, image (A) and (B) are lateral views, image (A) shows normal rectum and normal internal anal sphincter (IAS) with closed and empty anal canal. Image (B) shows an open anal canal with torn IAS. Images (C&D) are coronal sections show the anal canal is open with torn IAS in patients with FI.
The anal canal has an intimate relation with the posterior vaginal wall. CBT will cause injury of the collagen chassis of the posterior vaginal wall leading to its redundancy and prolapse. It will also lacerate the collagen chassis of the IAS causing its weakness and thus leads to fecal incontinence (FI). Direct trauma to the IAS e.g. anal intercourse will damage the strong collagen chassis of the IAS and leads to FI.
Diagnosis
Clinically the history and the examination findings are documented. Local pelvic examination in women, on inspection there are two new points to be kept in mind. Normally the external urethral meatus is looking directly forward, if it is seen looking forward and upwards this means there is a loss of posterior vesico-urethral angle. Normally the vagina is directed upwards and backwards from the introitus and is not seen, if the anterior and/or the posterior vaginal walls are seen at the introitus then there is vaginal prolapse. The patient is asked to bear down to estimate the extent of vaginal prolapse. She is also asked to cough to see leakage of urine on stress and its degree Figure 10.
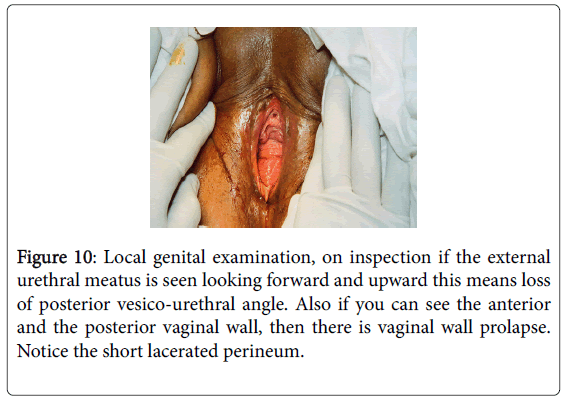
Figure 10: Local genital examination, on inspection if the external urethral meatus is seen looking forward and upward this means loss of posterior vesico-urethral angle. Also if you can see the anterior and the posterior vaginal wall, then there is vaginal wall prolapse. Notice the short lacerated perineum.
Midstream urine is examined and culture and sensitivity test done
Routine laboratory tests and evaluation of the general condition: Urodynamic studies measure the volume, the capacity of the bladder, the pressures in the bladder and the urethra. Structural damage of the collagen chassis of the IUS and/or the IAS are assessed by medical imaging magnetic resonance imaging (MRI) and/or three dimension ultrasound (3DUS). Medical imaging shows the lacerations in the collagen chassis, its extent and its degree.
In women CBT causes lacerations of the collagen chassis of the IUS and the IAS together with the collagen chassis of the vagina (Figures 11-13) [8-10]. Lacerations of the collagen chassis of the vagina leads to its redundancy and vaginal prolapse. Lacerations of the collagen chassis of the IUS and the IAS leads to urinary and fecal incontinence. There are many good reconstructive operations we introduced a new reconstructive operation “urethro-ano-vaginoplasty.” It is a simple vaginal operation we do not use tapes nor any grafts with excellent success rates. We expose the torn collagen chassis of the IUS and mend it with simple interrupted slowly absorbable suture material e.g. vicryl zero. Then we do overlapping of the bisected anterior vaginal wall without excising any part, so we aim at adding extra-support to the mended IUS and narrow the vagina without losing any tissue. Posterior we mend the torn collagen chassis of the IAS, approximate the two levator ani, repair the perineum we called this constructive operation “urethro-ano-vaginoplasty”.
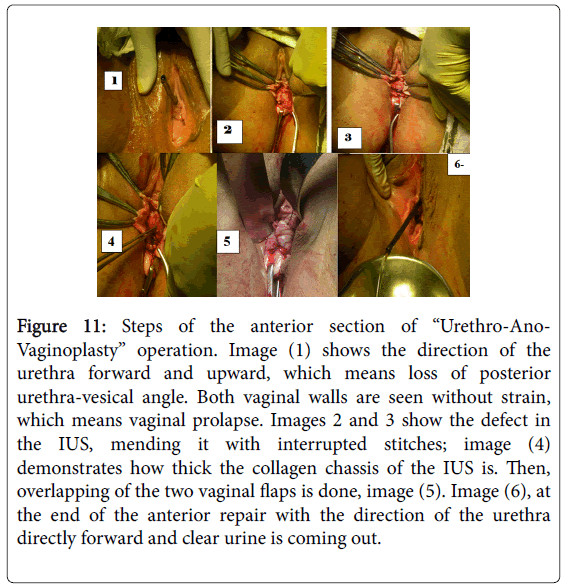
Figure 11: Steps of the anterior section of “Urethro-Ano- Vaginoplasty” operation. Image (1) shows the direction of the urethra forward and upward, which means loss of posterior urethra-vesical angle. Both vaginal walls are seen without strain, which means vaginal prolapse. Images 2 and 3 show the defect in the IUS, mending it with interrupted stitches; image (4) demonstrates how thick the collagen chassis of the IUS is. Then, overlapping of the two vaginal flaps is done, image (5). Image (6), at the end of the anterior repair with the direction of the urethra directly forward and clear urine is coming out.
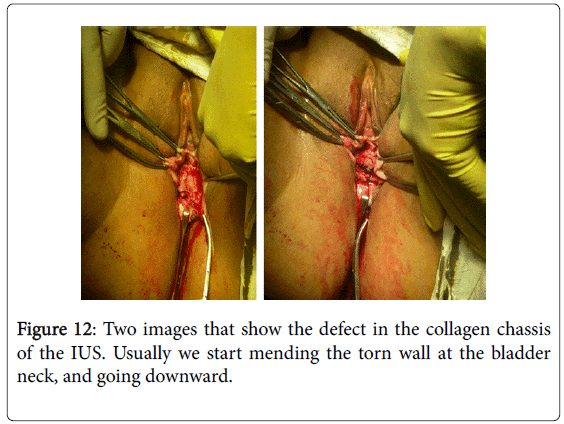
Figure 12: Two images that show the defect in the collagen chassis of the IUS. Usually we start mending the torn wall at the bladder neck, and going downward.
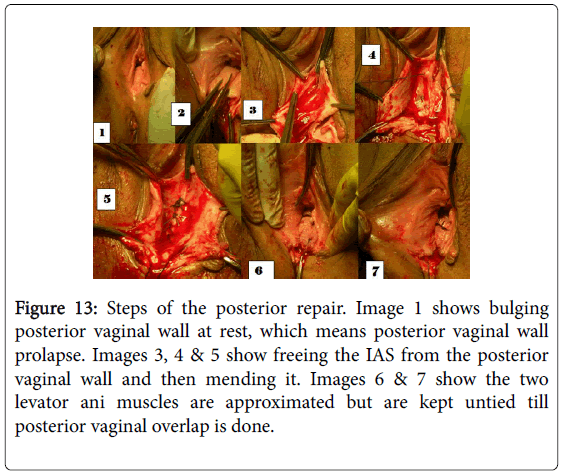
Figure 13: Steps of the posterior repair. Image 1 shows bulging posterior vaginal wall at rest, which means posterior vaginal wall prolapse. Images 3, 4 & 5 show freeing the IAS from the posterior vaginal wall and then mending it. Images 6 & 7 show the two levator ani muscles are approximated but are kept untied till posterior vaginal overlap is done.
Continence of urine depends on healthy intact two arcs a neural arc and a muscular arc. The neural axis, after toilet training consists of an intact alert CNS, intact thoraco-lumbar sympathetic nerves and intact sensory nerves. A healthy intact IUS forms the muscular arc of the good control. Sometimes the terminal sympathetic nerves do not produce nor-epinephrine so the IUS does not contract and there will be involuntary leak of urine (enuresis) [1-15]. The lack of norepinephrine is either partial or total deficiency. Partial lack of norepinephrine which is commoner (about 85% of patients with nocturnal enuresis) leads to nocturnal enuresis. Complete deficiency of norepinephrine leads to day and night enuresis. Growing up and facing every day troubles and annoyances stimulate the sympathetic nervous system and this explains spontaneous annual remission of about ten percent [2].
Structural damage of the IUS caused in women by CBT leads to a weak sphincter which cannot stand sudden rise of abdominal pressure as on coughing, sneezing &/or jumping, will allow some urine to enter the urethra. Urine in the urethra will either cause compelling sensation of desire to void (over active bladder OAB) or escapes (stress urinary incontinence SUI). The woman after feeling wet, there will be reactive sympathetic reflex which increases the existing acquired high sympathetic tone (gained from toilet training) closing the urethra preventing further loss of urine 3. The lacerations affecting the collagen chassis of the IUS get worse near and after menopause, as pelvic collagen gets weaker because it is estrogen dependent.
The sensory nerves for the rectum and the urinary bladder are the same (S. 2, 3 & 4), therefore full rectum with stool &/or flatus may give urgent sensations of desire to void (OAB).
In men senile prostatic enlargement will cause unequal pressure on the upper part of the urethra leading to bizarre dilatation of the urinary bladder neck with escape of some urine into the urethra. This leads to compelling desire to void (OAB), but due to the compressed urethra there will be hesitancy and any annoying factor on voiding will cause interrupted stream. The pothering factor will increase the sympathetic tone closing the urethra.
Structural damage of the IAS will lead to fecal incontinence (FI). The structural damage is caused mainly by CBT, but may be caused by direct injury like anal intercourse or forcing a hard object into the anal canal. After toilet training the anal canal is kept empty and closed all the time. Structural injury of the collagen chassis of the IAS leads to a weak sphincter that cannot stand rises of abdominal pressure and leads to escape of stool &/or flatus (FI). On medical imaging with MRI and/or 3DUS the lacerations in the collagen chassis of the IAS will be seen in addition to an open anal canal in patients with FI. Structural damage is corrected by reconstructive surgery “urethro-anovaginoplasty” we mend the torn collagen chassis of the IUS, IAS and the vagina. Correction of the torn chassis will restore the normal function.