Journal of Cancer Science and Research
Open Access
ISSN: 2576-1447
ISSN: 2576-1447
Research Article - (2022)Volume 7, Issue 6
Chemotherapy-induced nausea and vomiting (CINV) is one of the most common and feared side effects of chemotherapy especially in breast cancer. Despite recent advances in pharmacologic antiemetic therapy, additional treatment for break- through CINV is needed. Auriculotherapy, is a safe alternative medicine procedure with minimal side effects; several ran- domized controlled clinical trials have suggested its efficacy in controlling this side effect. A recent randomized controlled clinical trial in Iran , demonstrated that Auriculotherapy, significantly reduced the proportion of patients experiencing acute stress and vomiting during IVF. That trial, however, did not show that Auriculotherapy, significantly alleviated acute chemotherapy-induced nausea or delayed CINV. The clinical relevance of these results were limited by the fact that they predated the use of aprepitant and that only few Auriculotherapy points were stimulated during Auriculotherapy, treatment. More clinical trials to study the effect of acupuncture with additional antiemetic acupuncture points in ad- junct to modern pharmacologic antiemetic therapy are needed. Chemotherapy-induced nausea and vomiting (CINV) is one of the most common and feared treatment-related side effects among patients with cancer especially in breast cancer . Over the past decade, better understanding of the physiology of CINV and subsequent development of modern pharma- cologic antiemetic agents have substantially improved the control of CINV. However, a study suggests that CINV remains a significant problem among these patients.2 In addition, pharmacologic antiemetic agents are expensive and associated with potential side effects, and therefore exploring nonpharmacologic options for controlling CINV is important. Auric- ulotherapy, is an Chinese , europian medical technique proven to be effective and safe in treating multiple conditions, including nausea and vomiting caused by pregnancy,3 sea sickness,4 surgery,5 and chemotherapy.
Breast cancer is the most common cause of cancer morbidity in women worldwide [1]. In 2016, it was estimated that approximately 260,370 new cases were diagnosed in the United States [2]. First- line treatment for early breast cancer is curative surgery, but the cancer relapse rate is relatively high when using surgery alone [3, 4]. Researches indicated that the addition of adjuvant chemotherapy to surgery provided clinical benefit for breast cancer patients [5]. A widely used postoperative adjuvant chemotherapy protocol includes combination therapy [6, 7]. While has therapeutic efficacy, use of this therapy also has concomitant adverse effects, including neutropenia, thrombocytopenia, nausea, vomiting, diarrhea, asthenia and neurotoxicity [6]. While application of these drugs can effectively reduce symptoms, these agents also
have side effects such as mood disturbances and drowsiness [8]. Additionally, glucocorticosteroids may reduce anti-tumor effects of some chemotherapeutic agents [9].
Background
Before the advent of 5-hydroxytryptamine-3 (5-HT3)– receptor antagonists and neurokinin-1–receptor antagonists, CINV was poorly controlled. Among patients undergoing chemotherapy, 70% to 80% experienced severe CINV.7 Risk factors for CINV include female gender, young age, and treatment with highly emetogenic chemotherapy.8 Chemotherapy agents are divided into 4 emetogenic risk levels: high (> 90%), moderate (30%– 90%), low (10%–30%), and minimal (< 10%).1,9 CINV can be either acute, delayed, or anticipatory. Acute CINV occurs within 24 hours of chemotherapy, usually beginning within 2 to 4 hours and peaking in the first 4 to 6 hours.8 Delayed CINV occurs from day 2 to 6 of chemotherapy.8 Anticipatory CINV occurs before chemotherapy treatments in patients who have previously experienced significant CINV.8 Most antiemetic research focuses on reducing acute and delayed CINV, with the understanding that this would result in better control of anticipatory CINV.
Animal studies suggest that emetogenic chemotherapy agents entering the body through either mucosa or blood stimulate enteroendocrine cells located in the gastrointestinal mucosa of the proximal small intestine.8 Consequently, the enteroendocrine cells release local mediators, such as 5-HT, substance P, and cholecystokinin.8 These mediators then bind to the corresponding receptors at the end of the vagal afferent fibers located nearby, triggering the afferent stimuli and reaching the loosely organized neuronal areas within the medulla.10 Those neurons then coordinate the emetic reflex and result in nausea and vomiting.8
Other studies suggest that CINV occurs after neurotransmitters, such as dopamine, 5-HT, or hormonal stimuli, bind to area postrema, a structure located in the caudal end of the fourth ventricle,11 or the limbic forebrain.12
Corticosteroid has been used extensively as an antiemetic agent over the past 25 years, although its antiemetic mechanism is not well understood.8 Dopamine, 5-HT, and substance P are believed to be the important neurotransmitters mediating CINV.8 As a result, antiemetic medications are divided into 3 main categories: dopaminergic, 5-HT3–receptor, and neurokinin-1– receptor antagonists. Although dopaminergic antagonists, such as prochlorperazine, haloperidol, and metoclopramide, are the oldest and most widely used antiemetic drugs, they are associated with lower therapeutic index and greater potential side effects.
Understanding the important role 5-HT played in preventing CINV has revolutionized therapy;8 it has been regarded as the most important receptor in acute CINV.13,14 5-HT3 receptors are located in both central (area postrema) and peripheral nervous systems (vagal afferents).15 Selective 5-HT3–receptor antagonists have been established as standard CINV prophylactic therapy for patients undergoing moderately or highly emetogenic chemotherapy. Common side effects associated with 5-HT3– receptor antagonists are mild headache, transient liver enzyme elevation, and constipation.8 Although 5-HT3–receptor antagonists are highly effective in preventing acute CINV, they have notably lower efficacy in preventing delayed CINV.16 Substance P has also been suggested to play an important role in CINV. Its receptors, neurokinin-1 receptors, are located throughout central and peripheral nervous systems, including the area postrema and gastrointestinal tract. Aprepitant is the first drug in the class of neurokinin-1–receptor antagonists. Two phase III, randomized, controlled trials showed that the 3-drug combination of aprepitant, ondansetron, and dexamethasone controlled CINV significantly better than the 2-drug combination of ondansetron and dexamethasone during a 5-day study in patients undergoing highly emetogenic chemotherapy.17,18 These results led the FDA to approve adding aprepitant to antiemetic regimens for patients undergoing highly emetogenic chemotherapy.
Based on available evidence, current antiemetic guidelines recommend a 3-drug combination of a 5-HT3–receptor antagonist, dexamethasone, and aprepitant for patients undergoing highly emetogenic chemotherapy. For moderately emetogenic chemotherapy, a 2-drug combination with a 5-HT3– receptor antagonist and dexamethasone is recommended. For low emetogenic chemotherapy, dexamethasone with or without dopaminergic antagonists is recommended. No antiemetic agent is recommended for chemotherapy agents with minimal emetic risk.8
Using the current regimens, CINV is much less prevalent or severe. However, several questions remain. Although chemotherapy-induced vomiting has been much better controlled by the newly developed pharmacologic agents, chemotherapy- induced nausea is not.2 This problem was illustrated in a phase III, randomized, controlled trial assessing the role of aprepitant in patients receiving anthracycline and cyclophosphamide, in which aprepitant significantly lowered the proportion of patients experiencing chemotherapy-induced vomiting (76%–59%) but did not change the rate at which they experienced nausea.19 Lastly, even with the 3-drug regimen, 11% to 17% still experience acute CINV.17,18 Additional therapy is needed for breakthrough CINV and to better control nausea. Nonpharmacologic therapy, such as acupuncture, has therefore attracted significant research interest because of its minimal side effects and reported efficacies in relieving nausea and vomiting caused by multiple conditions.
Auriculotherapy is a therapeutic technique that can be used independently as well as in a complementary way to any other treatment. This technique is often referred to as ear acupuncture or auricular acupuncture and consists of treating very precise points on the ear for therapeutic purposes. Auriculotherapy can be a real asset where conventional treatment lacks efficiency or can not be used anymore because of serious side effects.
How auriculotherapy works can be outlined as follows: our brain disposes of a map of the entire organism that enables it to manage all bodily functions. This map is also present on the auricles. All information coming from the body is sent up to the brain but passes also through the auricles. This goes also for the information from the brain to the body. Treatment of very specific areas on the auricle permits to control the functioning of all possible organs that have their representation on the ear.
So, auriculotherapy consist in treating a number of points on the auricle in accordance with the pathology involved. Depending of the disease, specific neurovascular complexes are disturbed. These ‘points’ can be detected by palpation or by means of electrical detection. Objectivating active points on the ear has to be done very precisely, within a fraction of a millimeter.

Modern auriculotherapy is founded on very strict scientific principles and can be explained by neuroembryological and neurogenetic mechanisms: in the course of embryological and foetal development an auricular map arises that is practically identical to the cartographical relationship between brains and body. This neurophysiological accordance permets to send therapeutic ‘requests’ to the brain using our ears. If one would compare the human organism with a computer, then our auricles not only function as a screen but also as a keyboard enabling the auriculotherapist to send commands to the brain. When these commands or requests are justified (i.e. when there is really a problem), our brain attemps to correct the problem by means of a palet of neurophysiological mechanisms. In essence, auriculotherapy is nothing more (but also nothing less) than applied neurology.
The goal of a treatment is to modify the structure of the auricular point. This can be achieved in various ways:
by using cold (CAT or Cryo-Auriculo-Therapy), a very recent technique that was delevoped by Dr.David Alimi and his co- workers at the University of Paris XIII.
Auriculotherapy itself is quite painless, semi-permanent needles disappear spontaneously after days or weeks. The result can be very immediate or can be delayed by hours or days. Some patients can react very intensely and show transient aggravation. In general, one notices an improvement during the first week after treatment in case of recent problems and within a month in case of older problems.
When the result is insufficient, another treatment is planned. In most cases, 3 initial treatments are necessary. After that, the treatment plan is adapted in function of pathology, chronicity and evolution. Time between treatments varies between 2 weeks, a month to even several months.
Breast cancer patients were recruited for this study following criteria: aged 18-62 years and received adjuvant therapy. for patients to seek professional help for side effects due to difficulty of travel and time constraints. This may lead to lower compliance for utilization of S-1 oral treatments.
Auricular point acupressure (APA) is a well established treatment strategy in traditional Chinese medicine [10]. APA differs from acupuncture in that it requires neither needle insertion nor frequent visits to the therapist’s office [11]. Instead, APA works by fixing small plant seeds to the inner or outer auricular surfaces with tiny adhesive patches to stimulate acupoints [10, 11]. The APA technique originated from ancient China and was further studied by Nogier in the 20th century [12]. APA has been recognized by the World Health Organization to have whole- body therapeutic effects [13]. Currently, APA is widely applied to relieve various health problems, including anxiety, pain, smoking cessation, substance abuse, insomnia, nausea and vomiting from pregnancy or chemotherapy, weight control, and low back pain [11]. APA was found to mitigate chemotherapy-induced nausea and vomiting in ten pediatric patients studied for seven days [14].
In this study, we explored the efficacy of APA as a technique to control gastrointestinal dysfunction and improve nutritional status in gastric cancer patients on an at-home oral S-1 therapeutic protocol.
This was a prospective, randomized, controll- ed, single-blinded study, which was conducted malignant tumors, auricle defects or infections, previously diagnosed gastrointestinal disorders or having received any acupuncture or acupressure treatments in the past three months.
The recruited participants were randomized into two sub- cohorts (control and experimental) by applying restricted
randomization methods to achieve a balanced size between the groups. The adjuvant regimens were administered for all patients in three-week cycles. Patients in the control sub-cohort received non-digestive-organ directed APA treatments, while participants in the experimental sub-cohort had standard APA treatments. Prior to seed fixation, patients were asked to sit comfortably and silently. Outer ears were cleaned with 75% alcohol swabs. Specific auricular points for nausea, vomiting and diarrhea, as defined by Huang et al., were selected in the experimental subcohort, including the shenmen, cardia, stomach, sympathetic, digestive subcortex, liver and spleen (Figure 1A) [15]. Auricular points selected in the control sub-cohort were not associated with digestive system organs; these points included the eye, wrist, toe and external genitals (Figure 1B). The seeds were administered on the first day of a chemotherapy cycle and maintained for 21 days. If the fixations of the seeds were loosened or the seeds were lost, patients were asked to visit the treatment provider for re- treatment. Additionally, participants were trained to stimulate the acupoints at least three times per day for at least three minutes each time, even if symptoms were not present
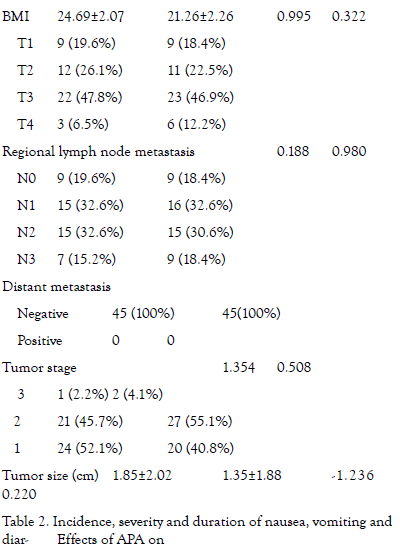
The clinical characteristics of participants were obtained from patient medical records. Nation- al Cancer Institute (NCI) common toxicity cri- teria (version 2.0) guidelines were applied to evaluate the severity of nausea, vomiting and diarrhea (Table 1). Participants were taught to record the severity of the adverse events daily throughout the experimental course. Ad- ditionally, patients were called every seven days to remind them to answer the questionnaire. The weight, height, total blood protein and albumin levels of each participant were measured two times, at the beginning and end of the study. Body mass index (BMI) was calculated using the following equation: BMI = weight (kg)/height (m)2.
Sample size of calculation ample size calculation
The primary study outcome was the difference in vomiting incidence rate between the sub-cohorts. The study was designed to have a statistic- al power of 0.9 to detect a difference between the subcohorts, on the basis of a published vomiting incidence rate of 10% in an experimental sub-cohort and of 40% in controls, with a two-sided alpha value of 0.05 [14, 16]. Achi- eving these specifications re- quired the recruitment of 40 participants per sub-cohort; 45 patients were recruited per sub-cohort to account for loss-to-follow up.
Patient demographics and clinical data
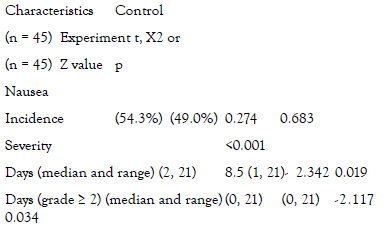
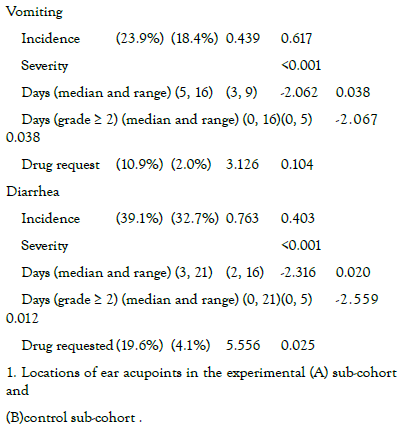
APA treatment is a feasible technique to decrease the severity and duration of nausea, vomiting and diarrhea events experienced by breast cancer patients receiving chemotherapy. Use of this technique may have improved the nutritional status of recipients. These data did not indicate that gastrointestinal-targeted APA reduced overall incidence rates of nausea, vomiting and diarrhea. More studies are needed to verify the findings of the present research and to further explore the underlying mechanisms of APA.
Co workers from the seyedelshohada Hospital helped with the trial completion.
Citation: Tofighi SAR, Reyhani M, et al. (2022) The effect of Auriculotherapy in the Control of Chemotherapy-Induced Nausea and Vomiting in Women with Breast Cancer. J Can Sci Res 7:524
Received: 10-Oct-2022, Manuscript No. JCSR-22-5634; Editor assigned: 12-Oct-2022, Pre QC No. JCSR-22-5634 (PQ); Reviewed: 26-Oct-2022, QC No. JCSR-22-5634; Revised: 03-Nov-2022, Manuscript No. JCSR-22-5634 (R); Published: 11-Nov-2022 , DOI: 10.35248/2576-1447.22.7.524
Copyright: © 2022 Tofighi SAR, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.