Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
ISSN: 2167-7948
Research Article - (2016) Volume 5, Issue 3
Background: Disease of the thyroid in Sub-Saharan Africa mainly present as multinodular goiter (MNG). Our aim was to standardize indications for total thyroidectomy (TT) after our experience in the major non-governmental hospital of North Uganda. Methods: We included patients submitted to thyroid surgery during 5 camps held by a team of Italian ENT surgeons from April 2012 to December 2015 at Saint Mary’s hospital Lacor, Uganda, for single lobe macronodules or MNGs. From an initial pool of 218, we selected 142 (65.14%) patients: 137 (96.48%) were submitted to thyroidectomy. Results: We performed 84 lobectomies (61.3%), 13 loboisthmusectomies (9.49%), 25 sub-total thyroidectomies (18.25%), and 15 TTs (10.95%). We observed 5 postoperative complications and 1 intraoperative death. TTs increased in number compared with partial thyroidectomies (p=0.02) and STTs (p<0.0001). Conclusions: Partial and sub-total thyroidectomies were the primary procedures, however TT was confirmed to be feasibile for treating MNG in a rural area.
<Keywords: Multinodular goiter, Total thyroidectomy, Partial thyroidectomy, North Uganda, Complications
Thyroid disorders are commonly encountered in Africa and often arise from environmental and nutritional factors [1], representing a severe public health problem in several countries of the sub-Saharan area, such as Uganda. In these geographic regions, the lack of iodine in the food and drink is the primary cause of thyroid gland disease, in which goiters represent the most common manifestations [2]. The universal salt iodination program was introduced with the aim of alleviating this deficiency; however, endemic goiter in Africa still presents a wide variability, reaching a prevalence of 60.2% in Uganda [3] These values remain high despite the widespread introduction of iodine, which may be due to the possible synergic role played by other goitrogens, which are substances that can interfere with iodine uptake [4,5].
Goiters can reach a significant volume and cause neck compression symptoms such as dysphagia and acute respiratory distress in combination with other mild symptoms, such as shortness of breath, pain during swallowing and aesthetic issues. However, in a low- and middle-income country (LMIC) the selection of the type of thyroid surgery needs to be based on several factors and may not always follow the same indications as for developed countries [6]. Infact, the availability of some facilities during in-hospital stays or the immediate postoperative period are major concerns, and indications for a total thyroidectomy (TT) in LMICs are still debated; many authors agree that it should be performed only in selected cases due to the scarce thyroxine supply, increased risk of postoperative complications and erratic follow-up [7].
In this study, we conducted a prospective analysis of our thyroid surgical experience in a non-governmental hospital of North Uganda between 2012 and 2015. Our main purpose was to identify the indications for different types of thyroid surgery in these areas. In addition, we gradually introduced the TT through a careful selection of patients.
This prospective study includes patients admitted to surgery for thyroid disease at St. Mary’s Hospital of Lacor (SML), a few kilometers from Gulu, the main town in North Uganda. The study population was collected during 5 different time periods, each lasting two to three weeks, from April 2012 to December 2015. The missions were supported by “Centro Salute Globale”, Tuscany Region, Italy.
SML is the major non-governmental hospital in North Uganda and East Africa, with 482 beds and 3 peripheral health centers. SML is also a University teaching sitefor the Government University of Gulu Faculty of Medicine. Almost all of the patients belong to the Acholi and Lango tribes; they come from the Gulu District and its suburbs (more than 90%), and most of them live and work in a rural setting (Figure 1).
Figure 1: Geographic area of the Gulu District.
The thyroid surgical team was composed of 2 experienced ENT surgeons, 1 assisting ENT resident, 1 experienced anesthesiologist and 1 anesthesiology resident from 2 of the major hospitals of middle Italy, Florence and Arezzo.
The day before the start of the surgical camp, the entire team visited each patient who was referred to it by the medical doctors of SML. A recent blood test, including the thyroid hormonal status (fT3, fT4, TSH), a chest X-ray and a recent ultrasound scan of the neck were also available. Fine-needle aspiration cytology (FNAC) was performed after our request in 2 cases of a high suspicion of thyroid cancer. Hence, indications for a partial, sub-total or total thyroidectomy depended only on the unilaterality vs the bilaterality of the disease. Giant goiters that extended to the mandibular arch and the mastoid tips were indicated exclusively for a TT.
Partial thyroidectomies included an isthmusectomy or a loboisthmusectomy, consisting of the resection of one thyroid lobe with or without the thyroid isthmus. A typical sub-total thyroidectomy is defined as the surgical removal of the thyroid gland while preserving the portion of the gland nearest to the suspensory ligament and tracheoesophageal groove [8]. In our camps, we preferred to perform an atypical sub-total resection of the thyroid: we routinely leave a larger portion of the gland because of the abnormal size of the nodules and the difficulty of sparing the residual healthy thyroid parenchyma.
All of the operations were performed under general anesthesia. We used propofol to induce the anesthesia and halothane as inhaled general anesthetic gas to deepen the anesthesia, to intubate and maintain the general anesthesia. The only other available tool was a 1- lead electrocardiograph, while the intraoperative monitoring of blood pressure was not possible. We did not administer prophylactic antibiotic therapy. After the operation, the patients spent one night in the intensive care unit. A neck drain was kept in place for 2 to 3 days. Daily clinical examination of the patients was performed to detect any early clinical signs of hypocalcemia or vocal cord palsy. The patients were discharged after the removal of the neck drain, normally 3 days after the surgery. They were not followed after their discharge from SML by the thyroid surgical team, which always left Uganda immediately after the surgical camp. However, the follow-up was performed by the local medical doctors and scheduled at 3, 6 and 12 months after the surgery. The histopathological examination of the excised thyroid tissue was performed at the Department of Pathology of SML.
The patients were selected for surgery on the basis of the inclusion and exclusion criteria, which are summarized in Table 1. A lobectomy was performed in cases of a single lobe macronodule or single lobe MNG. A loboisthmusectomy was performed for an MNG involving one lobe plus the isthmus. A STT was performed for an MNG involving both thyroid lobes if the patients could not afford lifelong therapy with thyroxin for cultural or socio-economic reasons; otherwise an indication for TT was given for an MNG. Furthermore, before performing a TT, we determined whether a calcium supply was available during hospitalization and in the immediate postoperative period to prevent dangerous hypocalcemia.
| Inclusion criteria | Exclusion criteria |
|---|---|
| Single lobe macronodule | General problems |
| 1.Heart failure | |
| 2.COPD* | |
| Multinodular goiter | Local problems |
| 1.Retrosternal goiter | 1.Patients with giant MNG could not afford total thyroidectomy |
| 2.Hyperthyroid goiter (fT3 and fT4 in the normal range at presentation) | 2.Hyperthyroid goiter (fT3 and fT4 out of normal range at presentation) |
| 3.Compressive symptoms | 3.Well-controlled euthyroid goiter without compressive symptoms |
| 4.Hoarseness | |
| 5.Painful goiter | |
| 6.Increased in volume with changing ultrasonographic characteristics | |
| 7.Pharmacologically well controlled Graves’ disease |
Table 1: Inclusion and exclusion criteria.
We described the general characteristics of the study population, including the sex, age, clinical diagnosis, thyroid hormone status, type of surgery, and operation time. Then, we compared the number of partial thyroidectomies and STTs to the TTs performed over the years.
We used Stata/SE 9.1 (StataCorp, College Station, TX) to perform the statistical analysis. The differences between the groups were analyzed using Fisher’s exact test, and a P-value equal or less than 0.05 was considered statistically significant. The study protocol was approved by both the Italian ethical committees of Florence and Arezzo and by SML, according to the Helsinki declaration. All of the patients signed a written informed consent before being included in our study.
From an initial pool of 218 patients, 142 (65.14%) were considered to be eligible for surgery. One hundred thirty-seven (96.48%) of the 142 surgical procedures performed were thyroidectomies. The other 5 (3.52%) cases included 3 Sistrunk procedures, 1 biopsy of a tender mass in the anterior cervical region with normal thyroid tissue, resulting in a diagnosis of fibromatosis on the final histopathologic analysis, and 1 biopsy of a suspected anaplastic cancer associated with a tracheotomy. Because the study focused on thyroid surgery, the 5 procedures that were not thyroidectomies were excluded from the analysis. Finally, 76 (34.86%) of the patients did not meet the inclusion criteria for the thyroidectomy: in 10 of 76 cases (13.16%), we recommended TTs for giant goiters that the patients could not afford; therefore, we considered this group not eligible for surgery; 27 (35.5%) were affected by uncontrolled hyperthyroidism at the time of our medical examination; 19 (25%) of the patients had a pharmacologically well-controlled euthyroid goiter or single nodules causing neither compressive nor other symptoms; 2 patients (2.6%) were considered at high risk for surgery due to impaired general health conditions; 15 (19.7%) were not submitted to surgery for logistical reasons; 2 (2.6%) had unresectable anaplastic cancer. Finally, 1 patient (1.3%) died during the anesthesia induction due to heart failure.
The general characteristics of the study population are described in Table 2. In patients with hypertension, an oral anti-hypertensive therapy was administered few days before the surgery.
| Number of patients | |
| Gender | |
| Male | 9 |
| Female | 128 |
| Age | |
| ≤44 years | 85 |
| ≥45 years | 52 |
| Hormone status | |
| Euthyroid goiter | 97 |
| Hyperthyroid goiter | 36 |
| Subclinic hypothyroid goiter | 4 |
| Clinical diagnosis | |
| Single lobe MNG/Single lobe macro-nodule | 94 |
| BilateralMNG | |
| Type of surgery | |
| Lobectomy | 84 |
| Loboisthmusectomy | 13 |
| Sub-total thyroidectomy | 25 |
| Total thyroidectomy | 15 |
| Operation time | |
| Lobectomy | 66.4 min (50-90) |
| Loboisthmusectomy | 88.75 min (55-120) |
| Sub-total thyroidectomy | 115 min (70-120) |
| Total thyroidectomy | 85 min (70-100) |
Table 2: Characteristics of patients submitted to thyroidectomy.
Of the 137 thyroidectomies, 84 lobectomies and 13 loboisthmusectomies were performed in cases of unilateral disease (a single-lobe MNG or single-lobe macronodules causing compressive symptoms).
We performed STTs in 25 cases and TTs in 15 cases. In one case TT was associated with bilateral modified radical neck dissection with preservation of the internal jugular vein and the spinal accessory nerve plus central compartment and upper mediastinal lymphnodes dissection for the presence of multiple neck and mediastinal metastases from papillary thyroid carcinoma.
Hyperthyroidism was present in 47 of the 137 (34.3%) cases; however, only 36 (26.27%) patients with pharmacologically wellcontrolled hyperthyroidism at the time of presentation could be operated, the other 11 (8.03%) were referred to clinical follow-up to continue medical therapy until the normalization of their thyroid hormone status. Graves’ disease was clinically present in 15 (31.91%) of the 47 cases of hyperthyroidisms, and 12 (80%) of these 15 cases were submitted to surgery.
TTs were performed only in the last three camps. The increasing number of TTs yields a statistical significance when compared with partial thyroidectomies (p=0.02) and STTs (p<0.0001) (Figures 2 and 3).
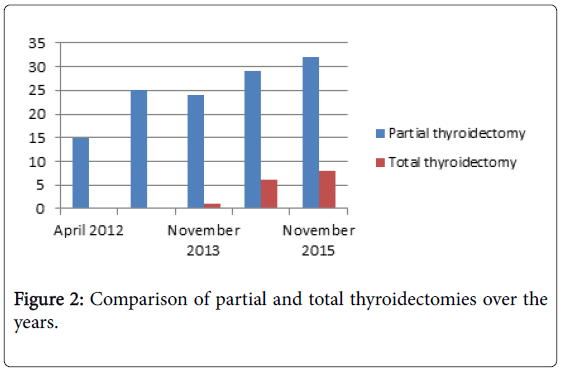
Figure 2: Comparison of partial and total thyroidectomies over the years.
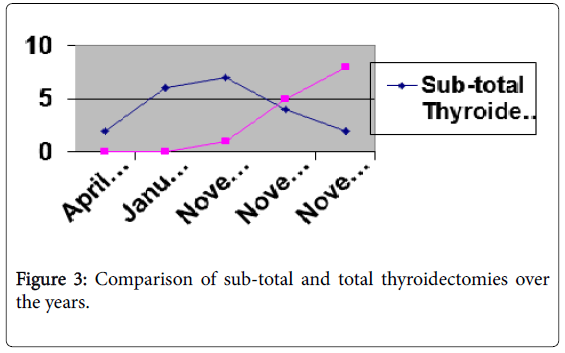
Figure 3: Comparison of sub-total and total thyroidectomies over the years.
The histopathological findings were benign in 133 out of 137 cases, including 90 (65.7%) cases of nodular hyperplasia, 26 (18.98%) colloidcystic nodules, 15 (10.95%) follicular adenomas, 2 (1.46%) lymphocytic infiltration of the nodules; finally 4 (2.92%) were papillary thyroid carcinomas. We recorded 5 postoperative complications: 2 cases of immediate postoperative bleeding that underwent successful surgical revision within the first 2 hours; 1 case of severe dysphonia associated with dysphagia in a TT for a giant goiter, with symptoms fully recovered one month after the surgery; 1 surgical wound dehiscence in a patient who underwent TT for a substernal goiter, treated with dressings and oral antibiotic therapy and recovered 15 days later. Finally, the recurrent laryngeal nerve (RLN) could not be spared during a totalization of thyroidectomy for a recurrent MNG after STT. One 15-year-old patient with well-controlled hyperthyroidism died at the end of a sub-total thyroidectomy for unknown reasons. We suspected a misdiagnosed cardio-vascular congenital malformation. The distant follow-up did not reveal any complications in the patients treated.
Economic development is increasing the life expectancy in LMICs and thus also the incidence and prevalence of chronic noncommunicable diseases that often require surgical treatment (i.e., cardiovascular disease and cancer).
Herein, we focused on thyroid goiter, which exemplifies the chronic troubling issues that affect developing countries [1,2]. Iodine deficiency is the most important risk factor for goiter [9]. Moreover, there is epidemiological and experimental evidence that the concomitant exposure to a cyanogenic glucoside, linamarin from Cassava, which is commonly eaten in poor rural areas, significantly increases the severity of goiter endemia in the presence of iodine deficiency [10,11].
In agreement with the literature [12], the common symptoms at presentation in our series included compressive symptoms of the neck, symptoms related to hyperthyroidism and cosmetic issues. In our study, Graves’ disease was clinically diagnosed in 32% of the entire case series, and cancer represented only a minority of the total number of patients, 7 cases of which 4 submitted to surgery. All of our patients had a diagnosis of thyroid enlargement on an ultrasound scan, and their hormone values were also analyzed. In the cases in which we suspected thyroid cancer, an FNAC of the major nodule was performed. In a developed country, this would be the standard of care for thyroid patients; unfortunately, it is often not universally available inside the African countries and requires an additional and expensive fee that few people can afford. Thanks to the existence of basic diagnostic procedures, such as hormonal blood tests and ultrasonography, we had the opportunity to select surgical patients appropriately.
During 5 surgical camps, we performed 137 thyroid procedures, 122 were partial or sub-total thyroidectomies and 15 were TTs.
In our series, the indications for surgery for unilateral thyroid disease included both the lobectomy and the loboisthmusectomy, which are considered to be the best treatment options in Africa [1,11]. These procedures’ main advantage is that they completely spare the contralateral lobe. This is of paramount importance both for ensuring thyroid function and for leaving the contralateral surgical field intact, thereby reducing surgical risks in the case of a recurrence. For a bilateral MNG, a sub-total resection of the thyroid was advocated whenever the thyroxine supply was likely to be inconsistent and unreliable, being the best treatment option in such cases. However, this type of resection does not definitively prevent hypothyroidism due to the possibility of leaving residual nonfunctioning thyroid parenchyma, as has been well reported in the literature [13-16].
Moreover, an STT results in a high risk of recurrence, especially in hyperthyroidism, that often becomes unresectable due to the fixation to the deep planes, increase the complication rates from the presence of surgical scars in cases of re-operation [17-19]. We recorded only one permanent RLN injury during a totalization of thyroidectomy for a recurrent MNG after STT.
On the one hand, a TT essentially eliminates the risk of recurrence, with an accompanying increased risk of permanent hypoparathyroidism or RLN injury. On the other hand, it should be considered the procedure of choice for an MNG whenever possible, especially considering that reoperations for goiter are significantly more morbid than any initial operation [20]. In developed countries, TT represents the treatment of choice for cancers, Graves’ disease and increasingly for benign disease. In LMICs, the risk of hypothyroidism due to a poor understanding or difficult access to a thyroid hormone supply and the risk of recurrence after partial resections need to be balanced. Recommendations for one option instead of another for an MNG treatment appear to be in conflict and reflect the dilemma of choosing an optimal operative strategy. A patient’s compliance and understanding is often unreliable. Because of this, as our team was onsite for only 2 to 3 weeks annually, we felt that a progressive and aware introduction was necessary before proposing a complete resection of the thyroid gland. We also first needed to ascertain the economic and cultural availability of a lifelong thyroxine supply for these patients. Infact, although one thyroxine tablet may cost only approximately 800 Uganda Schellings (0.28 USD), many people would find it difficult to afford its daily intake. Moreover, we must verify the availability of thyroxine in the local pharmacies. While the Mulago group [21] recently described their standard practice of removing all grossly abnormal thyroid tissue leaving normal looking tissue behind, in our sub-total resection of the thyroid we find it difficult to spare only the healthy thyroid tissue because it is normally completely overwhelmed by the presence of macronodules. The same authors stated that the TT was the gold standard only in cases of preoperatively or intraoperatively suspected cancers. Conversely, in SML, we preferred to perform atypical STTs for the MNGs in our first two camps; then, we succeeded in our attempt to gradually reduce their number in favor of TTs. Indeed, we found a statistically significant increased number of TTs compared with partial thyroidectomies (p=0.02) and STs (p=0<0.0001). Finally, in cases of giant goiters, TT represents, in our opinion, the only option worth consideration. In these cases, it is important to keep in mind the high risks for tracheomalacia and bilateral vocal fold paralysis that might occur.
Regarding thyroid cancer, in the 1980s, follicular cancer became prevalent in the regions with deficient iodine intake (35.8% vs 27.3%). In 2000, after the widespread iodination programs, this trend appeared to change in a few countries where the intake of iodine through water and food increased. We found only 4 papillary and 3 anaplastic cancers. Hence, the malignancy rate in our study was significantly lower than the rates previously reported in the literature.
The follow-up of patients is difficult in Africa because it is sporadic, as patients themselves present to doctors only when affected by severe symptoms. Nevertheless, the local medical staff did not report significant late complications in any of the patients who we treated.
In our series the incidence of intraoperative and postoperative complications, such as bleeding, RLN injuries or intraoperative thyrotoxicosis crises was very low if compared to those reported in the Mulago study. We had only 5 complications, which included 2 cases of immediate postoperative bleeding that underwent surgical revision within the first 2 hours, 1 case of severe dysphonia and dysphagia and 1 case of surgical wound dehiscence. The RLN was resected during a totalization of thyroidectomy, however this caused no long-term sequelae. We did not have any cases of symptomatic hypocalcemia. One patient died during surgery. We assumed a severe congenital malformation in this case; however, neither a preoperative nor a postoperative definitive diagnosis was possible. Finally, one other patient aged 74 years died during the anesthesia induction for unknown reasons. Therefore, it is important to treating younger patients than in developed countries, as we cannot control systemic diseases, which often result misdiagnosed, and we do not have access to proper anesthesia tools.
A good surgical selection and planning, in combination with the availability of a well-trained medical staff, represent the most important factors for success in these major surgical procedures. Proper training programs are required to ensure that the visiting surgeons and anesthesiologists can address the broad spectrum of surgical needs and challenging conditions of the areas they visit.
To the best of our knowledge, this study is the first to report the progressive introduction of TT into a sub-Saharan area. We believe in the importance of missions lasting over time and in the need for sensitizing local individuals by sharing common projects and establishing a positive collaboration.
Herein, we reported a change in the trend of thyroid disease management in SML. Further information is needed to better understand the burden of these disorders, to document their geographic and social backgrounds, and to improve the quality of care in developing sub-Saharan countries.
The authors would like to thank Fondazione Corti and “Centro Salute Globale” for sustaining our project. The humanitarian camps were financially supported by “Centro Salute Globale” of Tuscany Region, Italy.