Journal of Cancer Research and Immuno-Oncology
Open Access
ISSN: 2684-1266
ISSN: 2684-1266
Case Report - (2018) Volume 4, Issue 1
Sertoli-Leydig cell tumor of the ovary represents less than 0.5% of all ovary neoplasms. It is a tumor that affects predominantly young woman, who most of the times associate signs of virilization. It has recently been associated with mutations in DICER1. In this report, we describe a case of Sertoli-Leydig cell tumor in an asymptomatic 61- year-oldwoman who underwent a laparoscopic bilateral anexectomy for a heterogenous cystic lesion found in her left ovary. The microscopic examination of the lesion, showed a solid-cystic tumoral proliferation in the region identified as ovarian hilum, formed by two distinct and intermixed cell populations (Leydig cells and Sertoli cells). The prognosis of this kind of tumor is usually good, unless it shows poor differentiation and/or heterologous elements or retiforme pattern. So, the recommended treatment of these tumors, is a conservative approach. In our case, the anexectomy was performed by expressed desire of the patient.
Keywords: Androblastoma; Sertoli-Leydig; Ovary; Postmenopausal woman; Anexectomy
Sertoli-Leydig cell tumor of the ovary (as called Androblastoma) is a rare entity composed of variable proportions of Sertoli cells, Leydig cells, and sometimes primitive gonadal stroma and heterologous elements [1].
This lesion accounts for less than 0.5% of all ovary neoplasms, but it represents the most common androgenic functioning tumor, due to it can secrete testosterone, and less frequently human chorionic gonadotropin (HCG) and α-fetoprotein (AFP) [2,3]. Sertoli-Leydig cell tumor of the ovary affects predominantly young women, 40-60% of whom associate signs of virilization [1].
We present a case of a Sertoli-Leydig cell tumor of the ovary in a postmenopausal woman without any evident signs of virilization or other symptoms.
This report presents the case of an asymptomatic 61-year old woman, postmenopausal since 9 years ago and without sexual relations to date, to whom in a routine medical examination (2.5 years before) a heterogeneous cystic lesion in the left ovary is incidentally detected. This lesion measured 33 × 23 mm and showed a multicavitated cystic area of 20 mm with an anecogenic content and a dense portion in the lower pole of 13 mm. This lesion was classified ultrasonographically as GIRADs3 (probably benign), thus, the patient was follow with ultrasound and analytic controls (which includes tumor markers) every 6 months. No changes were observed during the following 2.5 years.
At this moment, we decided to realize a MRI which could not rule out a cystic epithelial neoplasm, and because of this (and by expressed desire of the patient) we decided to do a laparoscopic bilateral anexectomy without hysterectomy (to avoid comorbidities). During the surgery, it was observed a benign macroscopically cystic lesion in the left ovary, which was extracted laparoscopically in the way of integral pieces inside a surgical bag.
The right ovary showed only a yellow and microcystic area on its surface which measured 9 × 8 mm and microscopically represents a hyperthecosis area within an ovarian stromal hyperplasia.
The left ovary is multifragmented, for what is received multiple small yellow fragments which occupy an approximate volume of 1 cc and a bigger cystic like fragment which measured 3.5 cm in diameter (Figure 1). It was accompanied by a fallopian tube without macroscopic alterations.
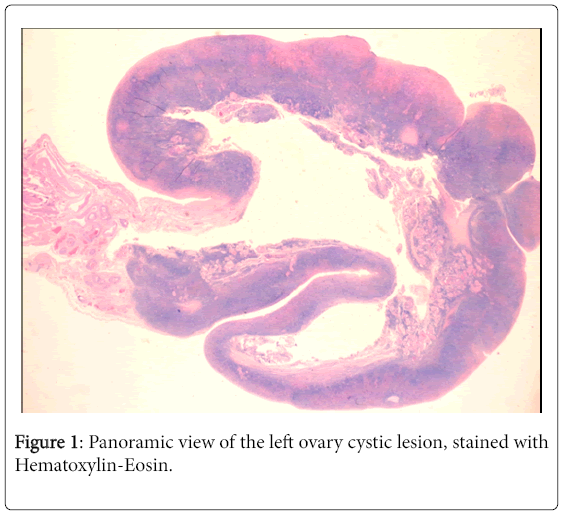
Figure 1: Panoramic view of the left ovary cystic lesion, stained with Hematoxylin-Eosin.
At microscopic evaluation, a solid-cystic tumoral proliferation with little fibrocellular stroma and abundant dilated and hialinized sanguine vessels are observed in the region identified as ovarian hilum (Figure 2A), without areas of tumoral necrosis, pleomorphism or significant mitotic activity. This proliferation is formed by two distinct and intermixed cell populations (Figure 2B). The first one corresponds to medium-sized Leydig cells, with a central nucleus and striking nucleolus, showing large granular cytoplasms with fine deposits of a pinkish-gray pigment and frequent eosinophilic cytoplasmic inclusions (Figure 2C). However, no clear Reinke crystalloids were identified. The second cell population is formed by Sertoli cells arranged forming small ovoid tubules or irregular solid areas (Figure 2D). These cells showed polygonal nuclei and clear, poorly delimited cytoplasms.
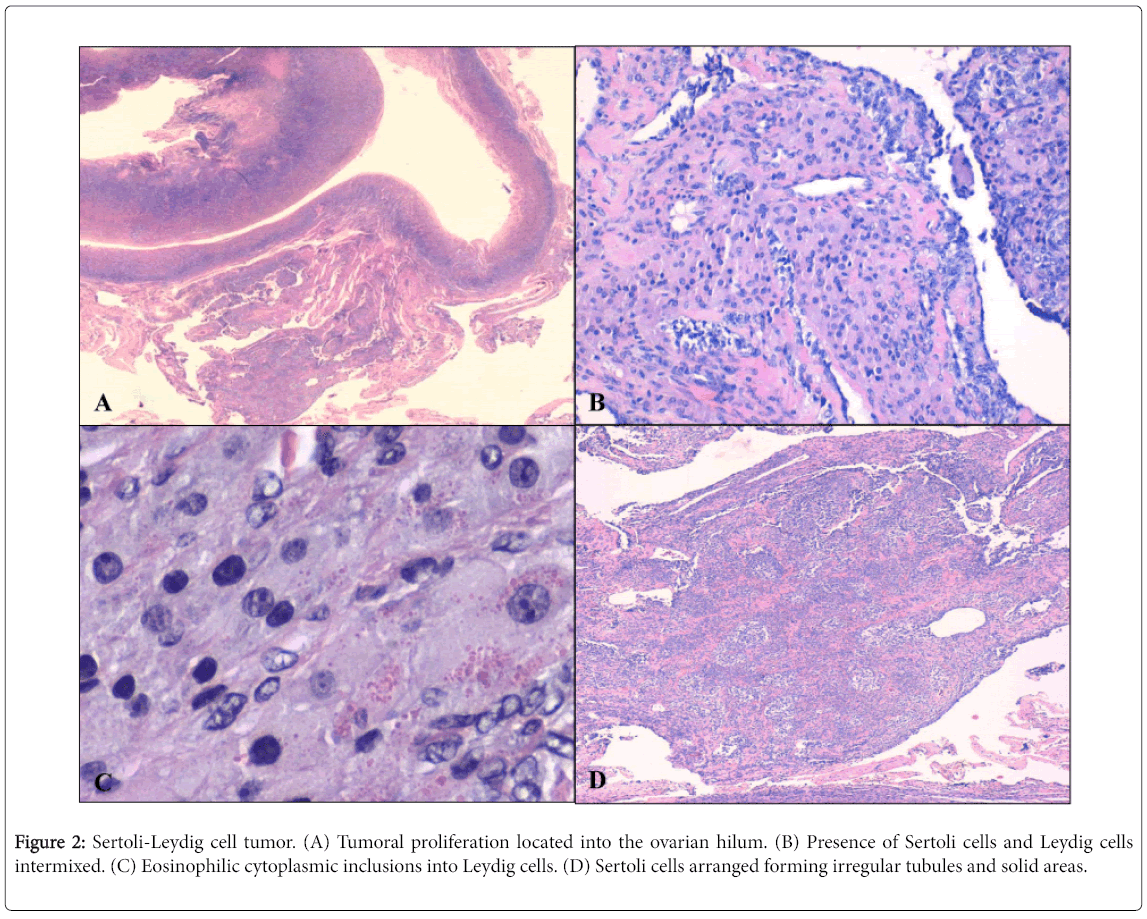
Figure 2: Sertoli-Leydig cell tumor. (A) Tumoral proliferation located into the ovarian hilum. (B) Presence of Sertoli cells and Leydig cells intermixed. (C) Eosinophilic cytoplasmic inclusions into Leydig cells. (D) Sertoli cells arranged forming irregular tubules and solid areas.
Immunohistochemistry (Figure 3) demonstrates intense and diffuse expression of Calretinin, WT-1 (Figure 3D), androgen receptors and vimentin in both cell populations. Further, the expression of Melan-A (Figure 3C), CD99 and α-inhibin (Figure 3B) was irregular (in both cell populations, as well) but more intense into Leydig cells. Estrogen and progesterone hormone receptors, and c-Kit showed weak and focal staining. Expression of EMA, PLAP, Racemase, CD10, CK7, CA125 or CA19.9 was no identified at all. MIB1 and Ki67 were less than 1%.
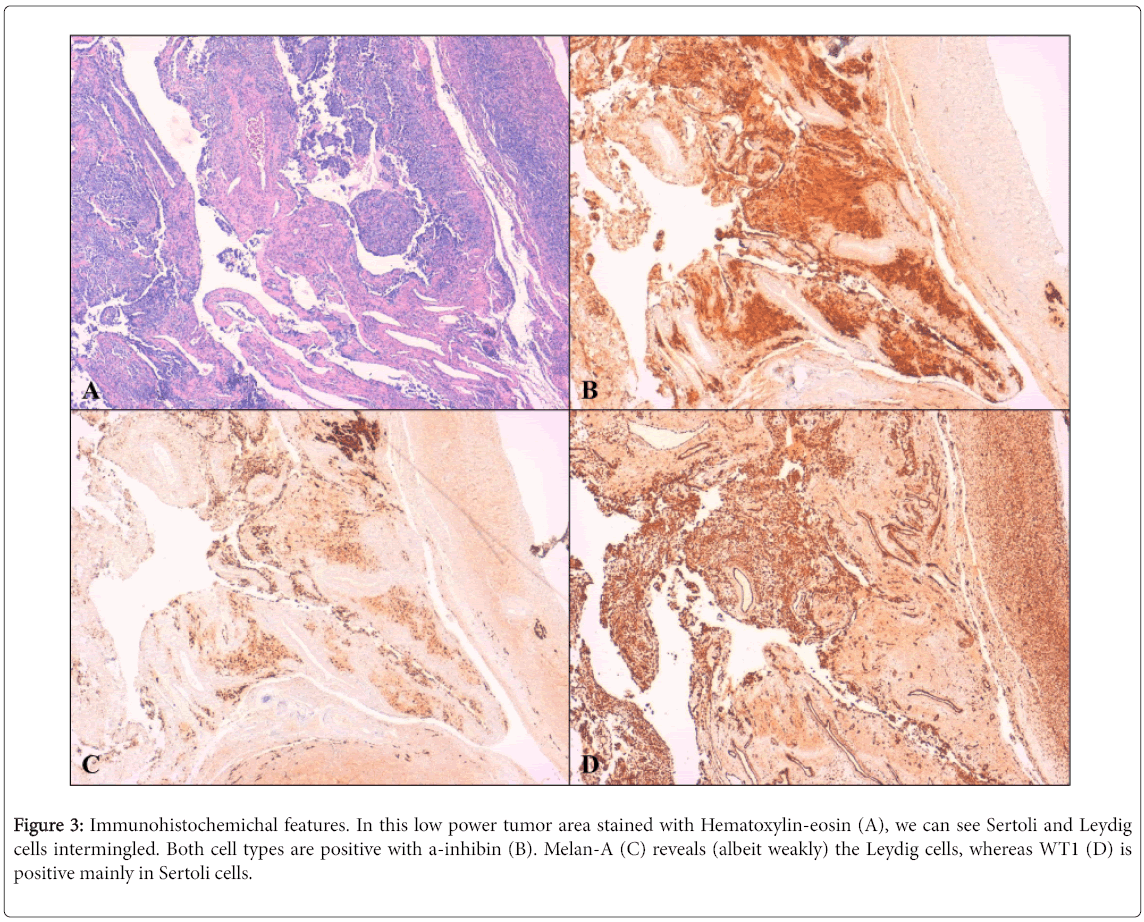
Figure 3: Immunohistochemichal features. In this low power tumor area stained with Hematoxylin-eosin (A), we can see Sertoli and Leydig cells intermingled. Both cell types are positive with a-inhibin (B). Melan-A (C) reveals (albeit weakly) the Leydig cells, whereas WT1 (D) is positive mainly in Sertoli cells.
In view of all these findings, a Sertoli-Leydig cell tumor, moderately differentiated and stage pT1c (limited to the ovary, with a broken capsule) was diagnosed. Although the left ovary was sent with a broken capsule, the fact that this break occurred inside a surgical bag and outside a surgical field, was the reason why this patient did not need more treatment or special follow-up. At the moment, the patient is being follow-up with ultrasound and analytic controls, and all the features are normal to date.
We have reported a case of Sertoli-Leydig cell tumor of the ovary in a postmenopausal woman, which was identified incidentally in a routine physical examination. This tumor is classified as mixed sex cord-stromal tumors in the last WHO classification (2014) [1].
Usually, the patients affected by this tumor were young women with virilization signs. Our patient doesn’t show any virilization or other signs which indicates the presence of this tumor.
The recommended treatment of these tumors, is a conservative approach, being considered enough a simple anexectomy in young patients [4]. However, in postmenopausal women, it has been recommended to do a hysterectomy with double anexectomy [5]. Other more aggressive treatments (radiotherapy or chemotherapy) are advisable in tumors with bad prognostic factors (high stage, poorly differentiated, heterologous elements, etc.).
The prognosis of this tumor is usually good, due to the fact that 80% of them are in stage IA of FIGO, fully encapsulated, and moderately differentiated. Tumors with poor differentiation and/or heterologous elements or retiform pattern, have worse prognosis. In general, this tumor do not metastasize (being rare node metastasis [1]); however the need a periodic follow-up with measurement of hormonal level (total testosterone and SHBG). Recently there has been an association between Sertoli-Leydig tumor and germline mutations in DICER1.
They are usually hereditary cases with familiar history, and which also show multinodular goiter and/or rare tumors like pleuropulmonary blastoma (especially in infants and young children), Willms tumor or cervical rabdomiosarcoma [6,7].