Journal of Developing Drugs
Open Access
ISSN: 2329-6631
ISSN: 2329-6631
Research Article - (2017) Volume 6, Issue 3
Introduction: Methotrexate is one of the most effective agents in chemotherapy regimens for childhood ALL. However, methotrexate has remarkable side effects, which causes complications in various tissues and organs of some patients under treatment of this drug. It is proved that genetic factors can determine methotrexate toxicity. The aim of this study is to evaluate the effect of RFC-I A80G polymorphism on toxicity and serum level of methotrexate in children affected by acute lymphoblastic leukemia.
Methods: A80G polymorphism of RFC-I was genotyped with PCR-RFLP method in 69 ALL patients treated with methotrexate. The relation between RFC-I genotypes and serum level of methotrexate and toxicity were evaluated using HPLC method and common terminology criteria for adverse events (CTCAE) respectively.
Results: In this study, frequency of allele A for A80G polymorphism was 42.8% in patients who were studied. In consolidation phase, allele A frequency in patients with hepatotoxicity was higher than patients with no hepatic event (P=0.03, OR=2.32, 95% CI=1.10-4.98). Nevertheless, there were not any association between the other types of toxicity and RFC-I genotypes. Also, there was no association between A80G genotypes and the serum level of methotrexate.
Conclusion: Based on the obtained results, we concluded that allele A of A80G polymorphism of RFC-I gene is a risk factor for methotrexate hepatotoxicity in consolidation phase and the A80G polymorphism can be utilized for prediction of methotrexate toxicity and dose adjustment.
Keywords: Methotrexate; Acute lymphoblastic leukemia; RFC-I genotypes and serum; RFC-I A80G polymorphism
Acute Lymphoblastic Leukemia (ALL) is a neoplasm that involves B or T lymphoid progenitors. ALL is the most common leukemia in the children under 15 years old. It has a peak incidence between the ages of 2 and 4 years, and incidence rate are gradually decreasing during later childhood and adolescence. The incidence rises again in the sixth decade of life, which is reaching a second and smaller peak in the elderly [1]. Toxic effects of chemical drugs become a major problem of chemotherapy.
The rate and severity of toxic effects are related to age, sex, race and patient’s pharmacogenetics [2]. Methotrexate (MTX) is an important agent in regimens become candidate for consolidation therapy in children suffering from ALL [3,4]. Methotrexate is an anti-folate agent that inhibits dihydrofolate reductase (DHFR) and thymidylate synthase (TS) enzymes, which are necessary for DNA synthesis and cell division. Therefore, Methotrexate can inhibit the cell division in malignant cells and also in normal cells in some tissues, which are involved with the adverse effects of this drug, such as bone marrow, liver, Nervous system, and gastrointestinal (GI) [5,6].
This agent can uptake by RFC-I transporter protein, whereas it exports from cells by ATP Binding Cassette Transporter (ABC transporters) proteins. Methotrexate in cells is converted to polyglutamate methotrexate by Folyl polyglutamate synthase (FPGS) that could stay in cell for a long time [7,8]. The serum level of methotrexate and its toxic effects differs individually, even in the same dose of MTX. These differences could be due to genetic variations in genes involving in intracellular kinetic of MTX and target genes of MTX, folate cycle and membrane transporters [9,10].
Since the RFC-I is the main folate and anti-folate transporter, many studies have been done on the effect of A80G polymorphism in patients with ALL that take MTX and its relations with toxicity. This polymorphism with rs1051266 ID in dbSNP is placed in coding sequence of RCF-1 mRNA. This polymorphism with amino acid change in location of 27 (His27Arg) of RFC-I protein, leads to change in function of RFC-I protein [10]. Allele A probably leads to decrease the ability of RFC-I protein for importing the MTX into the cell and increase the serum level of MTX [9]. Patients with ALL and lymphoma, that are homozygote for allele A, exhibit toxic complications in Gastrointestinal [9,11].
In this cohort study, incidence of A80G polymorphism of RFC-I gene and its association with toxicity of liver, bone marrow/blood and renal at consolidation and maintenance phase was evaluated. Furthermore, the relationship between polymorphism and various toxicities have been investigated.
Patients
In this study 69 children with ALL referred to Ali Asghar hospital were studied. BFM 2002 protocol was used for treatment of patients [12]. Based on this protocol, all patients received intermediate dose of MTX in consolidation phase and low dose in maintenance phase. Patients with T-ALL and Burkett’s Lymphoma were ruled out because of using different doses of MTX. Clinical and laboratory parameters were collected from patients’ records. All patients' parents filled the consent form.
Assessment of toxicity related to MTX
Forty-eight hours after administration of 2 gr/m2 of MTX, the serum level of MTX were measured by HPLC technique. The toxic effects of MTX on liver, kidney and hematopoietic tissue were evaluated. Assessment of GI toxicity was achieved by patient’s history of Diarrhea, nausea, vomiting and mucositis. Liver function was evaluated by measurement of serum level of aspartate aminotransferase (AST) and alanine aminotransferase (ALT). Kidney function was evaluated by measurement of creatinine.
In order to evaluation the bone marrow function, hemoglobin level (assessment of erythropoiesis), WBC count (assessment of leucopoiesis) and platelet count (assessment of thrombopoesis) was measured by cell counter (sysmex, kx21, Japan). Intensity of toxicity was determined based on Common Terminology Criteria for Adverse Events v3.0 (CTCAE) [13]. According to these criteria, amount of toxicity is based on severity of symptoms.
Polymerase chain reaction and restriction fragment length polymorphism
For each patient 5 ml blood was collected in EDTA tubes, which were kept in -20°C. Then, DNA was extracted by DNA extraction kit (Viogene, USA). Primers were designed for A80G polymorphism on the RFC-I gene and also the PCR condition were summarized in Table 1. For evaluating A80G polymorphism, Hin6I restriction enzyme (Fermentase life science, York, UK) was used. This enzyme detects the 5´… G C G C … 3´ or 3´… C G C G … 5´ sequences and cuts it. This enzyme was added to PCR product and tubes were incubated at 37°C for 16 hours and then product was run on 2% Agarose gel.
| Primer sequence | Number of cycles | Annealing temperature | PCR product | Fragment size after digestion |
|---|---|---|---|---|
| F: 5’-AGGGAGGCCTGCAGACCATCTT-3’ | 40 | 65° | 235bp | A/A genotype: 235bp A/G genotype: 235bp, 182bp and 53bp |
| R: 5’-CCCTGGCCGTATCTACGCCATG-3’ | G/G genotype: 182bp and 53bp |
Table 1: Primers and PCR condition for A80G polymorphism.
Statistical analysis
Data were analyzed using SPSS 17 and OpenEpi 2 [14]. In order to determination of the relation between A80G polymorphism and various types of toxicity, Chi square, and to evaluation the relation between A80G polymorphism and serum level of MTX, one-way ANOVA were used. The odds ratio and P-value were calculated and Pvalues less than 0.05 were considered statistically significant. In this study the effect of A80G genotypes on MTX toxicity was calculated, using Odds Ratio (OR) with CI=95%
Study population
The study population consists of 69 children (37 males and 32 females) ranging from 2 to 13 years old (5.18 ± 3.024 SD). Among the study group, 35 patients were affected by early pre- B, 30 patients were pre-B, and 4 patients were pro B subtype of ALL according to WHO classification [15].
Polymorphism of A80G
A80G Polymorphism was genotyped by PCR method (Figure 1), and then enzymatic digestion was performed using Hin6I (Figure 2). In this study, 22 patients (31.9%) with G/G, 35 patients (50.7%) with A/G and 12 patients (17.4%) with A/A genotype were detected. This SNP was in Hardy-Weinberg Equilibrium (HWE) in ALL patients.
Figure 1: Agarose gel electrophoresis of PCR products. Fragment 235 bp of A80G polymorphism of RFC-I gene. L, Ladder. N, negative control. 1-6, patients sample.
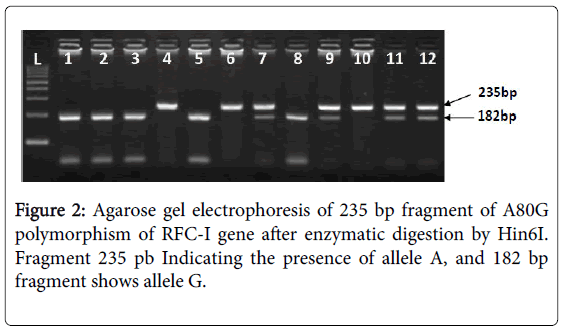
Figure 2: Agarose gel electrophoresis of 235 bp fragment of A80G polymorphism of RFC-I gene after enzymatic digestion by Hin6I. Fragment 235 pb Indicating the presence of allele A, and 182 bp fragment shows allele G.
Assessment of toxicity
Based on CTCAE v3.0 criteria, patients were evaluated for kidney, liver and gastrointestinal tract toxicity. None of patients had toxic kidney in maintenance and consolidation phase.
In maintenance phase, twenty-nine (50%) of patients had no liver toxicity, while 22 patients had liver toxicity grade 1 (37.9%), 5 patients had grade 2 (8.6%), 2 patients were in grade 3 (3.4%) and no one was in grade 4. In consolidation phase, 20 patients had no liver toxicity (31.7%), while 27 patients had toxicity grade 1 (42.9%), 7 patients had grade 2 (11.1%), 9 patients were in grade 3 (14.3%) and no one was in grade 4. Gastrointestinal toxicity only in consolidation phase was recorded.
Among patients, thirty-four cases (66.7%) had no gastrointestinal toxicity, 9 patients had toxicity grade 1 (17.6%), 8 patients had grade 2 (15.7%), and no one was in grades 3 and 4. Evaluation of bone marrow toxicity had been classified in 3 groups including anemia, leucopenia and thrombocytopenia (Table 2).
| Maintenance phase | Consolidation phase | |||||
|---|---|---|---|---|---|---|
|
|
Anemia | Leukopenia | Thrombocytopenia | Anemia | Leukopenia | Thrombocytopenia |
| Grade 0 | 26 | 2 | 39 | 15 | 6 | 33 |
| Grade 1 | 21 | 15 | 13 | 14 | 6 | 8 |
| Grade 2 | 11 | 26 | 4 | 26 | 28 | 6 |
| Grade 3 | 3 | 18 | 4 | 3 | 13 | 8 |
| Grade 4 | 2 | 2 | 3 | 0 | 5 | 3 |
Table 2: Evaluation of the bone marrow toxicity in maintenance and consolidation phase. Based on CTCAE v3.0 criteria, patients were assessed by anemia, Leukopenia and thrombocytopenia and were classified in five grades.
Association between A80G polymorphism of RFC-I gene and toxicity
Association between various types of toxicity (grade 1-4) in maintenance and consolidation phases and various genotypes of A80G polymorphism was analyzed (Table 3). In this study, all patients were divided in two groups: a group with toxicity, regardless of their toxicity grade, and the other group was nontoxic patients.
| Toxicity | A80G polymorphism genotypes | |||||||
|---|---|---|---|---|---|---|---|---|
| A/A+A/G | G/G | OR (95% CI) * | P value** | |||||
| consolidation phase | maintenance phase | consolidation phase | maintenance phase | consolidation phase | maintenance phase | consolidation phase | maintenance phase | |
| Gastro intestinal | 12(32.4%) | 5(35.7%) | 0.86(0.23-3.16) | 0.82 | ||||
| Liver | 23(57.5%) | 31(73.8%) | 6(33.3%) | 12(57.1%) | 2.70(0.85-8.66) | 0.1 | 0.19 | |
| Anemia | 30(75%) | 23(54.8%) | 13(72.2%) | 14(66.7%) | 1.15(0.33-4.05) | 0.60(0.20-1.80) | 0.82 | 0.38 |
| Leukopenia | 36(90%) | 41(97.7%) | 16(88.9%) | 20(95.2%) | 1.12(0.19-6.78) | 2.05(0.12-34.49) | 0.88 | 0.67 |
| Thrombocytopenia | 16(40%) | 17(40.5%) | 9(50%) | 7(33.3%) | 0.67(0.22-2.04) | 1.36(0.45-4.07) | 0.49 | 0.6 |
Table 3: Association between A80G polymorphism genotypes and toxicity of Gastrointestinal, Liver and Bone marrow (Leukopenia, anemia and thrombocytopenia) in consolidation and maintenance phase. In all cases, G/G genotype is considered as reference *, All p values are mutual and product of Mid-P exact**.
Furthermore, association between various types of toxicity (grade 1-4) in maintenance and consolidation phases and alleles of A80G polymorphism was also analyzed (Table 4).
| Toxicity | A80G polymorphism alleles | |||||||
|---|---|---|---|---|---|---|---|---|
| A | G | OR (95% CI) * | P value** | |||||
| Consolidation phase | Maintenance phase | Consolidation phase | maintenance phase | Consolidation phase | Maintenance phase | Consolidation phase | Maintenance phase | |
| Gastro intestinal |
13(27.7%) | 21(38.2%) | 0.62(0.27-1.43) | 0.27 | ||||
| Liver | 32(61.5%) | 39(73.6%) | 6(40.6%) | 47(64.4%) | 2.32(1.10-4.98) | 1.54(0.71-3.35) | 0.03 | 0.28 |
| Anemia | 41(78.8) | 31(58.5%) | 13(70.3%) | 43(58.9%) | 1.57(0.67-3.67) | 0.98(0.48-2.01) | 0.3 | 0.96 |
| Leukopenia | 48(92.3) | 52(98.1%) | 56(87.5%) | 70(95.9%) | 1.71(0.49-6.05) | 2.22(0.22-2.04) | 0.42 | 0.55 |
| Thrombocytopenia | 22(42.3%) | 21(39.6%) | 28(43.8%) | 27(37%) | 0.94(0.45-1.98) | 1.11(0.54-2.31) | 0.88 | 0.76 |
Table 4: Association between A80G polymorphism alleles and toxicity of Gastrointestinal, Liver and bone marrow (Leukopenia, anemia and thrombocytopenia) in consolidation phase of therapy. In all cases, G/G genotype is considered as reference *, All p values are mutual and product of Mid-P exact**.
According to tables, in patients who received medium dose (2 g/m2) of MTX in consolidation phase of treatment, there was no significant association between genotypes and alleles of A80G polymorphism and toxicity of gastrointestinal, bone marrow (leukopenia, anemia and thrombocytopenia). Patients with A/A and A/G genotypes in consolidation phase, experience liver toxicity more than patients with G/G genotype (elevated AST and/or ALT), but it was not statistically significant (p=0.1, OR=2.70, 95% CI=0.85-8.66). However, the frequency of allele A in patients with liver toxicity was significantly more than patients without liver toxicity (p=0.03, OR=2.32, 95% CI=1.10-4.98).
In maintenance phase, which patients received low dose of MTX, there was no significant association between genotypes and alleles of A80G polymorphism and toxicity of liver and bone marrow. Patients with A/G and A/A genotypes in maintenance phase, also experience liver toxicity more than patients with G/G genotype, but it was not statistically significant (p=0.19, OR=2.11, 95% CI=0.70-6.38). Frequency of Allele A in patients with liver toxicity was more than patients without liver toxicity, but it was not statistically significant (p=0.28, OR=1.54, 95% CI=0.71-3.35).
Association between A80G polymorphism RFC-1 gene and serum level of MTX
Association between A80G polymorphism of RFC-1 gene and serum level of MTX was analyzed by one-way ANOVA method (Table 5). However, serum level of MTX in A/A genotype was higher than A/G and G/G genotypes; there was no statistically significant association between A80G genotypes and serum level of MTX.
| Genotype | Number | Mean | SD | 95% CI | P value |
|---|---|---|---|---|---|
| A/A | 12 | 0.41 | 0.45 | 0.00-0.88 | |
| A/G | 35 | 0.39 | 0.17 | 0.29-0.48 | 0.53 |
| G/G | 22 | 0.30 | 0.12 | 0.21-0.38 |
Table 5: Association between A80G polymorphism of RFC-1 gene and serum level of MTX.
Methotrexate is one of the important components of therapeutic agents in pediatric ALL. Typically, all patients in consolidation and maintenance phases receive MTX in high or intermediate and low dose, respectively. Nowadays with new protocols, rate of cure is about 80%. With regard to increasing in the number of cured patients, more attention has been shifted to the adverse effects of the treatment [4].
In recent years, with the discovery of Pharmacokinetics and Pharmacodynamics of many drugs, which are using in ALL, a good understanding of adverse effects and drug toxicity are provided, especially proteins and genes that are involved in metabolism and transportation the drugs. Based on genetic variations in each patient, optimal dose of drug is predictable which leads to decrease the side effects and drug toxicity and probably more successful therapy.
Based on previous study Thiopurinemethyltransferase (TPMT) gene polymorphism has effects on 6-MP metabolism and toxicity, therefore in many guidelines recommended that before starting the treatment with 6-MP, status of TPMT polymorphisms must be determined [16].
One of the main drugs in ALL chemotherapy regimens, particularly in BFM 2002 protocol is methotrexate. This drug has side effects such as Myelosuppression, liver, gastrointestinal and kidney toxicity [4]. Appearance of these adverse effects is different in each patient even in same dose of MTX. Therefore, it seems that it is influenced by various factors such as patients genetic. MTX is an analog for folate and can suppress cycle of folate in cells by inhibiting the DHFR and TS, therefore many studies have done on the genetic variation of enzymes involving in folate cycle.
Some of these studies have shown the association between polymorphism of MTHFR and RFC-1 genes in occurrence toxicity related to MTX [10,17,18]. We studied the most common single nucleotide polymorphism of RCF-1gene, and relation to the toxicity and serum level of MTX in children with ALL. To our knowledge this study was the first study which Iranian patients were evaluated for allele frequency of A80G polymorphism of RFC-I gene.
Rely on this study; the frequency of A/A, A/G and G/Genotypes were 17.4%, 50.7% and 31.9%, and the frequency of A allele and G allele was 42.8% and 57.2% respectively. According to HapMap database (hapmap.ncbi.nlm.nih.gov), the frequency of allele A in American with West European origin population (CEU) is 45%, in Chinese population (CHB) is 50%, Japanese population (JPT) is 56.8% and in African Population (YRI) is 74.2%. Therefore, the frequency of allele A in Iranian population was similar to European and American Populations.
In our study, in consolidation phase there was no association between allele frequency of A80G polymorphism of RFC-I gene and gastrointestinal and bone marrow (leukopenia, anemia and thrombocytopenia) toxicity, but, allele had a significant association with live toxicity. In maintenance phase, there was no significant association between genotypes and alleles of A80G polymorphism of RFC-1 gene and liver and bone marrow (leukopenia, anemia and thrombocytopenia) toxicity. Furthermore, A80G polymorphism of RFC-I gene had no effect on the serum level of MTX.
Yanagimachi et al. studied relation between effect of polymorphisms of genes that are involved in folate cycle such as RFC-I on MTX toxicity in 92 children with Rheumatoid Arthritis treated with 10 mg/m2 MTX (which is similar to MTX dose in consolidation phase). They couldn’t find any association between liver dysfunction and A80G polymorphism of RFC-I gene, which confirm our results [19].
Laverdière et al. studied A80G polymorphism of RFC-I gene, its relationship with serum level of methotrexate and outcome of childhood acute lymphoblastic leukemia. Based on their findings, patients with allele A have higher risk of toxicity in both consolidation and maintenance phases. Based on this study, allele A leads to poor prognosis and higher serum level of MTX [9].
Kishi et al. showed relationship of several polymorphisms such as A80G polymorphism of RFC-I gene on chemotherapy toxicity related to ALL [20]. They used high dose of MTX for patients who was different with our study population and concluded consolidation and maintenance phases. They showed that allele A of A80G polymorphism of RFC-I gene leads to gastrointestinal toxicity. This association was not seen in our study, which could be due to differences in chemotherapy regimen (different MTX dose), race and number of patients.
Furthermore, in Kishi et al. and Shimasaki et al. showed the serum level of MTX in various A80G genotypes had nosignificant difference [10,20]. Shimasaki et al. found that frequency of G allele in patients with vomiting was significantly higher but in case of liver toxicity and mucositis they couldn’t found any significant relationship [10]. Also, Pakakasama et al. assessed the effect of genetic variations of folate metabolism enzymes on high dose MTX toxicity which had no effect on MTX toxicity [18].
Kotnik et al. Reviewed the effect of folate metabolism cycle enzymes polymorphisms on Methotrexate pharmacokinetics and toxicity who were treated with high dose MTX [21]. They concluded that G allele leads to protection against leukopenia that in the present study these findings were not obtained.
Erculj et al. studied on MTX pathway polymorphisms on HD-MTX treatment outcome in children with ALL. They genotyped children for methylenetetrahydrofolate dehydrogenase (MTHFD1) 1958G>A, methylene tetrahydrofolate reductase (MTHFR) 677C>T and 1298A>C and thymidylate synthase (TYMS) 2R>3R polymorphisms.
The MTHFD1 1958A allele significantly reduced the liver toxicity. The TYMS 3R allele significantly reduced the odds of leukopenia and thrombocytopenia [21]. In most of previous studies and also our study allele A of A80G polymorphism had been identified as a risk allele for Liver toxicity. It should be mentioned that degree and type of toxicity associated with A80G polymorphism can be different. Difference scan be influenced by: study design, Chemotherapy regimen, race, age, therapy phase, definition and degrees of the toxicity, etc.
Based on the results it seems that the Allele of A80G polymorphism could be as a risk factor for liver toxicity related to MTX usage in consolidation phase of treatment. It seems that larger sample size in subsequent studies is required to obtain more reliable data. This data can be used to develop an algorithm for adjustment the dose of methotrexate in ALL patients. This algorithm could be used to reduce the side effects of methotrexate.
We are gratefully appreciating financial support by Iranian National Science Federation (INSF) to complete this project.