Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
ISSN: 2167-7948
Case Report - (2014) Volume 3, Issue 2
Objective To compare the diagnostic accuracy of ultrasound guided fine needle aspiration biopsy (USG-FNAB) versus palpation guided thyroid biopsy. 1.2 Study Design Cross sectional study of patients who underwent thyroidectomy at our institution from May 2012 to June 2013 were included. Final Histopathology was compared with their cytology result whether it was obtained thru ultrasound guided or palpation guided FNAB. Sensitivity, specificity, positive and negative predictive value, accuracy rate and non-diagnostic yield were computed. 1.3 Subjects A total of 207 patients underwent thyroidectomy from May 2012 to June 2013. Seventy eight patients were excluded because of unavailability of cytology result (n=64) and had prior thyroidectomy (n=14). Only 129 patients were included in the study. Each site of the thyroid nodule that underwent FNAB was considered as one case. 1.4 Outcome Ultrasound Guided FNAB group (n=118) has a sensitivity of 78.57%, specificity 91.67%, positive predictive value 86.84%, negative predictive value 85.94%, accuracy rate of 86.2%. Palpation Guided FNAB group (n=57) has a sensitivity of 30.7%, specificity 100%, positive predictive value 100%, negative predictive value 81.25%, accuracy rate of 82.69%. Nondiagnostic yield for USG FNAB is 4% and Palpation FNAB is 12%. 1.5 Conclusion Ultrasound guidance improves sensitivity and overall diagnostic accuracy of FNAB in detecting thyroid malignancy. More importantly, it significantly lessens the non-diagnostic yield by 3x. Furthermore, USG FNAB was able to detect 6 out of 11 cases of micropapillary thyroid cancer translating it into 54.5% sensitivity in detecting micropapillary carcinoma. The improved diagnostic yield and accuracy rate of USG FNAB justify the additional cost of the procedure.
<Keywords: Ultrasound Guided Fine Needle Aspiration Biopsy,Palpation Guided Fine Needle Aspiration Biopsy, Thyroid Malignancy
About 5% of the general population has palpable thyroid nodules and the prevalence increases to 10-55% with the use of ultrasonography [1] and thyroid malignancy occurs in 5-15% of the cases [2]. Generally, nodules more than 1cm has a greater potential to be a clinically significant cancer however non palpable nodules have the same cancer risk as palpable nodules with the same size [3]. Fine needle aspiration biopsy (FNAB) is a common, reliable and inexpensive tool in the management of thyroid nodules. It is considered as the most accurate and cost effective method in the investigation of thyroid nodules [4]. Most palpable thyroid nodules can readily be biopsied without sonographic guidance (palpation-guided FNAB). However, non palpable nodules or complex nodules containing large areas of cystic degeneration are preferably biopsied under sonographic guidance to increase diagnostic accuracy [5,6]. With the use of Ultrasound, it can provide information regarding the location, number, size, echo structure and echogenicity of thyroid nodules. The 2009 American Thyroid Association Management Guideline on Thyroid Nodule recommends fine needle aspiration biopsy (FNAB) for thyroid nodules greater than 0.5cm with high risk history (history of thyroid cancer in one or more first degree relatives, history of external beam radiation as a child, exposure to ionizing radiation during childhood or adolescence; prior hemi-thyroidectomy with discovery of thyroid cancer; FDG activity on PET scanning; MEN2/FMTC associated RET proto-oncogene mutation, calcitonin >100 pg/ ml , multiple endocrine neoplasia, MEN; familial medullary thyroid cancer FMTC) and suspicious sonographic features such as micro-calcifications, hypoechoic, increased nodular vascularity, infiltrative margins, absent halo and taller than wide on transverse view [and suspicious sonographic features such as micro-calcifications, hypoechoic, increased nodular vascularity, infiltrative margins, absent halo and taller than wide on transverse view [7]. At our institution, USG FNAB is most commonly performed procedure to differentiate between benign and malignant condition.]. At our institution, USG FNAB is most commonly performed procedure to differentiate between benign and malignant condition.
Objective
The main objective of the study is to compare the diagnostic accuracy of USG-FNAB versus Palpation guided FNAB in detecting thyroid malignancy.
Specific Objectives:
1. To determine the sensitivity, specificity, positive and negative predictive value of USG-FNAB and Palpation guided FNAB
2. To determine the sensitivity of USG-FNAB in detecting micropapillary thyroid cancer
3. To determine the non-diagnostic or unsatisfactory yield of USG FNAB vs Palpation FNAB
4. To determine the implied risk of malignancy per category of thyroid cytopathology
Study design
This is a cross sectional study.
Study subjects
All patients who underwent thyroidectomy at our institution from May 2012 to June 2013 were eligible in the study. However, patients who do not have cytopathology retrievable at our institution and those who had history of prior thyroidectomy were excluded.
Data collection procedure
Thecensus of admitted patients referred to our Endocrinology consultants from May 2012 to June 2013 who underwent thyroidectomy were retrieved from the stored database at the Diabetes, Thyroid and Endocrine Center. Each site of the thyroid nodule that underwent FNAB was considered as one case. Final histopathology and cytology report were retrieved.An audit of the operative record of patients who underwent USG-FNAB at Diabetes, Thyroid and Endocrine Center (DTEC), St. Luke’s Medical Center and the Ultrasound Department during the period was done. They were categorized as USG-FNAB group. There were a total of 972 patients who underwent USG FNAB during the time period and only 82 (8.4%) patients underwent thyroidectomy. Those patients who do not have operative record retrievable at DTEC but with cytology report were categorized as Palpation guided FNAB group. Cytology reports are the results obtained from fine needle aspiration biopsy of the thyroid whether it was done under ultrasound guidance or palpation guidance.
All USG-FNAB procedures were performed at the Diabetes, Thyroid and Endocrine Center using Ultrasound equipment (Sonosite Micromaxx). A 1% lidocaine (E ML A, Astrazeneca) is administered over the area of interest for local anesthesia for about 15 to 30 minutes. The overlying skin is then cleansed with iodine or alcohol. Two ultrasound radio technicians alternately assisted the Endocrinologist or Surgeons in nodule localization using a 10-MHz transducer during the biopsy. A 23 or 25 gauge needle with a 10 ml plastic syringe was used during the procedure. The aspirated material was then smeared and fixed in 95% ethyl alcohol. All patients who underwent biopsy signed an informed consent. There were no major biopsy related complications noted in the Ultrasound guided biopsy group.Palpation guided FNAB was done in the clinics of the surgeons. The overlying skin was also cleansed with iodine or alcohol. A 23 or 25 gauge needle with a 10 ml plastic syringe was likewise used during the biopsy. The aspirated material is then smeared and fixed in 95% ethyl alcohol. Specimens were then analysed by the 2 consultant cytopathologist at Institute of Pathology, St. Luke’s Medical Center, Quezon City.
Data analysis
Every thyroid FNA was evaluated for adequacy. Inadequate samples are reported as “non-diagnostic” (ND) or “unsatisfactory” (UNS). For a thyroid FNA specimen to be satisfactory for evaluation, atleast 6 groups of benign follicular cells are required, each group composed of at least 10 cells [8,9]. In our institution, since 2013 each FNAB cytology result was subdivided into 6 categories using the 2007 Bethesda System for reporting thyroid cytopathology [10] 1.) Non diagnostic or Unsatisfactory is one in which results dicate cyst fluid only, virtually acellular specimen, other (obscuring blood, clotting artifact, etc). It is also defined as insufficient cytological material. For adequate cytological material, it is further subdivided into the following categories: 2.) Benign is one in which results indicate a benign follicular nodule (adenomatous nodule, colloid nodule), lymphocytic (Hashimoto) thyroiditis, granulomatous (sub-acute) thyroiditis. 3.) A typia of undetermined significance or Follicular lesion of undetermined significance is one in which it is not easily classified into the benign, suspicious or malignant categories. 4.) Follicular Neoplasm or Suspicious for a Follicular Neoplasm is a nodule that might be a follicular carcinoma in about 15 to 30% but most of the cases proves to be hyperplastic proliferations of follicular cells. These comprised the follicular lesions, hurthle lesions, nodular hyperplasia, follicular adenoma. 5.) Suspicious for Malignancy is one in which results indicate suspicious for papillary, medullary, metastatic carcinoma, lymphoma. 6.) Malignant is one in which results indicate papillary thyroid carcinoma, poorly differentiated carcinoma, medullary thyroid carcinoma, undifferentiated (anaplastic) carcinoma, squamous cell carcinoma, carcinoma with mixed features, metastatic carcinoma, non-hodgkin lymphoma. For the data analysis on diagnostic accuracy, the cytologic findings were compared with the final histopathologic findings. Histopathologic examination is the gold standard in the diagnosis of thyroid cancer. It is the tissue examination of the thyroid gland. It is obtained after thyroidectomy. The histopathologic result was classified into two categories: 1.) Malignant is one in which results indicate presence of cancer (papillary, follicular, medullary, anaplastic, hurthle cell carcinoma). 2.) Benign is one in which results benign condition (follicular adenoma, hurthle cell adenoma, thyroiditis and other benign findings).
Statistical analysis
The following were computed to assess the accuracy of FNAB in detecting thyroid malignancy: 1.) Sensitivity (Sn),(TP/[TP+FN]) proportion of patients with thyroid cancer and positive cytologic findings. 2.) Specificity (Sp), (TN/[TN+FP]) proportion of patient without thyroid cancer and negative cytologic findings. 3.) Positivepredictive value (PPV), (TP/[TP+FP]) is the chance that a patient who test positive for the FNAB truly has the disease 4.) Negative predictive value (NPV), (TN/[TN+FN]) is the chance that a patient who test negative for FNAB truly do not have the disease 5.) Accuracy rate (AR), proportion of correct results (true positive and true negative) in relation to all cases studied. Both suspicious for malignancy and malignancy on cytology were considered as “positive FNAB” while the benign category was considered as “negative FNAB”. Thyroid cytology categories such as non-diagnostic or unsatisfactory cytology, atypia of undetermined significance were considered as Benign category. Since follicular neoplas has only 30% of malignancy based on the literature [10], we excluded it in final data analysis.
A total of 207 patients underwent thyroidectomy from May 2012 to June 2013 at St. Luke’s Medical Center. A total of 78 patients were excluded and only 129 patients who underwent Fine needle aspiration biopsy were included in the study. The majority of patients were female with a female to male ratio of 15:1 (121 female: 8 male) with mean age of 45 years old (range 20-75) (Table 1). As can be seen from figure 1 and figure 2, majority of patients from the ultrasound guided FNAB had malignant cytopathology at 32.2% (33/118) compared with palpation guided FNAB at 7% (4/57). The palpation guided FNAB had benign cytopathology at 92.9% (53/57) compared to 67.8% (80/118) of ultrasound guided FNAB. The reason mainly for the higher incidence of malignant cytopathology in the ultrasound guided FNAB is that they were able to choose the thyroid nodule with suspicious ultrasonographic features and that they were able to biopsy the non palpable nodules (nodules that are less than 1 cm and are posteriorly located). Table 2 and table 3 shows the outcome summary of patients who underwent USG-FNAB and Palpation guided FNAB with their thyroid cytopathology category and corresponding final histopathology (Table 4).
| No. of patients who underwent Total Thyroidectomy | 207 |
| No. of excluded patients | 78 |
| No retrievable cytology | 64 |
| Completion Thyroidectomy | 14 |
| Recurrent Multinodular Goiter | 3 |
| Malignancy | 11 |
| No. of patients eligible for the study | 129 |
| Sex | |
| Female [no.(%)] | 121 (93.7%) |
| Male [no.(%)] | 8 (6.2%) |
| Age range | 20-75 (mean age of 45) |
| Ultrasound Guided FNAB | 82 |
| Palpation Guided FNAB | 47 |
Table 1: Demographic Characteristic of the Study.
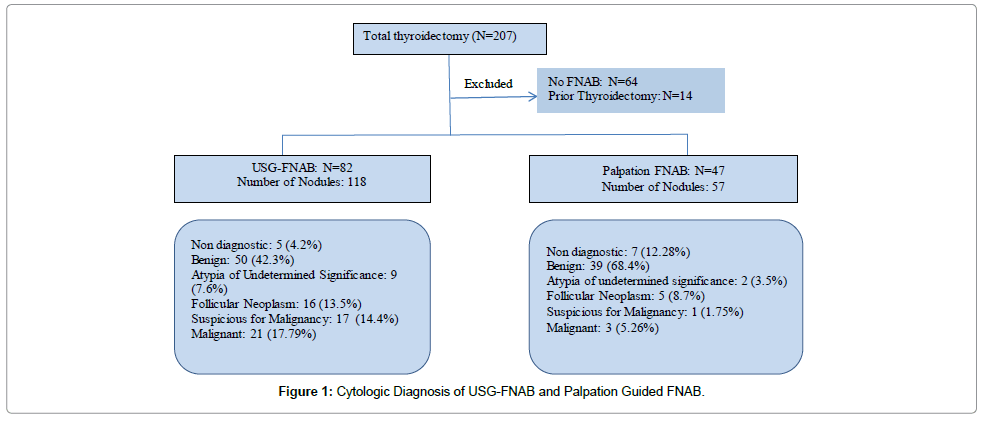
Figure 1: Cytologic Diagnosis of USG-FNAB and Palpation Guided FNAB.
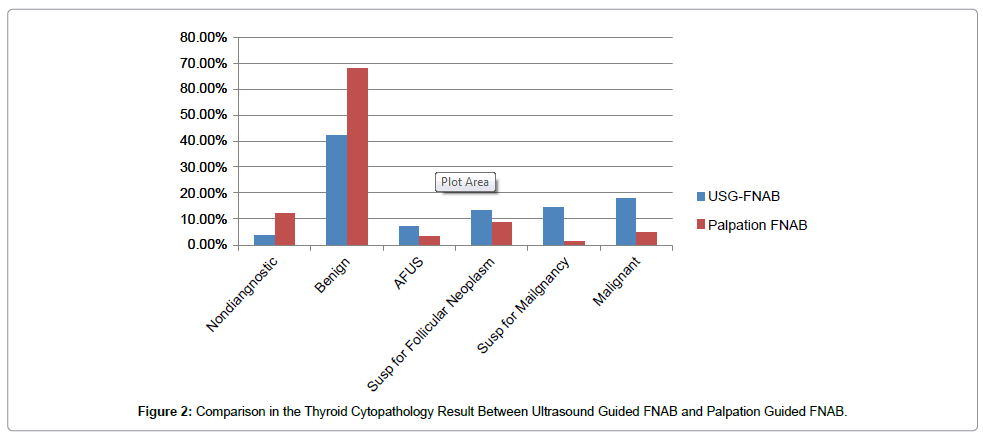
Figure 2: Comparison in the Thyroid Cytopathology Result Between Ultrasound Guided FNAB and Palpation Guided FNAB.
| Thyroid Cytopathology | Benign Histopathology | Malignant Histopathology |
|---|---|---|
| Non Diagnostic or Unsatisfactory (N=5) | N=2 | N=3 |
| Benign (n=50) | N=45 | N=5 |
| Atypia of Undetermined Significance (N=9) | N=8 | N=1 |
| Follicular Neoplasm or Suspicious for a Follicular Lesion (N=16) | N=11 | N=5 |
| Suspicious for Malignancy (N=17) | N=5 | N=12 |
| Malignant (N=21) | N=0 | N= 21 |
Table 2: Outcome Summary of Patients who underwent Ultrasound Guided FNAB (Total=118).
| Thyroid Cytopathology | Benign Histopathology | Malignant Histopathology |
|---|---|---|
| Non diagnostic or Unsatisfactory (N=7) | N=6 | N=1 |
| Benign (N=39) | N=32 | N=7 |
| Atypia of Undetermined Significance (N=2) | N=1 | N=1 |
| Follicular Neoplasm or Suspicious for a Follicular Lesion (N=5) | N=3 | N=2 |
| Suspicious for Malignancy (N=1) | N=0 | N=1 |
| Malignant (N=3) | N=0 | N=3 |
Table 3: Outcome Summary of Patients who underwent Palpation Guided FNAB (Total=57).
| Index | USG FNAB | Palpation FNAB |
|---|---|---|
| True Negative [no.(%)] | 55 | 39 |
| True Positive [no.(%)] | 33 | 4 |
| False Negative [no. (%)] | 9 | 9 |
| False Positive [no. (%)] | 5 | 0 |
| % Sensitivity | 78.57% | 30.77% |
| % Specificity | 91.67% | 100% |
| % Positive Predictive Value | 86.84% | 100% |
| % Negative Predictive Value | 85.94% | 81.25% |
| Accuracy Rate | 86.2% | 82.69% |
Table 4: Shows the index of accuracy rate of Ultrasound guided FNAB and Palpation FNAB (susp for follicular neoplasm not included in data analysis).
Categorizing the tumor size into <1 cm, 1-3 cm >3 cm, computed the index of accuracy rate are as follows (Table 5,6 and 7). For subcentimeter nodules, ultrasound guided FNAB should be used as an initial modality in detecting malignancy. It is highly sensitive, specific and with a high accuracy rate. For tumors 1-3cm and >3cm, USG FNAB has higher sensitivity and accuracy rate compared with palpation FNAB.Histologic examination of all the excised specimens showed 113 benign lesions (64.5%) including adenomatous goiter, hashimoto’s thyroiditis, nodular hyperplasia and 62 malignant lesions (35.4%) including micro Papillary thyroid cancer, papillary thyroid cancer, follicular thyroid cancer, hurthle cell carcinoma, medullary thyroid cancer. Table 8 shows the correlation of cytology and with final histopathology (Table 9).
| Index | USG FNAB | Palpation FNAB (N=0) |
|---|---|---|
| True Negative [no.(%)] | 5 | |
| True Positive [no.(%)] | 11 | |
| False Negative [no. (%)] | 3 | |
| False Positive [no. (%)] | 1 | |
| % Sensitivity | 78.57% | |
| % Specificity | 83.33% | |
| % Positive Predictive Value | 91.67% | |
| % Negative Predictive Value | 62.5% | |
| Accuracy Rate | 80% |
Table 5: Shows the index of accuracy for tumor <1cm.
| Index | USG FNAB | Palpation FNAB |
|---|---|---|
| True Negative [no.(%)] | 40 | 5 |
| True Positive [no.(%)] | 17 | 1 |
| False Negative [no. (%)] | 5 | 4 |
| False Positive [no. (%)] | 3 | 0 |
| % Sensitivity | 77.27% | 20% |
| % Specificity | 93.02% | 100% |
| % Positive Predictive Value | 85% | 100% |
| % Negative Predictive Value | 88.89% | 55.56% |
| Accuracy Rate | 87.6% | 60% |
Table 6: Shows the index of accuracy for tumor 1-3cm.
| Index | USG FNAB | Palpation FNAB (N=0) |
|---|---|---|
| True Negative [no.(%)] | 16 | 31 |
| True Positive [no.(%)] | 3 | 1 |
| False Negative [no. (%)] | 2 | 7 |
| False Positive [no. (%)] | 0 | 0 |
| % Sensitivity | 60% | 12.5% |
| % Specificity | 100% | 100% |
| % Positive Predictive Value | 100% | 100% |
| % Negative Predictive Value | 88.89% | 81.58% |
| Accuracy Rate | 90.4% | 82% |
Table 7: Shows the index of accuracy for tumor>3cm.
| Cytology | MicroPTCA (N=12) | PTCA (N=41) | FTCA (N=7) | Hurthle Ca (N=1) | MTC (N=1) | Benign (N=113) |
|---|---|---|---|---|---|---|
| Cyst Fluid (N=12) | 1 | 2 | 1 | 0 | 0 | 8 |
| Colloid Goiter (n=89) | 4 | 5 | 3 | 0 | 0 | 77 |
| Atypia of undetermined significance (N=11) | 1 | 1 | 0 | 0 | 0 | 9 |
| Follicular Neoplasm (N=21) | 1 | 2 | 3 | 0 | 1 | 14 |
| Susp for PTCA (N=18) | 2 | 10 | 0 | 1 | 0 | 4 |
| PTCA (N=24) | 3 | 21 | 0 | 0 | 0 | 0 |
Table 8: Correlation of Cytology with Final Histopathology.
| Thyroid Cytopathology | Malignant Histopathology | Computed Risk of Malignancy | Risk of Malignancy according to Bethesda System |
|---|---|---|---|
| Non-diagnostic or Unsatisfactory (N=12) | 4/12 | 33% | 1-4 % |
| Benign (N=89) | 12/89 | 13.5% | 0-3 % |
| Atypia of Undetermined Significance (N=11) | 2/11 | 22.2% | 5-15% |
| Follicular Neoplasm or Suspicious for a Follicular Lesion (N=21) | 7/21 | 33.3% | 15-30% |
| Suspicious for Malignancy (N=18) | 13/18 | 72.2% | 60-75% |
| Malignant (N=24) | 24/24 | 100% | 97-99% |
Table 9: Diagnostic Category with their computed risk of malignancy.
Ultrasound guided FNAB compared with palpation guided FNAB has higher sensitivity and higher accuracy rate, 78.57% versus 30.7% and 86.2% versus 82.69% respectively. Use of ultrasound guidance is more preferred than palpation FNAB because it is both highly sensitive and specific. As a diagnostic tool, it should correctly identify the patients with thyroid malignancy and should be able to rule it out. The sensitivity of ultrasound guided FNAB is 2.5 times more than palpation guided FNAB. With the use of ultrasound, the aspirator can locate the nodule of interest and can aspirate the nodule with suspicious sonographic finding for malignancy even if it is subcentimeter. The higher specificity of the palpation guided FNAB is because of the fact that only big nodules that are palpable are the ones aspirated. Large tumor >4 cm increases the risk for malignancy [11]. The computed malignancy rate of USG-FNAB is 27.9% versus 7.6% with palpation FNAB. To our knowledge, this is the first study comparing the diagnostic accuracy of ultrasound guided FNAB and palpation guided FNAB in our country (Table 10). Comparing with previous study of Young et al. [12], the noted slightly higher accuracy rate in their study is attributed to the non inclusion of non-diagnostic and indeterminate results (atypia and follicular neoplasm) with their final data analysis. Have we also excluded in our data analysis the non-diagnostic and indeterminate results (atypical follicular cells of undetermined significance), our accuracy rate would be higher (Table 11). The result of our study is comparable with other previous studies in that ultrasound guided FNAB is more sensitive and accurate with lesser percentage of inadequate specimens compared with palpation guided FNAB. However, because of the short duration of our study, we only had smaller number of patients compared with other studies. We also had lower sensitivity but with higher specificity and accuracy rate.
| Our study (2013) | Young et al. [12] | |
|---|---|---|
| Accuracy Rate | 86.2 | 87.2 |
| Sensitivity | 78.57 | 70.3 |
| Specificity | 91.67 | 92.8 |
| Positive Predictive Value | 86.84 | 76.5 |
| Negative Predictive Value | 85.94 | 90.4 |
Table 10: Comparison of our result with previous study done St. Luke’s Diabetes, Thyroid and Endocrine Center.
| References | Country | Year | Duration of study | Cases operated | Malignancy Rate | Sensitivity | Specificity | Accuracy Rate | Inadequacy |
|---|---|---|---|---|---|---|---|---|---|
| Danese et al. [13] | Italy | 1998 | 15 years | 1075 | 91.8 vs 97.1 | 68.8 vs 70.9 | 72.6 vs 75.9 | 8.7 vs 3.5% | |
| Izquierdoet al. [14] | USA | 2006 | 47 months | 276 | 60.9 vs 80% | 11.2 vs7.1% | |||
| Carmeci et al. [15] | USA | 1998 | 5 years | 497 | 40% vs 59% | 89 vs 100 | 69 vs 100 | 16 vs 7% | |
| Our study | Philippines | 2013 | 1 year | 129 | 7.6% 27.9% |
30.7% vs 78.57% | 100 vs 91.67 | 82.69% vs 86.2% | 12 vs 4% |
Table 11: Comparison of our results with the results of previous studies: Palpation Guided versus Ultrasound guided FNAB.
Non palpable nodules
As a consequence of the increasing application of ultrasound, the prevalence of incidental thyroid nodules in the general population has increased [16,17]. Some clinicians would recommend an USG-FNAB in evaluating non palpable thyroid nodules if they have ultrasound features suggestive of malignancy such as the following: solid, hypoechoic, indistinct margins and with micro-calcifications while some clinicians would just observe and monitor the thyroid nodules. Clinicians also have different opinions regarding management of thyroid micro-carcinomas, some would just do lobectomy while some would recommend total thyroidectomy with radioactive iodine ablation therapy (Table 12). There were a total of 23 sub-centimeter nodules with suspicious sonographic findings that were biopsied. Majority had solid composition with presence of calcification in about 30.4%. Almost half of the patients had malignant cytology. On final histopathology, 34.7% had micro papillary thyroid cancer and 26% had Papillary thyroid cancer.
| Patient Demographics (N=23) | |
|---|---|
| Sex | |
| Female | N=19 (82.6%) |
| Male | N=4 (17.4%) |
| Age | |
| <45 y/o | N=9 (39%) |
| >45 y/o | N=14 (61%) |
| Ultrasound Characteristics | |
| Solid | N=18 (78.26%) |
| Calcification | N=7 (30.4%) |
| Hypoechoic | N=4 (17.3%) |
| Inhomogenous | N=2 (8.69%) |
| Cytologic Diagnosis | |
| Non diagnostic | N= 3 (13%) |
| Benign | N= 5 (21.7%) |
| Atypia of Undetermined Significance | N= 3 (13%) |
| Suspicious for Follicular Neoplasm | N= 1 (4.3%) |
| Suspicious for Malignancy | N= 4 (17.3%) |
| Malignant | N= 7 (30.4%) |
| Final Histopathology | |
| Benign | N=9 (39.1%) |
| Micro PTCA | N=8 (34.7%) |
| PTCA | N=6 (26%) |
Table 12: Demographic Data of Patients with Sub-centimeter Nodules.
Accuracy of ultrasound guided FNAB in detecting micropapillary thyroid carcinoma
In our study, 6 out of 11 cases of micropapillary thyroid carcinoma were correctly diagnosed using the ultrasound. This translates to 54.5% sensitivity in detecting micropapillary thyroid carcinoma. These carcinomas could have been missed using the conventional method since it is non-palpable. The nodules measured from 0.6x0.3x0.3 to 2.2x1x1.7. Among the ultrasound features, 67% were solid and 33% were complex, 33% had calcification, 16% had hypoechogenecity. There was no case of micropapillary thyroid carcinoma diagnosed using the palpation guided FNAB.
Regarding the non-diagnostic yield, use of ultrasound guidance lessen the risk of non-diagnostic result by as much as 3 times. This is because the ultrasound can locate the solid component in a complex nodule while in the blind FNAB, the components of the complex nodule cannot be identified hence, specimen may consist only of cyst fluid. The 4 nodules with inadequate specimen in the ultrasound guided biopsy group was done by residents in training. The nodules measured from 1.1x0.8x0.8 to 5x3.4x4.5. The experience of the aspirator plays role in the adequacy of the specimen. The one nodule done by the consultant was done only with one pass and the nodule measured only 0.6x0.5x0.6. Hence, we recommend increasing the number of passes to more than 1. Comparing with previous study by Young et al. [12] with our present study the rate of inadequate specimen using ultrasound guidance at St. Luke’s Diabetes, Thyroid and Endocrine Center decreased from 9.7% to 4.2%. This is mainly because of the increased number of passes and the improved skills of the aspirator over time.Comparing with the inadequate yield of palpation guided FNAB, 5 out of the 7 nodules were done by the residents in training (71%) and the nodule size ranges from 3.8x2.2x4.7 to 12.1x7.8x14 (mean average volume of 271). The use of palpation guided biopsy should not be only dependent on the nodule size but also on the characteristic of the nodule whether it is purely solid or complex. If the nodule is complex, there is chance that the aspirated material would only be cystic fluid or blood. Unlike if the nodule size is purely solid, the risk of non-diagnostic yield is very low. All of the nodules were complex so even though they were big and palpable, they still yielded non-diagnostic result.
Cost and benefit
The expected cost of Ultrasound Guided FNAB in our institution is roughly 12,000 pesos and it is 8,500 pesos for palpation guided FNAB alone. At initial look, palpation guided FNAB is cheaper than ultrasound guided FNAB but considering the fact that without the use of ultrasound, the non-diagnostic yield for palpation FNAB alone was 3x higher requiring patient to undergo a repeat FNAB thus incurring more cost. In this situation, ultrasound guided FNAB is considered a diagnostic of choice when a fine needle aspiration biopsy returns an inconclusive diagnosis because of cytologic ambiguity or paucity of specimen. Our conclusion is the same as with the study of Khalid et al. [18] the use of ultrasound guided FNAB as the initial modality for tissue biopsy of a thyroid nodule is more effective than palpation FNAB at a justified additional cost.
Implied risk of malignancy
Based on our results, the “benign” cytology has a higher risk of malignancy compared with the Americans. This translates to a higher incidence of thyroid malignancy among Filipinos probably due to genetic predisposition [19] and environmental influences [20]. For unsatisfactory or non-diagnostic results, it is better to repeat FNA with Ultrasound guidance. In our study, the Ultrasound features of the non-diagnostic specimen that had Papillary Thyroid Cancer on final histopathology showed the nodule to be solid with calcification with measurement of 0.7cm to 3cm. The American Thyroid Association recommends close observation or surgical excision for partially cystic nodules that yield non-diagnostic aspirates and surgery should be considered if the cytologically non-diagnostic nodule is solid [7].
A benign cytology should be clinically followed up and if they have suspicious ultrasonographic features with a size of >4 cm, we recommend thyroidectomy because the incidence of malignancy is higher compared with the literature at 13.5% versus 0-3%. In our study, patients who had false negative results are the ones with solid nodule, >1cm, some with calcification (Table 13). Because of the higher incidence of malignancy among patients with atypia of undetermined significance at 22.2% compared with 5-15% at the literature we recommend repeat FNA and surgical lobectomy for the suspicious for follicular neoplasm. Certain clinical features such as male sex, nodule >4 cm [11], older patient age (>45 years) [21] can improve the diagnostic accuracy for malignancy for patients with atypia and follicular neoplasm but the overall predictive values are still low. Our computed risk of malignancy for suspicious for malignancy and malignant is the same as with the literature hence we recommend total thyroidectomy for these categories.
| Ultrasound Guided FNAB (N=5) | Palpation Guided FNAB (N=7) | |
|---|---|---|
| Sex Female Male |
4 (80%) 1 (20%) |
7 (100%) 0 |
| Age <45 y/o >45 y/o |
1 (20%) 4 (80%) |
6 (85.7%) 1 (14.2%) |
| Tumor Size <1cm 1-2cm 2-3cm 3-4cm >4cm |
1 (20%) 2 (40%) 0 0 2 (40%) |
0 2 (28.5%) 2 (28.5%) 0 3 (42.8%) |
| UltrasoundCharacteristic SolidComplex Calcification |
5 (100%) 0 2 (40%) |
4 (57.1%) 3 (42.8%) 2 (28.5%) |
Table 13: Demographic Profile of False Negatives (Benign Cytology with Malignant Histopathology).
US guidance for FNA is recommended for those nodules that are non-palpable, predominantly cystic posteriorly located, multinodular goiter and hypo functioning nodules. Palpation guided FNAB still has a role in big, solid, solitary nodule.USG FNAB has higher accuracy in detecting thyroid malignancy compared with palpation guided FNAB. It has 2.5x more sensitivity in detecting thyroid cancers. USG FNAB was able to detect 6 out of 11 cases of micropapillary thyroid cancer which could have been missed by palpation guided FNAB. USG FNAB lessens the risk of on diagnostic yield by 3x.
Ultrasound guidance improves sensitivity and improves overall diagnostic accuracy of FNAB in detecting thyroid malignancy. More importantly, it significantly lessens the non-diagnostic yield by 3x. It also has 54.5% sensitivity in detecting micropapillary thyroid cancer. The improved diagnostic yield and accuracy justify the additional cost of the procedure.
The authors would like to thank the help of Dr. Oliver Allan Dampil and Dr. Maribel Develos for the data analysis.