Medical & Surgical Urology
Open Access
ISSN: 2168-9857
ISSN: 2168-9857
Case Report - (2018) Volume 7, Issue 4
Keywords: Female urethra carcinoma; Surgery; Chemotherapy
Primary cancer of the female urethra is rare. It accounts for 1% of cancers, with an incidence of less than ten cases per one million [1,2]. It is often symptomatic and palpable. In 50% of cases, the diagnosis is made at a metastatic stage [3]. There are several pathotological features each of them corresponding to a specific therapeutic strategy [4]. The treatment is based on surgery and radiotherapy. We report two cases of urethral cancer in black female.
Case 1
A 70-year-old woman with no pathological history initially consulted for dysuria and initial hematuria, and ultimately urinary retention. The physical examination revealed a painful mass, located on the anterior surface of the vagina and bleeding at palpation. There was no inguinal lymphadenopathy. The patient underwent a biopsy of the mass and pathology showed a moderately differentiated and infiltrating adenocarcinoma of the urethra. Cystoscopy and thoracoabdominal CT scan found an invasion of the bladder trigone. The patient underwent an anterior pelvectomy and ileal conduit for urinary diversion. The surgical resection was complete (R0) and the patient was staged pT3N0M0 (Figures 1 and 2). But postoperatively she refused to do chemotherapy or radiotherapy in medical oncology center.
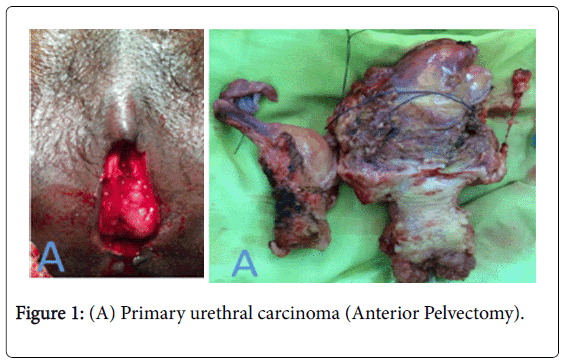
Figure 1: (A) Primary urethral carcinoma (Anterior Pelvectomy).
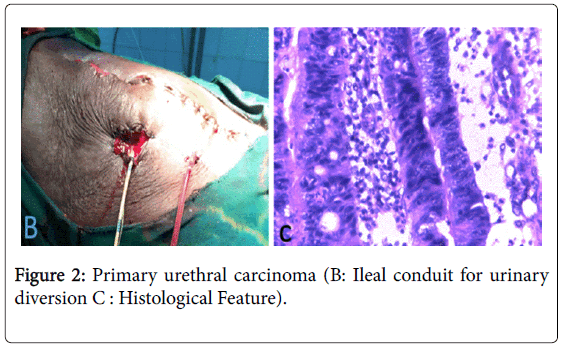
Figure 2: Primary urethral carcinoma (B: Ileal conduit for urinary diversion C : Histological Feature).
Case 2
A 27-year-old patient, two gravidities and two parities was referred in urology for the treatment of total hematuria and finally urinary retention with vulvovaginal bleeding. Examination revealed a painful mass located at the anterior surface of the vagina. There was no inguinal lymphadepathy. Examination under general anesthesia and urethrocystoscopy revealed a urethral fistula. Pathology of the biopsy revealed urothelial carcinoma. Urethrocystoscopy and thoracoabdominopelvic CT scan showed an invasion of the bladder trigone. The patient underwent anterior pelvectomy and an ileal conduit. The surgical resection was complete (R0) and the patient was staged pT3N0M0. Adjuvant chemotherapy was performed in a medical oncology center. After one year follow up the patient was doing well with no local recurrence.
Cancer of the female urethra is an extremely rare disease. It accounts for 0.02% of all cancers in women [2]. The average age at diagnosis is 50 years-old [1]. Multiple risk factors are considered, are identified in favor of female urethral carcinoma: chronic irritations, recurrent urinary tract infections, urethral diverticula and proliferative lesions such as papilloma, adenoma, polyp, or leukoplakia, sexual activity [1-6]. In our cases, none of those risk factors were found.
Squamous cell carcinoma develops most often on the distal urethra. Urothelial carcinomas affect the proximal urethra and the bladder neck. Adenocarcinoma, more common in women, appears to develop from existing urethral diverticula and occurs on metaplasia or periurethral glands [4]. Other histological types are rare: melanoma, carcinoid tumors or small cell carcinoma, adenosquamous carcinomas, adenoid cystic carcinoma, neuroendocrine carcinomas and cloacogen carcinomas [4].
Many prognosis factors of primary urethral carcinomas have been identified: advanced age (>65 years), black race, histological type, anatomical localization, local extension, stage, grade, nodal involvement and metastasis [3-5]. Five-year survival is 89% for tumors less than 2 cm, 36% for tumors 2-4 cm, and 19% for tumors larger than 4 cm. Squamous cell carcinomas appear to be of better prognoses than urothelial carcinomas. Adenocarcinoma has a very poor prognosis with a 5-year specific survival of 0% [3-7]. Five-year survival was 46%, with 89% survival for low grade and 33% for high grade. The poor prognosis of advanced diseases is associated with the invasion of neighboring organs, the impossibility of obtaining a complete surgical resection and the presence of lymphadenopathies [4].
Clinical symptoms are present in 94% of cases [3-10]. Obstructive symptoms are more consistent than urinary irritative symptoms [3,4]. Hematuria leads to diagnosis [4].
Clinical examination most often reveals a urethral mass, an induration of the anterior vaginal wall [3,10]. Urethral fistula must be diagnosed [2]. In 30% of cases, lymphadenopathy is present especially in the inguinal area. The lesion is most often a palpated mass in the form of friable induration on the anterior surface of the vagina [4]. Initial clinical examination will be completed by an examination under anesthesia and will be coupled with urethrocystoscopy and biopsies that will confirm the diagnosis. Clinical examination under general anesthesia associated with urethrocystoscopy and biopsies confirm the diagnosis [3]. CT and especially MRI are very helpful for the staging. MRI is very appropriate to establish the loco-regional extent of disease at diagnosis.
Single modality treatment fails in most cases of locally advanced tumors. The five-year survival rate is below 20% and the local recurrence rate is 66% [4]. Extensive surgery shows only an 11%–21% 5-year survival rate in women who underwent a pelvic exenteration [7].
For proximal or extensive tumors, an association between radiotherapy and surgery appears to be beneficial, and in the case of distal localized lesion, a single enlarged excision or interstitial brachytherapy could be performed [11-14]. Chemotherapy is recommended for proximal tumors with the M-VAC combination or Carboplatin and Gemcitabine combination, similar to the chemotherapies used for urothelial tumors. Squamous cell carcinomas are sensitive to the combination of 5-FU and cisplatin [3,13,14].
For distal, superficial and well-localized distal urethral cancers, a simple circumferential excision of the urethra associated with excision of the adjacent part of the anterior vaginal area is sufficient and verifies that the limits of resection are healthy at examination. For proximal urethral cancers or invasive urethral lesions, anterior pelvic anesthesia is recommended as first-line therapy [4,12]: Extensive resection is essential, including urethrocystectomy, colo-hysterectomy, and a widewalled resection of anterior vagina. The perineal incision should be wider, the labia majora retracted and the incision made in front of the clitoris. The incision continues downwards with the labia minora and joins the vaginal incision initiated by the suprapubic approach. Pelvic ilio-obturator dissection should be systematic in the event of proximal injury. For distal tumors, inguinal dissection is performed only in patients with palpable lymphadenopathy [4]. Radiotherapy alone can be as effective as surgery in small lesions of the distal urethra. Irradiation can be carried out either by brachytherapy with iridium 192 or by external irradiation delivering 50 to 65 grays [14].
In Africa, female urethral carcinomas are very rare. The diagnosis is established by pathology examination of biopsy. Anterior pelvectomy and ileal conduit is a viable option that can be completed by chemotherapy or radiotherapy.
Written informed consent was obtained from the patients for publication of this case report and any accompanying images.
None