Medical & Surgical Urology
Open Access
ISSN: 2168-9857
ISSN: 2168-9857
Research Article - (2018) Volume 7, Issue 4
Introduction: Type-III chronic prostatitis (CP) is characterized by pelvic pain, sexual dysfunction and urinary symptoms in the absence of infection. It is also known as chronic pelvic pain syndrome (CPPS) This study discusses the cause of CP/CPPS, the understanding of which can help to find effective therapy.
Materials: An observational clinical trial, before and 6 months after treatment with Thermobalancing therapy (TT) and Dr Allen’s therapeutic device (DATD), which uses natural body energy, has been used. The treatment group-45 patients with CP/CPPS, who received DATD, and the control group-45 men with CP/CPPS, who not.
Methods: The National Institute of Health Chronic Prostatitis Symptom Index (NIH-CPSI) include examination of pain score and quality of life (QoL), ultrasound-prostate volume (PVmL), uroflowmetry-maximum urine flow rate (Qmax).
Results: Compared to control, significant improvements from baseline to endpoint were seen: pain score, 10.38 to 3.58 against 10.49 to 9.71, (P<0.001); QoL index 8.11 to 2.98; against 8.47 to 8.33 (P<0.001); PVmL 31.75 ± 7.01 to 27.07 ± 4.52 against 30.77 ± 6.44 to 31.58 ± 7.14 (P<0.001); QmaxmL/sec, 11.93 ± 4.34 to 16.45 ± 3.50 against 12.59 ± 3.57 to 12.20 ± 2.54 (P<0.001).
Conclusions: Vascular changes, namely pathological activity of capillaries, in the prostate tissue cause CP/ CPPS. The focus of hypothermia combined with spontaneous expansion of capillaries create the pressure in the prostate tissue and, consequently, the CP/CPPS symptoms. DATD, by accumulation of emitted body heat and spreading this safe energy to the prostate in men with CP/CPPS, relieves pain and other symptoms effectively.
Keywords: Aetiology of CP/CPPS; Thermobalancing therapy; Chronic prostatitis; Pathophysiology of CP/CPPS; Cause of chronic prostatitis symptoms
Many scientists propose that chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS) may not exist as a disease, as its pathophysiological mechanisms are unknown and there are no suitable and effective treatments [1,2]. Other scholars see the immunological mechanisms underlying chronic pelvic pain and prostate inflammation in CP/CPPS [3,4]. Some of researchers are still looking for infection in CP/CPPS and, consequently, recommend antibiotics, alpha-blockers and antiphlogistics to treat this common disease [5,6].
CP/CPPS is disease troubling men below their 50th with severe pelvic pain, sexual dysfunction and urinary symptoms, having negative impact on quality-of-life, with prevalence in average 8.2% of men’s population [7,8]. Mental health remains a major challenge in men with CP/CPPS and is a source of frustration to both the patient and urologists or general practitioners, since standard treatments often fail [9]. Therefore, new treatment procedures for CP/CPPS are required [10].
The cause of all chronic non-malignant internal diseases, including CP/CPPS, originates at the vascular level and termed as pathological activity of capillaries [11]. 2 physiological properties of capillaries are activated by an initial trigger, which can be infection cold, stress, etc. They named by physiologists’ constriction of capillaries [12], the first property, which emerges a focus of micro-hypothermia in the prostate tissue, and the second property spontaneous expansion of capillaries to improve blood circulation in the affected area [13]. Expansion of capillaries forms extra tissue gradually, and the focus of microhypothermia in the prostate tissue becomes a continuous trigger itself leading to chronic disease.
To liquidate this focus of hypothermia and, consequently, spontaneous expansion of capillaries Thermobalancing therapy (TT) with therapeutic device (DATD) were created and received a US patent. The therapy with DADT, which accumulates the emitted body heat, provides continuous application of a natural source of energy to affected prostate tissue, terminating the focus of hypothermia and chronic process [14]. It was shown that the use of TT with DATD for the treatment of men with benign prostatic hyperplasia (BPH) reduced the size of enlarged prostate and dramatically improved urinary symptoms [15,16].
In men with CP/CPPS inflammation is not associated with an increased risk of this problem but chronic inflammation predicts the risk of symptomatic progression [17]. So, the prostate in men with CP/ CPPS is inflamed and this inflammation can be caused by the violation of the microcirculation in the prostate tissue due to pathological activity of capillaries. In this study, are presented changes in clinical parameters and characteristics in men with CP/CPPS on TT with DATD. Thorough examination of these factors can help to understand the aetiology and pathogenesis of this chronic disease, i.e. the cause of CP/CPPS.
Patient enrollment began in July 2013. The ethics committee of the State Medical University approved the clinical study, and the study complied with the tenets of the Declaration of Helsinki.
The treatment group-45 men diagnosed with CP/CPPS, and the control group-45 men with CP/CPPS. The two study groups were statistically similar. The data gathered in men with CP/CPPS who received treatment with TT and DATD for 6 months was compared with the control group, men who did not receive DATD.
The age of participants was <55 years. The clinical trial was conducted at The Department of Urology of the Yerevan State Medical University. Men were included with confirmed diagnosis of chronic prostatitis; with serum prostatic specific antigen (PSA) >4 ng/ mL, and no histological evidence of cancer. Men with acute prostatitis; urethral stricture, neurogenic bladder, and other co-morbidities such as impaired renal function and diabetes mellitus were excluded from the trial. Medical treatments at the time of enrollment were not taken into consideration. The patient selection was carried out in a multidisciplinary manner in conjunction with urologists. The written informed consent for participation in the study was obtained from all patients.
An observational clinically controlled study was used. The trial was not placebo for ethical reasons, since men with CP/CPPS experience serious mental problems [18]. Providing patients with CP/CPPS for wearing a device that does not help does not make sense, since they will not use it. Of course, after people felt better, they used the device around their body for 6 months, as prescribed. Therefore, we conducted the observational study in which treatment group underwent TT, and the control group did not.
The dynamic of symptoms in men with CP/CPPS who received TT with DATD, without medications and supplements, was compared with the control group, who did not receive DATD. The baseline evaluations included medical history; physical examination, digital rectal examination; serum biochemical measurements, PSA test, electrolytes, urinalysis; and renal function tests. Assessments were made twice, at baseline and after the 6-month period of treatment. All patients were evaluated for NIH-CPSI, pain and QoL scores, ultrasound PV mL, and uroflowmetry Qmax mL/s. Changes of clinical symptoms in each group by using NIH-CPSI. Uroflowmetry was used for the measurement of the rate of urine flow parameters (Sanuro2UL, Santron Meditronic, Maharashtra, India), and ultrasound was used to determine the volume of the prostate gland (US-9000E2 ultrasound scanner, Rising Medical Equipment Co. Ltd, China). The standard ellipsoid formula, length × width × height × 0.52, was used to determine PV.
Outcome measures
Primary end-points were the changes in pain and QoL score after the 6-month treatment period and secondary end-points were the changes in PV and Qmax after the 6-month treatment.
After screening, men in the treatment group were given DATD. Which should be applied topically. It contains a thermoelement, which is made of a special mixture of waxes. This thermoelement accumulates the naturally emitted body heat and turns into a source of energy itself. A second part of the device is an elastic belt that keeps a thermoelement in the projection of the prostate for a prolonged duration.
The thermoelement allows accumulation of body heat and acts as the heat source for the prostate. The neoprene belt keeps the thermoelement tightly applied to the skin, so the energy overcomes skin barrier and spreads toward the affected prostate. Neoprene material prevents heat transfer by closing the thermoelement from the outside (Figure 1).
Figure 1: Device on body.
DATD was registered in 2010 at the Medicines and Healthcare Products Regulatory Agency as a class-1 medical device, as per the independent, authorized CE Marking representative in UK or EU. The regulation of medical devices in Europe and outside the European Union are same, class-I medical device without a measuring function and supplied in non-sterile conditions may only require a supplier’s declaration of conformity, where the manufacturer is responsible for ensuring that the product complies with the relevant requirement.
Statistical analysis
As independent samples t-test and paired samples t-test are only suitable for interval and ratio data, we used the Wilcoxon signed-ranks test for analyses. P<0.05 was considered statistically significant. Statistical analyses were carried out using SPSS v22 (IBM, Armonk, NY, USA).
Dynamic of pain and quality of life in men with CP/CPPS
In this Figure 2, pain score in men with CP/CPPS in the treatment group decreased from 10.38 to 3.58, P<0.001, after DATD was used. In the control group, pain score decreased slightly, from 10.49 to 9.71.
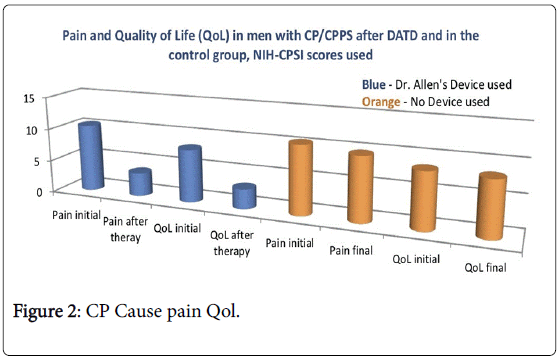
Figure 2: CP Cause pain Qol.
QoL decreased from 8.11 to 2.98, P<0.001, in the treatment group, while in the control group, QoL decreased slightly from 8.47 to 8.33.
Thus, the obtained data demonstrates that men in treatment group after use of DATD have better outcomes in the clinical symptoms than in the control group.
Dynamic of prostate volume and uroflowmetry Qmax in men with CP/CPPS
In this Figure 3, PV mL in men with CP/CPPS in the treatment group decreased from 31.75 to 27.07 mL, P<0.001, after DATD was used. In the control group, PV mL increased slightly, from 30.77 to 31.58 mL.
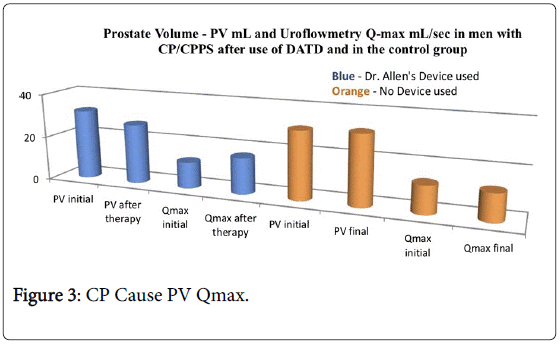
Figure 3: CP Cause PV Qmax.
Qmax increased from 11.93 to 16.45 mL/s, P<0.001, in the treatment group, while in the control group, Qmax decreased from 12.59 to 12.20 mL/s.
Thus, the obtained data demonstrates that men in treatment group after use of DATD have better outcomes in the clinical parameters than in the control group.
The outcomes of the clinical trial demonstrate that TT decreases pain significantly, and consequently improves QoL in men with CP/ CPPS. The reduction of PV and increases of Qmax prove that there is improvement in the prostate tissue. The decrease in the size of the prostate is associated with the cessation of inflammation caused by the pathological activity of the capillaries. This leads to an improvement in blood circulation in the prostate tissue and to a reduction in pain.
These data confirm that TT with DATD are effective for men with CP/CPPS, and DATD can be used for men with CP/CPPS, as an independent treatment option [19,20]. It should be noted that no adverse events were found during the clinical trial in the treatment group.
The study was not randomized. Someone may expect that having a “placebo” or “sham” group for controls could provide more robust outcomes. However, in patients with CP/CPPS, their chronic pelvic pain is largely unresponsive to standard medical interventions, and higher pain is naturally associated with diminished QoL [21]. Furthermore, different placebo-controlled studies in men with CP/ CPPS have not found any improvement in patient using placebotablets, and often patients in the placebo group refused to complete the study because of worsening symptoms [22]. Therefore, it is practically impossible to convince patients with CP/CPPS to wear a shame device on their bodies for six months. Usually, patients experienced some pain relief within a couple of weeks; therefore, they used DATD as was required. Thus, an observational clinically controlled design was used in this study.
Researches proposed immunological, neurological, endocrine, or psychological mechanism of CP/CPPS development [23]. They looked into hypogonadism, a treatment of which is rises in the aging population [24] and recommended the use of testosterone replacement therapy for CP/CPPS, as target therapy [25,26]. In the last decade, vascular dysfunction was suggested in aetiology of CP/CPPS [27], as chronic ischemic processes were found in the prostate tissue [28]. In CP/CPPS patients, color doppler examination of prostate has shown that there is a significant increase in blood circulation in the prostatic capsule and diffusion flow throughout the parenchyma [29]. It was also established increased prostatic pressure in men with CP/CPPS [30].
Standard treatments fail to determine this disorder, so there is no understanding of the cause of CP/CPPS. Therefore, for CP/CPPS a multimodal approach is usually required that may include the six domains: urinary symptoms, psychological dysfunction, organ-specific symptoms, infectious causes, neurologic dysfunction, and tenderness of the pelvic floor muscles [31]. Another review suggests that acupuncture and extracorporeal shockwave therapy may decrease prostatitis symptoms and may not be associated with a greater incidence of adverse event [32]. It also was shown that some of the interventions can decrease prostatitis symptoms in an appreciable number without a greater incidence of adverse events, but the quality of evidence was mostly low [33].
Positive changes in clinical symptoms and parameters in patients with CP/CPPS who used DATD should be explained by changes at the vascular level in the prostate tissue [34]. The findings of this clinical trial correlate with outcomes of another clinical controlled trial on Thermobalancing therapy in men with BPH, where was demonstrated significant decrease of prostate volume and lower urinary tract symptoms in men with BPH after use of DATD. And these improvements in clinical parameters were also associated with positive changes in the vascular level of the prostate gland [35,36].
It was proved that patients with CP/CPPS have significantly higher pressure in the prostatic tissues than the control group subjects [37]. Indeed, pain syndrome can be associated with the increased pressure in the gland. When DATD is applied to the body, the natural thermoelement spreads energy continuously toward the affected prostate, terminating the focus of hypothermia and ischemia, thereby relieving continuous pressure inside the prostate tissue, relieving pain and other CP/CPPS symptoms [38]. Moreover, it should be noted that DATD is a cost-effective solution for men with CP/CPPS, as the thermoelement is active for about a year. Even though CP/CPPS has unpleasant symptoms, they all refer to non-life-threatening conditions that should be treated safely and non-invasively, in the first place. Therefore, this therapy for patients with CP/CPPS should be recommended for patients with CP/CPPS and administered by physicians or general practitioners [39].
The use of TT with DATD in men with CP/CPPS reduces pain and improves QoL. These positive changes in clinical characteristics in parameters after therapy are associated with improvement of blood circulation in the affected prostate. Violation of the microcirculation in the prostate tissue with a constant trigger creates a focus of hypothermia, accompanied by spontaneous expansion of capillaries and increased pressure in the prostate tissue. This chain of physical changes in the prostate tissue can be considered as the cause of CP/ CPPS. Termination the focus of hypothermia by a steady flow of harmless energy from DATD relieves pain and other symptoms of CP/ CPPS. Thus, TT with DATD for men with CP/CPPS should be prescribed as a first-line treatment option.
Ethics committee of the Yerevan State Medical University approved the clinical study with TT and DATD, No. 1, dated 18/09/2014.
Data sharing not applicable to this article as no datasets were generated or analysed during the current study.
These studies were not supported by Grant and did not have financial interest.
There was no additional funding for this clinical study.
I am grateful to Prof Aghajanyan IG, the founder of Armenian Urology Association, and the staff of the Department of Urology at the Yerevan State Medical University for supervision of patients during the study.