Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
ISSN: 2167-7948
Research Article - (2015) Volume 4, Issue 4
Background and Purpose: Ultrasound imaging criteria for cervical lymph nodes were set mainly to increase sensitivity. However, unlike the lateral neck compartment, the challenge in the central compartment is the low sensitivity of Ultrasonography. We performed this study to evaluate whether the sensitivity of Ultrasonography could be increased by considering any detected lymph node in the central compartment as malignant.
Methods: Forty one patients with differentiated thyroid cancer underwent dedicated pre-operative Ultrasonography by one radiologist for detection of metastatic lymph nodes in the central compartment. Any lymph node detected was considered positive regardless of Ultrasound morphologic criteria. All patients underwent thyroidectomy with central node dissection (CND), unilateral in 31 and bilateral in 10 cases, based on tumor size and laterality. Ultrasound imaging results were compared to histopathologic results.
Results: The number of true positive cases by Ultrasonography was 13, false negative cases 8, true negative 15 and false positive 5 cases. The sensitivity of US was 61.9%, the specificity 75%, the positive predictive value 72.2% and the negative predictive value 65.2%.
Conclusions: The sensitivity of Ultrasonography for detection of metastatic lymph nodes in the central compartment in patients with DTC may be increased, compared to previously published data, by considering every detected node as positive rather than using the routine criteria for lymph node metastases in other neck levels.
<Keywords: Central compartment; Differentiated thyroid cancer; Lymph node metastases; Sensitivity of Ultrasound imaging
Lymph node metastases occur frequently in patients with differentiated thyroid cancer (DTC). It is estimated that 20-50% of patients with papillary carcinoma will harbour lymph node metastases at the time of diagnosis [1,2].
According to the latest TNM staging of papillary carcinoma, nodal involvement or N stage is divided into N1a (level VI or central compartment) and N1b (other neck levels or lateral compartment) [3]. This subdivision has both therapeutic and prognostic implications, and nodal metastases in the lateral compartment have worse prognosis [4]. Ultrasonography (US) is the first and most widely accepted modality of choice for staging of DTC [5]. The guidelines established by the American Thyroid Association recommend preoperative neck US for all patients with suspected or proved thyroid cancer [6].
The sensitivity of US for detection of nodal metastases in the central compartment was repeatedly reported as lower than that for the lateral compartment. In a recent meta-analysis of studies discussing the role of US in pre-operative diagnosis of nodal metastases, the pooled sensitivity of US for detection of metastatic lymph nodes in the central compartment was only 45% [7]. Most studies used imaging criteria for identification of metastatic nodes in the central compartment that were based on information gained from US imaging of nodes in the lateral compartment. For example, some studies used a size limit of >10 mm for identification of metastases in the central compartment [8,9]. Other studies used several morphologic and Doppler criteria similar to those used for imaging of lateral compartment lymph nodes [5]. However, because benign nodes are very commonly detected in the lateral compartment, those US criteria were primarily set to increase specificity nonetheless at the expense of a slightly lowered sensitivity.
On the other hand, because US scanning of the central compartment is technically difficult, the real limitation appears to be the low sensitivity of US In detection of central compartment lymph nodes, while the specificity was repeatedly reported as excellent. We postulated that the desirable increase in sensitivity of US may be possible if all US imaging criteria for detection of metastatic nodes used in previous studies were totally ignored. We performed this study to evaluate whether considering any detected lymph node in the central compartment as malignant would increase the sensitivity of US with acceptable specificity.
Study Population
This study was approved by our institutional board review and informed consent was obtained from all patients. The study population consisted of consecutive patients between December 2012 and November 2013, with the diagnosis of well differentiated thyroid carcinoma. Patients with primary tumors, and those scheduled for completion thyroidectomy were included. Patients who received radiation or patients with previous nodal dissection were excluded. All patients underwent preoperative ultrasonography followed in less than 1 week by surgery. After exclusion of patients unfit for surgery 41 patients were included in the study.
Ultrasonography
Ultrasonography was performed by one specialized radiologist, with 9 years experience in US, who was blinded to any previous imaging or clinical data and focused only on detection of metastatic central lymph nodes. Ultrasonography was performed using a highresolution phased-array linear transducer (Xario SSA-660A, Toshiba Medical Systems Corporation, Tochigi, Japan). Any detected lymph node in the central compartment was documented. The size, the presence of calcification, cystic degeneration, distorted hilum, rounded morphology, abnormal flow on color Doppler were all recorded. However, according to the purpose of this study, any lymph node detected in the central compartment was considered positive.
Standard of reference
All patients underwent surgical dissection of the central compartment (CND) at the time of thyroidectomy regardless of results of US. In 31 patients, unilateral CND was performed and in 10 patients bilateral CND, based on size and laterality of primary tumor. Surgery was performed by the same surgical team in all cases. The dissected central compartment was sent separately for pathologic evaluation and was examined by experienced pathologists. The number and size of positive lymph nodes in the central compartment was recorded as the gold standard for comparison with US findings.
The sensitivity, specificity, positive predictive value and negative predictive value of US were calculated using the formulas:
Sensitivity =True positives / (True positives + False negatives)
Specificity=True negatives / (True negatives+ False positives)
Positive predictive value= True positives/ (True positives + False positives)
Negative predictive value= True negatives / (True negatives + False negatives)
True positive cases were defined as those positive on both US and pathologic evaluation. False positive cases were defined as those positive on US but not on pathologic evaluation. True negative cases were defined as negative on both US and pathologic evaluation. False negative cases were defined as those negative on US but positive on pathologic evaluation.
Forty one patients were included in the study, 26 females and 15 males, mean age 44 years. Thirty four patients underwent initial thyroidectomy and 7 underwent completion thyroidectomy. The histopathologic type was papillary carcinoma in 32 patients, follicular carcinoma in 7 and medullary carcinoma in 2 patients.
Pathologic evaluation
Metastases were detected by pathologic evaluation in 21 of the 41 patients. They were unilateral in 19 and bilateral in only 2 patients. Number of infiltrated nodes ranged between 1 and 7 nodes per patient per side.
Ultrasonography findings
Ultrasonography revealed positive central compartment lymph nodes in 18 out of 41 patients. In all patients, this was in the ispilateral paratracheal (n=15) or pre-tracheal subsites (n=3).
Sensitivity, specificity, positive predictive value and negative predictive value of Ultrasonography
The number of true positive cases was 13, false negative cases 8, true negative 15 and false positive 5 cases. The sensitivity of US was 61.9%, the specificity 75%, the positive predictive value 72.2% and the negative predictive value 65.2%.
Ultrasound imaging criteria of metastatic and non-metastatic central compartment lymph nodes
In 2 patients with metastatic nodes, 2 central compartment lymph nodes were detected by US, so the number of metastatic individual nodes was 15. The number of non-metastatic nodes was 5. The shortaxis diameter of metastatic nodes ranged between 2 and 16 mm (Figure 1), and of non-metastatic nodes between 4 and 13 mm. Table 1 summarizes the US criteria for metastatic and non-metastatic nodes.
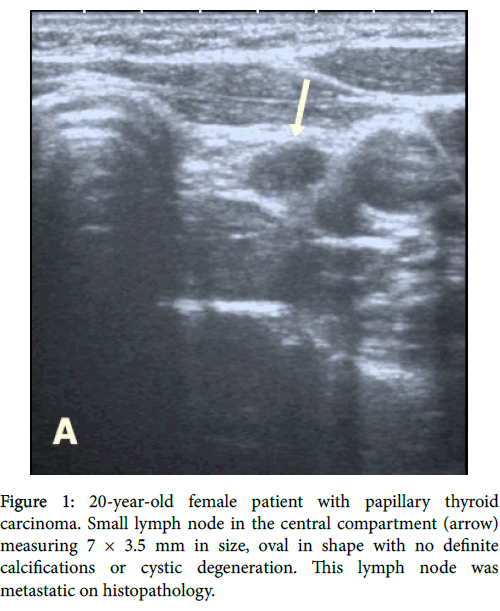
Figure 1: 20-year-old female patient with papillary thyroid carcinoma. Small lymph node in the central compartment (arrow) measuring 7 × 3.5 mm in size, oval in shape with no definite calcifications or cystic degeneration. This lymph node was metastatic on histopathology.
The surgical management is different for lymph nodes in the central and lateral compartments in patients with DTC. Lateral neck dissection is usually performed only as a therapeutic measure based on preoperative diagnosis of nodal metastases in the lateral compartment [6]. On the other hand, prophylactic central compartment lymph node dissection (CND) is performed routinely in many institutions as it improves accuracy of staging, reduces post-operative thyroglobulin level and reduces risk for nodal recurrence thus avoiding re-operation in the central neck [2,10,11]. Therefore, preoperative diagnosis of central lymph node metastases was considered less important and clinically insignificant, as compared to lateral compartment lymph nodes.
However, prophylactic CND is not without disadvantages; it has been associated with prolonged operative time, and potential surgical morbidity; including recurrent laryngeal nerve injury and hypoparathyroidism [12-14]. Moreover, in some studies, prophylactic CND did not result in a clinically relevant reduction of recurrence [14,15]. The American Thyroid Association advises prophylactic CND in advanced cases only, but justifies treatment of small clinically nodenegative tumors without CND, depending on the surgeon's expertise and the balance between safety and risk of local recurrence [6]. While in Medullary thyroid cancer, the American Thyroid Association recommends prophylactic neck dissection with no evidence of neck lymph node metastases by US examination and no evidence of distant metastases.
Other national and international guidelines vary between recommending routine prophylactic CND for all patients, or for high risk only or not recommending prophylactic CND at all [16].
A major factor for the unresolved controversy about prophylactic CND is the low sensitivity of pre-operative assessment which encourages surgeons to perform prophylactic CND despite the added morbidity [16-18]. Central nodes are usually non-palpable [19], and many previous studies have described US as virtually insensitive for detection of central compartment lymph node metastases with sensitivity ranging between 10% and 23% only [5,8,19].
In our study, US had a sensitivity of 62% for detection of nodal metastases in the central compartment, which is higher than many previous studies. In contradistinction to other studies, we deliberately neglected all ultrasound imaging criteria for identifying nodal metastases aiming to increase the sensitivity, and any lymph node detected in the central compartment was considered positive. The specificity of US in our study was 75%, which is still higher than that reported in some previous studies [20].
Other studies with high specificity (97-99%) demonstrated very low sensitivity (11-23%) [5,8,19]. The US morphologic criteria of central lymph nodes in our study such as calcifications, cystic degeneration and abnormal vascularity were only seen with metastatic nodes and hence highly specific, but they were seen in a small proportion of lymph nodes, so that their sensitivity was very low, Table 1. Interestingly, in many patients central nodes were smaller than lateral nodes in the same patient and abnormal morphology was seen in lateral nodes only (Figure 2). We believe that improvement of sensitivity nonetheless with moderate specificity is more beneficial in this clinical scenario. This is because sensitivity of a test is a measure of its ability to correctly identify patients with the disease. Thus a highly sensitive test prevents under-staging of patients and hence is more important for cancer management than a test with low sensitivity but high specificity [21].
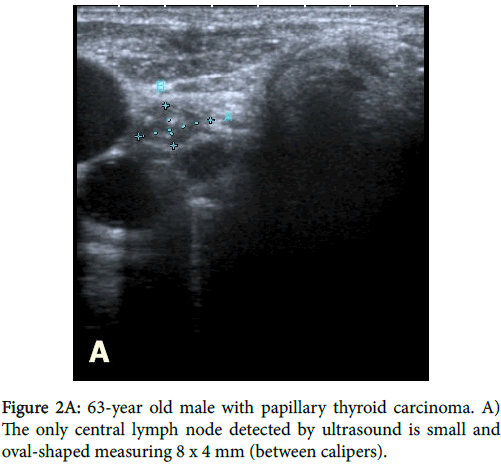
Figure 2A: 63-year old male with papillary thyroid carcinoma. A) The only central lymph node detected by ultrasound is small and oval-shaped measuring 8 x 4 mm (between calipers).
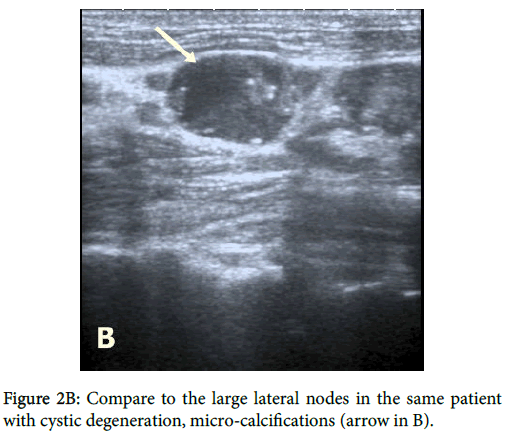
Figure 2B: Compare to the large lateral nodes in the same patient with cystic degeneration, micro-calcifications (arrow in B).
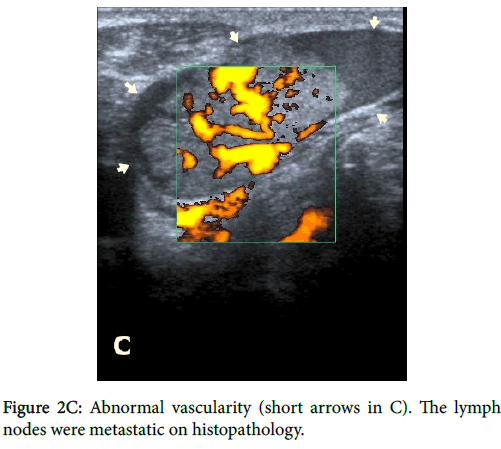
Figure 2C: Abnormal vascularity (short arrows in C). The lymph nodes were metastatic on histopathology.
The previously reported lower accuracy of US in the central compartment compared to the lateral compartment could be attributed to many factors. Firstly, the technical difficulty; where metastatic nodes may be masked by the enlarged thyroid gland and the multifocal nodules and the presence of many surrounding structures with poor acoustic transmission [19,20,22], figure 3. Secondly, it should be noted that the experience of radiologists in US imaging of the central neck compartment is lower than that in the lateral neck. This could be also inferred from the paucity of studies describing imaging of the central compartment lymph nodes in the radiologic literature, compared to the extensive studies on lateral compartment lymph node imaging [20]. We believe that the accuracy of US may be improved with better knowledge of limitations and pitfalls of imaging of the central compartment nodes and with growing experience.
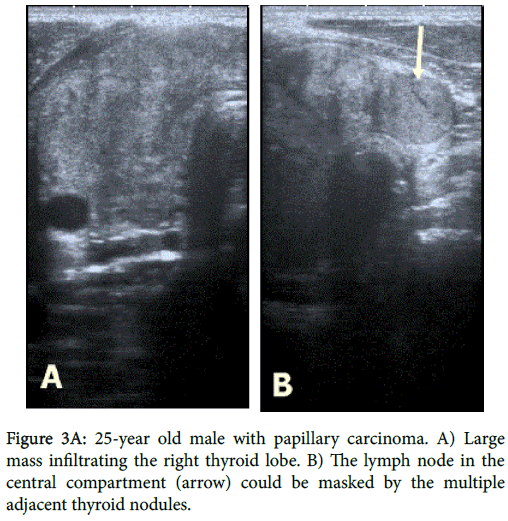
Figure 3A: 25-year old male with papillary carcinoma. A) Large mass infiltrating the right thyrsoid lobe. B) The lymph node in the central compartment (arrow) could be masked by the multiple adjacent thyroid nodules.
A limitation of our study is the relatively small number of patients. However, the prospective and blinded approach allows safe conclusions. Another limitation is that we included patients undergoing both primary and completion surgeries for thyroid carcinoma. However, patients with previous neck dissection or irradiation were excluded.
In conclusion, it is possible to increase the sensitivity of US for detection of metastatic lymph nodes in the central compartment in patients with DTC, compared to previously published data, by considering every detected node as positive rather than using the routine criteria for lymph node metastases in other neck levels. Radiologists should be more informed about limitations and pitfalls of US in the central neck compartment. Further studies are encouraged to validate those results.