Biochemistry & Pharmacology: Open Access
Open Access
ISSN: 2167-0501
ISSN: 2167-0501
Research Article - (2014) Volume 3, Issue 4
Concentrations of Sodium (Na), Potassium (K), Calcium (Ca) and Copper (Cu) in the semen of infertile male with and without varicocele in relation to serum steroid hormones, spermato¬zoa quality were evaluated. The study group comprised of 300 males, 102(34%) with varicocele, 123(41%) without varicocele, and 75(25%) fertile control groups which were randomly selected. Seminal analysis was performed (including volume, sperm count, motility, viscosity, viability and morphology) with biochemical measurements of fructose and mixed agglutination reaction (MAR) for ASA. Atomic absorption was used to estimate the level of Cu, and flame photometer for Na, K and Ca in seminal plasma. Serum levels of progesterone and testosterone were estimated using a competitive chemoluminescent enzyme immunoassay. A significant difference in sperm viscosity, sluggish and immotile sperms, progesterone was appeared among infertile males with and without varicocele in comparison to fertile groups. Despite the significant decreases of semen K and Ca among infertile male (with and without varicocele) in comparison with fertile (p<0.05), the mean Na and Cu concentrations were none significantly between groups. Potassium concentration was highly significant with abnormal testosterone level (p=0.001) and Cu concentration was highly significant with abnormal progesterone level (p=0.001). Furthermore, calcium level was significantly increased (p=0.001) with sluggish and immotile sperms, sperm account, fructose and ASA among normal and abnormal cases. Cu level appeared to be decreased in fertile male compared to infertile male with and without varicocele. Yet, the proportion of abnormality in fructose and % ASA is increased with increasing Cu levels in seminal plasma, whereas low level of Cu showed a negative effect on seminal fluid volume, morphology and sperm count. It is suggested that seminal plasma K and Cu exert particular effects on steroid hormone and semen quality. However, measurement of seminal plasma trace elements may serve as an accurate parameter to evaluate male fertility since they are correlated with the disturbance of semen parameters especially sperm motility, volume, count and viability.
<Keywords: Sodium, Potassium, Calcium, Copper, Steroid hormone
World health organization defined infertility as failure of conceiving a child for at least 12 month of unprotected intercourse [1]. Infertility has been shown to have a high prevalence worldwide (affects one in six). It has been reported that male factor infertility plays a role in approximately 30-55% of infertile couples [2]. However, despite advances in diagnostic methods in the field of andrology, there remains a significant subset of these sub fertile men who are classified as having unexplained male infertility. Male infertility has multiple causes and the commonest single defined cause is sperm dysfunction [2]. Despite the problem in assessing the prevalence of infertility in developing countries, between 8-12% of couples around the world have difficulty conceiving a child at some point in their lives.
The etiologies of male infertility include gene mutations, aneuploidies, infectious diseases, ejaculatory duct occlusion, varcocele, radiation, chemotherapy and erectile dysfunction [3].
Infertility is complex and has many causes and consequences depending on the gender, sexual abnormalities, and environmental factors [4]. Human semen contains high concentrations of trace elements like calcium (Ca), magnesium (Mg), copper (Cu), selenium (Se), and zinc (Zn) in bound and free (ionic) forms. These trace elements play very vital role in affecting various parameters of semen [5].
There are some studies which demonstrate the significance of trace elements in male fertility. Zinc was found to have high levels in semen from mammals, and zinc has been found to be critical to spermatogenesis [6].
Increased levels of metal ions in blood plasma [7] or semen [8] appear to be significantly and positively correlated with male infertility [9]. Spermatogenesis in mammals requires the action of a number of peptide and steroid hormones (sex hormones), each of which plays an important role in normal functioning of the seminiferous epithelium. Sex hormones are not critical only for regulation of male germ cell development, but also for proliferation and function of the somatic cell types required for proper development of the testis [9]. Among the most common somatic cells that are affected by sex hormones are the interstitial steroidogenic leydig cells, whose primary function appears to be production of testosterone [10]. The sertoli cells, whose direct contact with proliferating and differentiating germ cells within the seminiferous tubules makes them essential for providing both physical and nutritional support for spermatogenesis [11]. FSH and LH are secreted by the anterior pituitary and act directly on the testes to stimulate somatic cell function in support of spermatogenesis [12]. LH is known to act on leydig cells to produce testosterone while FSH acts on sertoli cells to promote spermatogenesis [13].
Seminal plasma is very important for sperm metabolism, function, survival, and transport in the female genital tract. Cations such as Na, K, Ca, and P in the seminal plasma establish osmotic balance, while essential trace elements are components of many important enzymes. Thus, biochemical evaluation of seminal plasma is an important criterion for assessing fertility and diagnosing male reproductive disorders [14-16].
Abnormal levels of Ca, Na, K, Zn, and Cu in seminal plasma have been reported to be correlated with infertility in humans. Ca is the trigger for the acrosome reaction in mammalian spermatozoa and there is substantial evidence that Ca is differentially involved in sperm motility, depending on the stage of sperm maturation. However, Magnus et al. [17] reported no association between ionized calcium concentrations and the proportion of spermatozoa displaying progressive movement. Prien et al. [18] compared sperm motility, velocity and progressive movement with total and ionized calcium. The ions present in the semen help in stimulating the motility and glycolysis. The addition of potassium to semen extenders has been shown to improve motility of stallion Padilla et al. [19] and human sperm Karow et al. [20] but Rossato et al. [21] found no correlation between the ionic composition and the osmolarity of human seminal plasma.
Intracellular concentrations of potassium are higher than those of seminal plasma, and therefore potassium levels are linked to sperm concentration. In ram, increasing potassium levels are negatively correlated to progressive motility, while the reverse is true for sodium and chloride Abdel-Rahman et al. [22]. In ram ejaculates, intracellular calcium and magnesium concentrations were higher than in seminal plasma as opposed to phosphate levels. Furthermore, lower values of progressive motility has been reported to be correlated to increasing levels of calcium and decreasing magnesium and phosphate concentrations levels Abdel-Rahman et al. [22].
Copper is an important element for numerous metalloenzymes and metalloproteins that are involved in energy or antioxidant metabolism. However, in its ionic form (Cu+2) and at high level, this trace element rapidly becomes toxic to a variety of cells, including human spermatozoa [23]. It has been identified that Cu is highly toxic for sperm [24]. In vitro studies, it has been demonstrated the effect of Cu in intrauterine devices preventing conception [25]. The present study was designed to evaluate seminal plasma levels of copper, sodium, potassium and calcium and to correlate their concentrations with various semen parameters among fertile and infertile male subjects.
Study groups
Two hundred and twenty- five infertile males including 102 (34%) patient with varicocele and 123 (41%) without varicocele which were recruited in this study. Their mean ages were 31.3 ± 5.2 and 32.3 ± 5.9 years, respectively. Men were attending the infertility department at Medical Hussein City Hospital in Jordan with complete medical and clinical histories. Patients married and infertile (with their fertile female partner) which were for at least more than one year of unproductive intercourse. A questionnaire survey collected data regarding patient occupation, marital status, infertility history and other data. Patients with a history of trace metals exposure or who resided in areas known to have heavy metals contamination, smokers, and alcoholic consumers were excluded from this study. Varicocele was diagnosed after physical examination, duplex, and Color Doppler Ultrasonography. All cases of varicocele were classified as grade I (palpable distension detected only during a valsalva manoeuvre) [25]. Control group was randomly selected from other outpatient clinics of the same hospital and consists of 75 (25%) fertile married males with mean age of 33.36 ± 6.27 years. They are clinically asymptomatic males without varicocele and normal seminal fluids. Informed consent was obtained from all study cases.
Seminal Fluid Samples
Semen specimens were collected through masturbation after 3 days abstinence. Each patient provided at least two samples within one month. Samples were incubated for 30 min at 37°C for liquefaction. A routine semen analysis was performed upon liquefaction according to WHO to measure volume, pH, sperm concentration, motility, viscosity, viability and morphology (WHO, 2010). The remaining semen sample was centrifuged at 1000 ×g for 10 min; the seminal plasma was separated for three equal parts and stored at -70°C until further analyses. Morphology was determined after incubation of the sample with trypsin for 10 minutes at 25°C according to the methylene blue eosin staining procedure, feathering, and fixation by flame. At least 100 cells were examined at a final magnification of 1000x. Viscosity of the liquefied sample was estimated by introducing a glass rod into the sample and observing the thread that forms on withdrawal of the rod. Threads obtained from normal samples should not exceed 2 cm in length [26]. Motility was expressed as a percentage of motile spermatozoa and their mean velocity. The conventional analysis is recommended in which a fixed volume of semen is delivered onto a clean glass slide and covered with a mm cover slip (WHO, 2010). The preparation is then examined at a magnification of 400xs. The microscopic field is scanned systematically, and the motility of each spermatozoon encountered is graded a, b, c, or d. At least 100 spermatozoa are classified in this way. The presence of 50% or more with forward progression (categories a and b) or 25% or more with rapid progression (category a) within 60 minutes of ejaculation were considered as normal results. The results were averaged for the two samples, and a single value was used for each parameter. Sperm motility was calculated by multiplying sperm concentration x106/ml) and semen volume (ml).
Trace elements determination
Determination of Cupper (Cu) concentration was carried out according to a method of using Atomic absorption spectrophotometer (AA 6650 Shimadzu, Japan). While, the determination of Sodium (Na), Potassium (K) and Calicium (Ca) concentrations were analyzed by using Flame photometer (Microprocessor Scientific International, India).
Frozen semen samples were liquefied at room temperature and digested in covered beakers in a fume cupboard with a 1:1 solution of highly purified HN03 under moderate heating conditions (85°C). Al1 laboratory ware used was previously treated with 10% nitric acid for 48 hours and copiously rinsed with distilled-deionized water to eliminate possible traces of metals. Semen samples were diluted 1:50 for Cu, Na, K, and Ca determination. Concentrations were determined by comparison with standard curves covering different concentration ranges. Aqueous standards for plotting calibration graphs were obtained by serial dilution of stock solutions containing 1000 pg/mL of the analyte as nitrates. Blanks were prepared in a similar fashion as samples.
Mixed Anti-globulin Reaction (MAR) Test
The MAR test is performed by mixing fresh, untreated semen with sheep blood cells (SRBs) coated with human IgG. A monospecific antihuman-IgG antiserum is added to this mixture, which was mixed and read within 10 minutes. Positive and negative control samples were run along with each experiment. The formation of mixed agglutinates between sRBC and motile spermatozoa proves the presence of IgG antibodies on the sperms. Immunologic infertility is suspected when 10%-90% of the motile spermatozoa attached to the RBCs [27].
Determination of seminal fluid fructose
The method is adopted from that of Seliwanoff. The principle depends upon the presence of fructose (ketoses), which forms a pink color when heated, with resorcinol in the presence of hydrochloric acid (ARCOMEX, Fructose. S.F). Intensity of the red complex is proportional to the fructose concentration and measured photometrically at 490 nm [28]. Normal fructose level in the seminal plasma is 120-500 g/dl.
Hormone estimation
Serum levels of progesterone and testosterone were estimated by a competitive chemoluminescent enzyme immunoassay using IMMULITE 2000 Progesterone and IMMULITE 2000. Total Testosterone which was utilized specific antibody-coated polystyrene beads as a solid phase [29,30]. Samples were incubated with alkaline phosphatase-labeled regent and the bound label was then quantified using a specific chemoluminescent substrate. Light emission was detected by photomultiplier tube, and the results were calculated for each sample. The normal ranges for progesterone is 0.27-0.9 ng/ml and for testosterone 262-1593 ng/dl.
Statistical analysis
The collected data was entered to statistical Package for Social Sciences (SPSS) version 19. The descriptive statistics using frequency and percentage was used to describe the study variables. The continuous variables within the database were converted to rank cases using four ranks. The ranking was used as a procedure to make possible to test two discrete variable using non-parametric statistics. Kruskal-Wallis test was used to test the effect of independent variables.
Serum and seminal plasma obtained from 300 men including infertile with varicocele, infertile without varicocele, and fertile control males. Their ages varied from 25 to 47 years, thus covering the entire span of the reproductive years. Seminal fluid and serum samples were investigated for the possible relations between trace metals (Cu, Na, K and Ca), seminal fluid parameters, fructose levels, autoimmunity to sperm antigen and steroid hormones.
Seminal fluid parameters
The criteria for normozoospermia was a concentration of ≥ 20×10(6)/ml, with grade a motility in 25% or grade a and b motility in 50% of spermatozoa, normal morphology in at least 30% of the spermatozoa, viability >75% of the total sperms, and semen volume >2 ml. The mean values for normal sperm count(x106), viability(%), progressive motility (x106), and normal morphology(%) were 96 ± 78.0, 84 ± 82.4, and 60 ± 80.0; 6 ± 4.9, 6 ± 5.9, and 9 ± 12.0; 6 ± 4.9, 15 ± 14.7, and 9 ± 12.0; 3±2.4, 0±0, and 3 ± 4 for infertile without varicocele, infertile with varicocele, and fertile males, respectively (Table 1).
| Seminal fluid parameters | Infertile without varicocele Mean ±SD |
Infertile with varicocele Mean ±SD |
Fertile male Mean ±SD |
Count (% of total ) |
P- value | |
|---|---|---|---|---|---|---|
| Sperm count (x106) | Normal Abnormal |
96(78.0%) 27(22.0%) |
84(82.4%) 18(17.6%) |
60(80.0%) 15(20.0%) |
240(80%) 60(20%) |
NS |
| Viability (%) | Normal Abnormal |
6(4.9%) 117(95.1%) |
6(5.9%) 96(94.1%) |
9(12.0%) 66(88.0%) |
21(7%) 279(93%) |
NS |
| Viscosity (cm) | Normal Abnormal |
102(82.9%) 21(17.0%) |
81(79.4%) 21(20.6%) |
60(80.0%) 15(20.0%) |
243(81%) 57(19.0%) |
0.05 |
| Sperm morphology (%) | Normal Abnormal |
3(2.4%) 120(97.6%) |
0(0%) 102(100%) |
3(4%) 72(96%) |
6(2%) 294(98%) |
NS |
| Progressive Motility (a+b) (%) | Existed Not existed |
6(4.9%) 117(95.1%) |
15(14.7%) 87(85.3%) |
9(12%) 66(88%) |
30(10%) 270(90%) |
NS |
| Sluggish motility (c) (%) | Existed Not existed |
99(80.5%) 24(19.5%) |
90(88.2%) 12(11.8%) |
75(100%) 0(0%) |
264(88%) 36(12.0%) |
0.001 |
| Immotile (d) (%) | Existed Not existed |
105(85.4%) 18(14.6%) |
96(94.1%) 6(5.9%) |
75(100%) 0(0%) |
276(92.%) 24(8%) |
0.001 |
| Fructose Concentration (g/dl) |
Normal Abnormal |
114(92.7%) 9(7.3%) |
78(76.5%) 24(23.5%) |
69(92%) 6(8%) |
261(87%) 39(13%) |
NS |
| Antisperm antibody (%) | Absent Present |
93(75.6%) 30(24.4%) |
72(70.6%) 30(29.4%) |
57(76.0%) 18(24%) |
222(74%) 78(26.0%) |
NS |
| Testosterone ng/dl | Normal Abnormal |
93(75.6%) 30(24.4%) |
78(76.5%) 24(23.5%) |
57(76%) 18(24%) |
228(76%) 72(24%) |
NS |
| Progesterone ng/dl | Normal Abnormal |
63(51.2%) 60(48.8%) |
45(44.1%) 57(55.9%) |
48(64%) 27(36%) |
135(45%) 165(55%) |
0.03 |
Table 1: A comparison between Sperm parameters, fructose level, and steroid hormones among infertile males with varicocele, without varicocele, and fertile.
The proportion with sperm viability (>75%), was 117(95.1%), 96(94.1%), and 66(88.0%); asthenospermia (progressive motility >50%) was 117(95.1%), 87(85.3%), and 66(88.0%); oligospermia (sperm density <20×106/mL) was 36(48.8%), 39(88.2%), and 18(24%); azospermia (no sperm in the ejaculate) was 21(17.1%), 6(5.9%), and 0(0%), and teratospermia (morphology <30%) was 120(97.6%), 102(100%), and 72(96%) for infertile without varicocele, with varicocele, and fertile male, respectively. Analyzing of seminal fluid samples revealed significant differences in sperm viscosity, sluggish motility, and immotility (P<0.05).
Seminal fructose concentration was estimated among our study groups. The mean ranges of fructose in the seminal plasma was 102- 1040, 35-671, and 113-909 mg/dl in infertile males without varicocele, with varicocele, and fertile, respectively. No significant differences in the level of seminal fructose among infertile and fertile males were recorded. MAR test was used to detect sperm autoantibodies in the seminal plasma. ASA was present in 30(24.4%) infertile male without varicocele, 30(29.4%) infertile with varicocele, and in 18 (24%) fertile males. These results showed no significant differences.
Progesterone and testosterone in the serum
The mean ranges values for serum testosterone and progesterone were: (140-1342), (173-903), and (42-788) ng/dl for testosterone, while (0.15-0.86), (0.15-1.10), and (0.09-0.89) ng/ml for progesterone in males with varicocele, without varicocele, and fertile males, respectively (Table 1). However, no significant differences appeared in testosterone concentration between infertile and fertile group. Progesterone level was found to be significant among infertile and fertile cases.
Trace elements concentration in the seminal fluid
The mean concentration of Na, K, Ca and Cu in the seminal fluid among infertile male without varicocele was 1541, 777, 125 and 1.9 μg/ml as compared to 1375, 764, 115 and 2.0 μg/ml for infertile with varicocele and 1703, 883, 150 and 1.7 μg/ml for fertile male (Table 2 and Figure 1). This decreases in K and Ca among infertile as compared to fertile males appeared significant (0.001, 0.04 respectively). However, Na and Cu showed a non-significant difference among infertile without varicocele, infertile with varicocele and fertile males.
| Infertility status | Na µg/ml means ±SD |
K µg/ml means ±SD |
Ca µg/ml means ±SD |
Cu µg/ml means ±SD |
|---|---|---|---|---|
| Infertile without varicocele |
1541.6 ±665.8 | 776.8± 379.7 | 124.8±114.15 | 1.88±1.623 |
| Infertile with varicocele |
1374.9±626.5 | 764.1±484.1 | 115.4±90.02 | 1.961±2.054 |
| Fertile male | 1703.4±853.5 | 883.5±464.3 | 150.39±118.71 | 1.73±1.83 |
| P value | NS | 0.001 | 0.04 | NS |
Table 2: Trace elements concentration among infertile and fertile males.
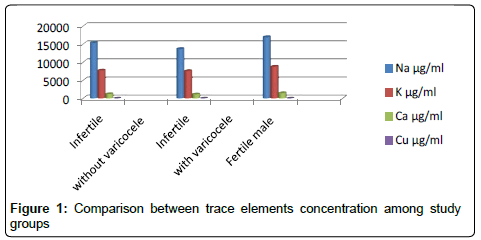
Figure 1: Comparison between trace elements concentration among study
Trace elements and steroid hormones
The concentration of trace elements measured in the seminal plasma and their relation to hormones in the serum are presented in Table 3. The mean Cu was highly significantly (p=0.001) among cases of normal and abnormal increases in progesterone and testosterone concentration. While Na, K, Ca showed a non-significant in cases with normal and abnormal progesterone levels.
| Testosterone ng/dl | Na µg/ml Mean ±SD | K µg/ml Mean± SD | Ca µg/ml Mean± SD | Cu µg/ml Mean± SD | |
|---|---|---|---|---|---|
| Abnormal | 1648.7 (811.3%) | 837.5 (400.1%) | 137.7 (101.5%) | 1.72 (1.86%) | |
| Normal | 1486.4 (677.4%) | 787.1 (452.2%) | 124.9 (110.4%) | 1.92 (1.81%) | |
| Total | 1525.4 (713.8%) | 799.1 (440.1%) | 128.0 (108.3%) | 1.87 (1.82%) | |
| P- value | NS | 0.001 | NS | NS | |
| Progesterone ng/dl | Abnormal | 1458.8 (670.4%) | 467.9 (410.1%) | 125.2 (106.5%) | 1.46 (1.34%) |
| Normal | 1606.7 (758.2%) | 841.0 (472.5%) | 131.4 (110.7%) | 2.36 ( 2.18%) | |
| Total | 1525.4 (713.8%) | 799.1 (440.1%) | 128.0 (108.3%) | 1.87 (1.82%) | |
| P- value | NS | NS | NS | 0.001 |
Note: Normal value for testosterone= 262-1593 ng/dl, progesterone= 0.27- 0.9 ng/dl, and fructose= 120-500 g/dl
Table 3: Means of Na, K, Ca, and Cu concentrations in relation to progesterone and testosterone concentration in the serum of the study groups.
Trace elements and seminal fluid parameters
Semen parameters were divided into two groups (normal and abnormal), according to the WHO recommended reference values (WHO, 2010) and the level of Na, K, Ca, and Cu were compared between these two groups using rank sum tests (Table 4). The mean concentrations of Na and K was increases significantly (p=0.05- 0.001) in cases with viability, motility, sluggish and immotile sperms. However, Ca and Cu was slightly increase in cases with abnormal viability, motility, sperm count (p<0.05). No significant correlation was observed between Na, K, and Ca and fructose seminal fluid parameter. On the other hand, there were significant differences (p<0.05) in Cu concentrations between men with normal and abnormal sperm fructose. Mean serum Cu level in cases with abnormal sperm viability, volume, fructose and ASA was 1.93, 1.81, 2.22 and 1.99 μg/ ml compared to 1.09, 1.88, 1.82 and 1.53 μg/ml in cases with normal values, respectively (p<0.05).
| Na µg/ml Mean ±SD | K µg/ml Mean± SD | Ca µg/ml Mean± SD | Cu µg/ml Mean± SD | ||
|---|---|---|---|---|---|
| Viability (%) | Abnormal | 1546 (721.8%) | 808.0 (441.8%) | 130.5 (107.2%) | 1.93 (1.85%) |
| Normal | 1245 (534.2%) | 681.4 (407.9%) | 94.31 (119.3%) | 1.09 (1.12%) | |
| P-value | NS | 0.01 | 0.001 | 0.003 | |
| Volume (ml) | Abnormal | 1592 (834.3%) | 823.85 (366.9%) | 159.5 (123.1%) | 1.81 (2.09%) |
| Normal | 1508 (681.3%) | 792.9 (457.1%) | 122.6 (103.8%) | 1.88 (1.75%) | |
| P-value | 0.002 | 0.01 | 0.05 | NS | |
| progressive motility (%) q | Not existed | 1555 (723.8%) | 814.6 (446.8%) | 134.8 (110.3%) | 1.90 (1.85%) |
| existed | 1255 (556.8%) | 659.5 (350.2%) | 66.69 (63.83%) | 1.59 (1.57%) | |
| P-value | 0.01 | 0.008 | 0.008 | NS | |
| Sperm morphology (%) | Abnormal | 1835 (483.8%) | 991.7 (110.7%) | 107.1 (110.3%) | 1.85 (1.82%) |
| Normal | 1328 (689.7%) | 731.5 (343.8%) | 150.9 (68.45%) | 2.66 (2.34%) | |
| P-value | 0.001 | 0.02 | 0.02 | NS | |
| Sluggish motility (%) | Not existed | 1271 (584.2%) | 674.1 (265.1%) | 69.02 (79.35%) | 2.29 (2.21%) |
| Existed | 1559 (723.8%) | 816.3 (456.6%) | 136.1 (109.3%) | 1.81 (1.76%) | |
| P –value | NS | NS | 0.001 | NS | |
| Immotile sperm (%) | Not existed | 1269 (632.9%) | 648.1 (253.5%) | 74.55 (91.98%) | 2.37 (1.79%) |
| Existed | 1547 (717.1%) | 812.2 (450.6%) | 132.69 (108.4%) | 1.83 (±1.82%) | |
| P-value | NS | NS | 0.001 | NS | |
| Count x106/ml | Abnormal | 1486 (666.6%) | 826.1 (411.4%) | 142.6 (1167%) | 2.03 (1.90%) |
| Normal | 1550 (743.2%) | 781.9 (457.8%) | 118.6 (101.7%) | 1.772 (1.77%) | |
| P-value | 0.03 | NS | 0.03 | NS | |
| Fructose | Abnormal | 1415 (638.2%) | 649.9 (374.4%) | 125.3 (93.18%) | 2.22 (2.12%) |
| Normal | 1541 (724.1%) | 821.4 (445.4%) | 128.4 (110.5%) | 1.82 (1.77%) | |
| P- value | NS | NS | NS | 0.05 | |
| ASA (%) | Negative | 1525 (690.5%) | 794.0 (43.2%) | 121.7 (109.1%) | 1.99 (1.87%) |
| Positive | 1524 (781.1%) | 813.6 (433.8%) | 145.9 (104.6%) | 1.53 (1.64%) | |
| P –value | NS | NS | NS | 0.006 |
Table 4: Means of Na, K, Ca, and Cu concentrations in relation to sperm count, volume, viability, motility, fructose, leukocyte and the presence of sperm autoantibody.
Male factor infertility has been estimated to account for approximately 50% of all problems with fertility. These problems either interfere with the sperm production process or disrupt their motility after production. Population-based studies are needed to investigate the trends in male reproductive disorders and to explore environmental factors influencing male reproductive health. Patients with and without varicocele tend to have a statistically different semen parameters as compared with fertile regarding sperm viscosity, sluggish and immotile sperms, in addition to progesterone level (p=0.05, 0.001, 0.001, and 0.05, respectively). These results are in accordance with previous studies that demonstrated the detrimental effect of varicocele on sperm quality [26-28]. However, they revealed the association of varicocele with the stress sperm pattern in the form of increased number of abnormal forms, decreased progressive motility and sperm density. In addition, a significant differences was reported in the level of progesterone mainly cases with varicocele group which explained their importance as an infertility determinant among varicocele-related infertility. In addition, viscosity of ejaculate was reported to occur more frequently among infertile couples than in fertile [29]. The importance of semen viscosity lies in the fact that the spermatozoa are tangled in the mucoid mass in the semen and prevented from migrating into the cervical tract to ascend the site of fertilization [30]. Several conditions, such as concentrations of prostate-specific antigen, zinc, calcium, and activity of neutral α-glucosidase in seminal plasma, were found to be correlated with abnormal semen viscosity [31,32].
Some trace amounts of metals are essential for physiological homeostasis; it is well known that excessive or insufficient concentrations of these elements will induce toxicity and deficiency symptoms. The result of other studies showed significance differences of seminal plasma copper concentration between infertile and fertile males, while in recent study there was no significant correlation between seminal plasma copper concentration and infertility.
In the present study the trace elements (Cu, Ca, K and Na) in the seminal plasma of infertile men were investigated and compared to fertile. Semen from infertile male with and without varicocele appeared to contain a significant low concentration of K and Ca (p=0.001, 0.04, respectively) compared to fertile males, while, Cu and Na levels were not.
Although, the role of copper in male reproductive capacity appears to be largely unknown, but this metal appears to be involved in spermatozoa motility and it may also act at the pituitary receptors which control the release of LH [23,33,34] demonstrated a weak but significant positive correlation between blood copper concentrations and sperm motility. The recent study was not in agreement with above both studies.
This study showed that the seminal plasma calcium level was significantly lower in the infertile men compared to the fertile controls (p<0.05). Wong et al. [23] in his study in Netherland reported similar findings of low Ca in the seminal plasma of infertile men which accounts for hypomotility. This has demonstrated the importance of calcium in sperm physiology, including motility [5] metabolism [35], acrosome reaction and fertilization [36]. It is known that calcium is required to initiate the acrosome reaction with its attendant release of enzymes and membrane alterations needed for successful egg-sperm interaction. This accounts for the significantly higher seminal plasma calcium level in normospermic compared to the oligospermic, azoospermic and asthenoligospermic subjects. Calcium is also necessary for maximum motility of sperm cells.
Semen volume, morphology and motility showed a significant difference between normal and abnormal with Ca, Na and K but nonsignificant with Cu indicating that the higher the volume of semen the more will be the concentration of Ca, Na and K in the seminal fluid. This finding agrees with the observation of Kanwal et al. [37] who reported that Ca related to semen volume in bull. Abdel-Rahman et al. [22] also reported a positive correlation between K and semen volume. In the same vein, Na and K showed a positive and significant correlation with sperm motility. This signifies that the progressive active movement of spermatozoa may be improved or increased with higher concentration of Na, Na and K in the seminal fluid of the bucks. This is in contrary to the report by Kaya et al. [38] who observed a negative correlation between sperm motility and Na and K concentrations in ram. However, a positive but non-significant correlation of r = 0.17 has been reported by Kanwal et al. [37] between K and sperm motility in bull. Intracellular calcium (Ca) is essential for the sperm motility, metabolism and acrosomal reaction [39]. Potassium and sodium are also present in high concentrations in the seminal plasma that have the great role in acrosomal reactions [40].
Examinations of the seminal plasma suggest that the concentrations of all elements were within the physiological limits and comparable to the results of other authors [41-43], their concentrations were significantly (p<0.001) higher in the infertile group compared to other groups. As we found no data available to compare and discuss our detected statistical differences, we assume that unlike the blood plasma, the seminal plasma does not have a proper filtration system and therefore acts as an accumulator of any organic or inorganic substance. At the same time, lower concentrations of chemical elements in the sperm cells prove that spermatozoa lack a typical cytoplasm as a source of potential binding molecules for the minerals. Nonetheless, we have to be aware of the fact that the content of chemical elements within spermatozoa may vary and is highly dependent on the concentration of the sperm cell within the ejaculate. The results of this study may give an indication about the involvement of trace elements as an important etiological role in the pathogenicity of unexplained infertility and therapeutic intervention with these elements supplement in a suitable formula may be beneficial and might give a promise in this respect.