Endocrinology & Metabolic Syndrome
Open Access
ISSN: 2161-1017
ISSN: 2161-1017
Research Article - (2018) Volume 7, Issue 1
Along with all the commonly known rationale; oxidative stress, reactive oxygen species (ROS), growing number of AGEs, accumulation and outbreak of Tridoshas. Throughout year plays decisive role in the development of Diabetes as well as its complications. In the present study, I have discussed about their effective and economical management based on the principles of Ayurveda in the form of distinctive line of treatment which includes Tab.Dibet-all (a poly herbomineral formulation), Tab. Dtox-OD and Tab Glybra. This trio is indistinguishable from allopathy drugs in terms of pharmacology. With so many benefits concealed inside; this line of treatment is having remarkable potential regarding antidibetic, antiglycating, antihyperlipidimic, rejuvinative and preventive/protective activities by the means of breaking cross-links of proteins induced by AGEs, inhibition of AGE formation, blockade of the AGE–RAGE interaction, suppression of RAGE expression and prevention from glycer-AGEs-induced ROS formation ensuring good control over intricate pathology of diabetes and thus protecting diabetics to a higher extent from the complications of diabetes slowly footing towards them. This is the most imperative thing regarding intricate and vague pathology like Diabetes mellitus.
Only the integrated approach towards this gruesome situation will going to help mankind. May this study of ‘Tab. Dibet-all (a poly herbomineral formulation), Tab. Dtox-OD and Tab. Glybra’ with its sovereign effects could serve as a light of hope towards search of ideal treatment of Diabetes mellitus type-2. This can be a supplementary remedy for type-1, hereditary and chronic diabetics also and unquestionably lend a hand to revolutionize the future scenario of these tribulations.
Keywords: Dibet-all (a poly herbomineral formulation); Aadvanced glycation end products (AGEs); Reactive oxygen species (ROS)
The annual spend on account of diabetes treatment in India is pegged at Rs 1.5 lakh crore, 4.7 times the Centre's allocation of Rs 32,000 crore on health and three-fourth of the budgeted service tax collections this fiscal, with experts saying that the cost of treatment of the disease is rising by 20-30% every year. A study by Lancet has expressed concern over the rising cost of insulin, making it virtually unaffordable for a large chunk of patients globally with India, known as the diabetes capital of the world, accounting for 60 million of them. The economic burden of diabetes is high in the country as most patients pay out of-pocket, and due to lack of medical reimbursement. While diabetes rate has increased by around 45% globally, it has jumped 123% in India between 1990 and 2013, according to the Institute for Health Metrics and Evaluation at the University of Washington [1]. People with diabetes have health care costs 2.3 times greater than those without diabetes [2]. Recently, advanced glycation end products (AGEs) accumulation in vivo has been implicated as a major pathogenic process in diabetic omplications, including neuropathy, nephropathy, retinopathy and cataract [3,4] and other health disorders, such as atherosclerosis [5] Alzheimer’s disease [6,7] and normal aging [8,9]. Reactive oxygen species (ROS) formed during the glycation process [10] could cause oxidative stress and damage to tissues, which are also common end points of the above diseases [11,12]. AGE modifications not only change the physicochemical properties of the afflicted molecules but also induce cellular signaling, activation of transcription factors and subsequent gene expression in vitro and in vivo [13]. In diabetes, the glycation of myelin has been found to be increasing as well. AGEs on myelin could trap plasma proteins such as IgG and IgM to elicit further immunological reactions, contributing to both nerve and neuronal demyelination in diabetic neuropathy [14,15]. Furthermore, the glycation and AGE formation occurred on DNA and histones could bring about errors in replication and transcription thereby promoting mutations responsible for diabetic embryopathy [16]. Once formed, AGEs may continue to take part in a covalent crosslink with proteins which are generally stable and long lived, such as collagen and crystallins [17]. Whatever condition it is, the formation of AGEs is influenced by several factors, like sugar concentration, chemical structure, turnover rate of targeted protein and the degree of oxidative stress in the environment [18-21].
This presents an alarming picture and an imperative need to develop effective as well as economical management strategies to halt the rising trend of Diabetes mellitus (DM). It affects almost every system of the human body. Disappointingly, to manage diabetes without side effects is still a challenge [22]. As long as we are not living in harmony with nature and our constitution, we cannot expect ourselves to be really healed. Ayurveda gives us the means.
A 38 year old male patient came to my clinic on 8/06/2017 with chief complaint of obesity (79.1 kg) of height ~ 5’ 7’’ along with allied common complaints of obesity like breathlessness, increased sweating, snoring, inability to cope with sudden physical activity; feeling very tired every day etc. On taking detailed history of the illness, patient was found to have strong positive family history of DM. His father was a patient of uncontrolled DM and eventually died with chronic heart disease at the age of 60. Suspecting him a diabetic; patient was ask to do BSL first which was reported to be 208.79 mg/dl fasting blood sugar (FBS) and 299.25 mg/dl post prandial blood sugar (PPBS). After confirm diagnosis of DM the Ayurvedic treatment (Table 1) was started on 11/06/17 suggesting him to consult an allopathy dibetologist; as patient was bit anxious about BSL reports. [Later on through a phone call I came to know that the antidiabetic drug Tab.Geminor M-1 OD (Metformin (SR) -500 mg + Glimperide-1mg) was started to him from 14/06/2017 by a MD medicine allopathy doctor] Patient was asked for follow up & investigations i.e. FBS and PPBS after 1 month.
| Sr.no | Name of the drug | Dose | Duration |
|---|---|---|---|
| 1 | Tab.Dibet-all- 600 mg (a poly herbomineral formulation) |
2 tablets bid with a cup of lukewarm water 10 min before meal | 4 months |
| 2 | Tab.Dtox-OD- 600 mg (tablet of Terminalia chebula) |
2 tablets early in the morning around 5 to 6 a.m. | 5 months |
| 3 | Tab.Glybra-500 mg (tablet of Glycyrrhiza glabra) |
1 tablet as an adjuvant (Anupaan) to Tab.Dtox-OD | 5 months |
Table 1: Ayurvedic treatment given.
He was asked to avoid sugar completely, to curtail the use of energyrich foods like rice, potatoes, fried foods, bakery and dairy products strictly and to take brisk morning walk of 4 to 6 km daily.
On 7/07/2017 patient came with a report of fasting blood glucose 85.19 mg/dl, post prandial 152.33 mg/dl and weight was 76.2 kg.
On 17/08/17 patient reported to have fasting blood glucose 81.10 mg/dl, post prandial 157.12 mg/dl and weight was 74.7 kg. The dose of Tab.Geminor M-1 was tapered to ½ tablet OD and the Ayurvedic medicine was continued as it is for next 1 month.
On 20/09/17 patient reported to have fasting blood glucose 105.79 mg/dl, post prandial 170.87 mg/dl and weight was 73.8 kg.
All the medicines continued as it is for another one month, but at the time of fourth follow up.
On 10/10/17(10 days before his actual date of follow up) patient make me a phone call in the morning around 8 am and started complaining of giddiness this morning since 5 - 6 am. I just ask him to go for BSL check up first. Patient reported to have fasting blood glucose 76.14 mg/dl, post prandial 127.45 mg/dl. Considering hypoglycemia; Tab. Geminor M-1 withdrawn completely and even the dose of one of the Ayurvedic medicine Tab.Dibet-all was also curtail to half dose (i.e. 1 bid) on a telephonic conversation and patient’s blood glucose was monitored every month to avoid any sudden hike in blood glucose levels.
When patient came to clinic dated 24/10/17; on examination pulse, BP was normal and no other specific cause was found for giddiness clinically and weight was 73 kg.
24/10/17 onwards patient was kept entirely on Ayurvedic medicines with following changes.
Tab.Dibet-all was also withdrawn completely and Tab.Dtox-OD was reduced to half dose i.e. 1 tab. OD and
1) Tab.Glybra was kept as it is for next one month.
On 13/11/17 patient reported to have fasting blood glucose 76.98 mg/dl, post prandial 138.67 mg/dl and weight was 69.6 kg.
From 13/11/17 onwards even the Ayurvedic medicines were stopped absolutely and patient was asked for follow up after one month.
On 14/12/17 patient reported me to have fasting blood glucose 84 mg/dl, post prandial 124 mg/dl on telephone and reports were sent to my clinic by post and weight was 68 kg.
Right now the patient is free from any sort of Antidiabetic medicine; allopathic as well as Ayurvedic. He has been counseled well about the recurrence of disease in absence of proper lifestyle and warned to have exercise, diet management and asked for regular check-up.
Assessment: The patient was examined once in a month on an average. In the present study only the laboratory findings of fasting blood sugar (FBS) and post prandial blood sugar (PPBS) were kept. After completion of 5 months of treatment, the efficacy of the therapy was assessed on the basis of the objective criteria only i.e. BSL & weight.
Discussion
This line of treatment for Diabetes mellitus is designed on the very basic principle i.e. the drugs that work along with endogenous insulin secretion, overcoming resistance, maintaining normal blood sugar level and restoring the liver glycogen level on one hand and also possess antioxidant activity on the other [23] over and above having potential of prevention/protection to a higher extent from complications of Diabetes mellitus to which the diabetics are may going to face in future. With Antidibetic, antiglycating, antihyperlipidimic, rejuvinative and preventive/protective activities by the means of breaking cross-links of proteins induced by AGEs, inhibition of AGE formation, blockade of the AGE–RAGE interaction, suppression of RAGE expression and prevention from glycer-AGEs-induced ROS formation this line of treatment ensurrs good control over intricate pathology of diabetes and thus protecting diabetics to a higher extent from the complications of diabetes slowly footing towards them. This is the most imperative thing regarding intricate and vague pathology like Diabetes mellitus (Tables 2-5).
| Assessment criteria | Parameter | 11-06-2017 | 5/07/17 | 10/08/17 | 10/09/17 | 10/10/17 | 13/11/17 | 14/12/17 |
| Objective | FBS | 208.79 | 85.19 | 81.1 | 105.79 | 76.14 | 76.98 | 84.14 |
| PPBS | 299.25 | 152.33 | 157.12 | 170.87 | 127.45 | 138.67 | 124.57 |
Table 2: Laboratory findings of fasting as well as post prandial blood sugar.
| Assessment criteria | 08/06/17 (when came to my clinic) |
07/07/17 | 17/8/17 | 20/9/17 | 24/10/17 | 13/11/17 | 14/12/17 |
| Weight in kg |
79.1 kg | 76.2 kg | 74.7 kg | 73.8 kg | 73 kg | 70 kg | 68 kg |
Table 3: Change in weight at the time of every follow-up.
| Name & Dose of tablet | 14-06-2017 | 14-06-2017 | From 10/10/17 onwards |
|---|---|---|---|
| Tab.Geminor M-1 (Metformin (SR)-500 mg + Glimperide-1mg) |
1 OD | ½ OD | Stopped |
Table 4A: Tapering dose of allopathic drug.
| Name & Dose of tablet | 11-06-2017 | From 10/10/17 onwards | From 24/10/17 onwards | From 13/11/17 onwards |
|---|---|---|---|---|
| Tab.Dibet-all- 600 mg | 2 bid | 1 bid | Stopped | Stopped |
| Tab.Dtox-OD- 600 mg | 2 OD | Kept as it is | 1 OD | Stopped |
| Tab.Glybra- 500 mg | 1 OD | Kept as it is | Kept as it is | Stopped |
Table 4B: Tapering dose of Ayurvedic medicines.
| Assessment criteria | Parameter | Before treatment | After treatment |
|---|---|---|---|
| Objective | FBS | 208.79 | 84.14 |
| PPBS | 299.25 | 124.57 | |
| Weight | 79.1 kg | 68 kg |
Table 5: Overall effect of therapy after completion of treatment.
There are four classes of Oral hypoglycemic agents (OHAs) in modern medicine frequently used worldwide, they are
a. Sensitizers
Biguanides
Thiazolidinediones (TZD)
b. Secretagogues
- Sulfonylureas
- Nonsulfonylurea secretagogues
c. Drugs like Metformin
d. Alpha glucosidase inhibitors
(Which cannot be given so easily to the patient at a time or for a long duration due to the adverse effects?)
Whereas the Dibet-all is having a ten stage effects at once along with prevention/protection to a higher extent from the complex metabolic derangement of type-2 diabetes mellitus; consequences of which diabetic patients are may going to face in future (Figures 1 and 2).
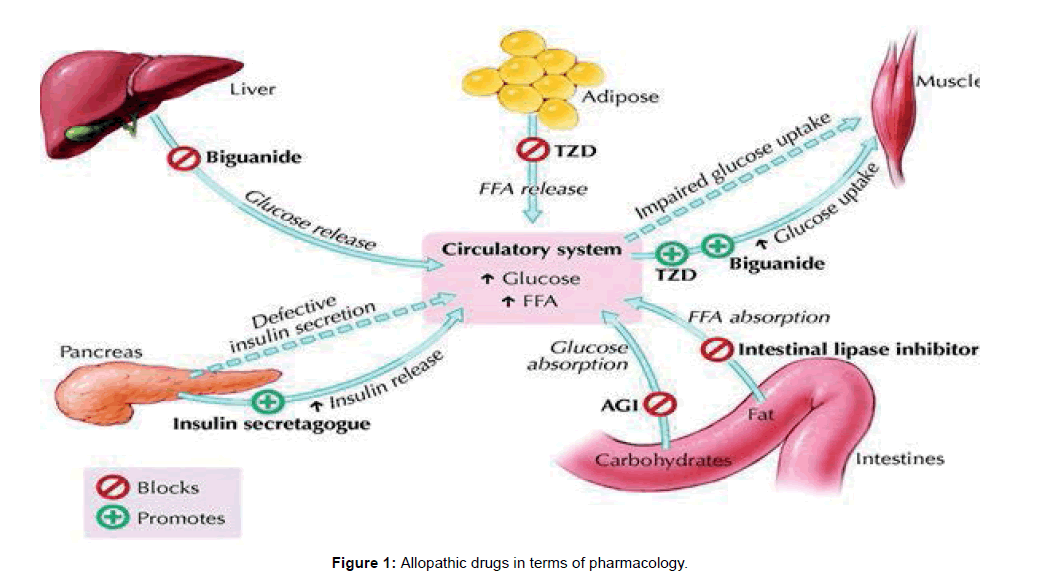
Figure 1: Allopathic drugs in terms of pharmacology.
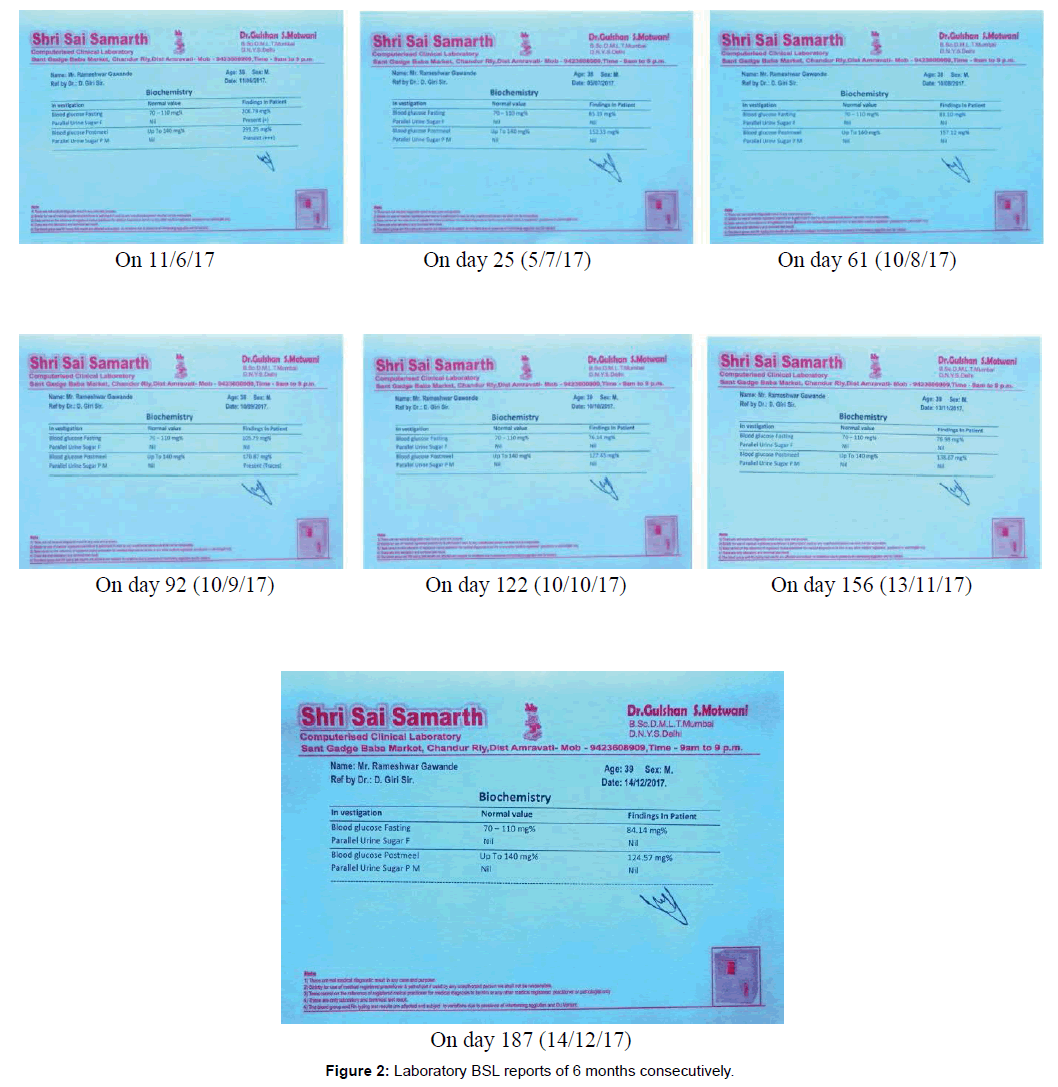
Figure 2: Laboratory BSL reports of 6 months consecutively.
Network pharmacology of these Ayurvedic herbs indistinguishable from allopathic drugs in terms of pharmacology can be understood with the help of following diagram and Table 6.
| (A) | ||
|---|---|---|
| Sr. no. | Actions of Ayurvedic herbs identical to allopathic drugs | Actions of Ayurvedic herbs identical to allopathic drugs |
| 1 | Like Insulin Secretogougue (Increase insulin secretion & mimic insulin) | - Insulin release through K(+)-ATP - Insulinogenic or mimic insulin - Insulinogenic or mimic |
| 2 | Like Alpha Glucosidase inhibitory (Lowers glucose absorption from gut) | α-glucosidase inhibitor and α-amylase inhibitor (starch blockers or Carbohydrate-blockers) |
| 3 | Like TZD + Biguanide (Regularizes muscular glucose uptake) | - Activation of GLUT4 |
| - increase in AMPK signalling | ||
| 4 | Like Biguanide (checks glucose release from liver) | - DPP-4 inhibitory |
| (B) | ||
|---|---|---|
| Sr. no | Action | Possible mechanism of Ayurvedic herbs |
| 5 | AGE inhibitors | Potent inhibitor cross-linking and breaker of collagen cross linking |
| 6 | Anti-hyperlipidemic | Lipid lowering |
| Lipase inhibitors [Lipase inhibitors may affect the amount of fat absorbed, yet they do not block the absorption of a particular type of fat] |
||
| 7 | Protective | Renoprotective β-cells protecting Neuroprotective Cardio protective Hepato protective Anti-cataract Cardio protective activity B.P regulator |
| 8 | Cardio protective activity B.P | Reversal of fatty change in blood vessels and alteration in serum lipid profile. |
| 9 | Feeling of satiety | Acts on TEF (Thermal effect of Food) |
| 10 | (Thermal effect of Food) | (Thermal effect of Food) |
Table 6: (A) Actions of Ayurvedic herbs (from Dibet-all) and their possible mechanism.
(B) Beneficiary effects of Ayurvedic herbs (from Dibet-all) and their possible mechanism.
Plausible role of Tab.Dtox-OD (Tab.of Terminalia chebula) in Diabetes mellitus Chebulagic acid from drug Terminalia chebula is alone potent antidiabetic with its reversible and non-competitive Alpha glucosidase inhibitory effect [24] as well as antihyperlipidemic, tissue glycogen content reducing and in vitro release of insulin [25]. Many reports have alluded to the potential role of AGEs in the development of diabetic complications [26-28]. simultaneously the protective role of Chebulagic acid against AGEs induced endothelial cell dysfunction was also reported [29]. Chebulagic acid is a more potent inhibitor cross-linking and breaker of collagen cross-linking [30] this will unquestionably lend a hand to revolutionize the future scenario of the D.M patients on the subject of microvascular as well as macrovascular complications. Three gallotannins (3-5) from Terminalia fruits acting as enhancers of both PPARα and PPARγ signaling increased insulin stimulated glucose uptake without inducing the adipogenesis [31]. Terminalia chebula is a potential source of natural antioxidants [32-34].
which have free radical scavenging activity and might be used for reducing oxidative stress in diabetes [35]. Upon investigating the protective activity of Terminalia chebula extract against AGE-induced vascular endothelium dysfunction, human umbilical vein endothelial cells (HUVEC) incubated with 100 μg/mL of AGEs had significantly enhanced reactive oxygen species (ROS) formation, whereas the treatment of T. chebula reduced AGE-induced ROS generation [36]. Chebulic acid at both doses (25 and 50 mg/kg) improves biochemical alterations caused by renal ischemia in diabetic rats [37]. Many reports have advocated the nutraceutical potential of Terminalia chebula [38,39]. Thus Tab.Dtox-OD (tab.of Terminalia chebula) might have played a role as Preventive, Curative and Rejuvenative medicine in the present case study.
Beneficiary effects of Tab.Glybra (Tab. of Glycyrrhiza glabra) in Diabetes mellitus
The Glycyrrhizin from drug Glycyrrhiza glabra is quite effective against hyperglycaemia, hyperlipidaemia and associated oxidative stress [40]. Glycyrrhizin improves fatty acid oxidation and glucose homeostasis by elevating levels of peroxisome proliferator activated receptor gamma (PPARgamma) and glucose transporter 4 (GLUT4) proteins [41]. Glycyrrhizin possesses therapeutic potential against hepatocellular damage by reducing oxidative stress, hepatic inflammation and apoptotic cell death [42]. The inhibition of protein glycation and oxidation are the most desirable and beneficiary properties in case of Diabetes mellitus founds in Glycyrrhiza glabra. The entire perception Tab. Dibet-all (a poly herbomineral formulation) Tab.Dtox-OD and Tab. Glybra rewarding all the necessities of treatment regime mentioned above can be a worth for the management of Diabetes mellitus by countering its intricate pathology.
This case study documented substantial reduction in weight and marked antihyperglycemic effect of this treatment regime. With Antidiabetic (Pramehaghna), Antihyperlipidimic (Medohar) and Rejuvinative (Rasayan) properties this therapy might have countered the complex derangements of type-2 Diabetes mellitus. The consorted approach of management explored here may serve as a light of hope towards search of ideal treatment for Diabetes mellitus as well as its complications. This therapy can be a supplementary remedy for type-1, hereditary and chronic diabetes. Further preclinical and clinical studies are warranted to establish the effectiveness, cost-benefits and to explore clinical endpoints.