Biochemistry & Pharmacology: Open Access
Open Access
ISSN: 2167-0501
ISSN: 2167-0501
Review Article - (2014) Volume 3, Issue 5
Background: Diabetes mellitus has reached epidemic proportions in many countries. Current challenges in diabetes mellitus management include: optimizing the use of currently available therapies to ensure adequate glycemic, blood pressure, and lipid control and to reduce complications. Aim of the review is to provide a brief overview of recent advancement in diabetes mellitus management. Method Different published articles were reviewed systematically. Result Current standard of care for Type 2 Diabetes mellitus consists of screening for elevated HbA1c levels or, in some cases, fasting plasma glucose, with diagnosis followed by management with lifestyle modifications and metformin. While Insulin, along with diet, is crucial to the survival of individuals with Type 1 Diabetes Mellitus. Despite the known benefits of lifestyle modification, and insulin therapy many individuals still find it harder to maintain a healthier life because of the higher possibilities of sedentary behavior and overeating in the modern world. The success of antidiabetes medication has also been limited by their mechanisms of action, and undesirable side effects. The past 10 years have seen an explosion in the number of new treatments available for diabetes and there are a number of exciting new drugs in development to achieve these goals including oral insulin, islet and pancreatic cell transplant, gene therapy, the incretins, dipeptidyl peptidase-4 inhibitors, peroxisome proliferator-activated receptor inhibitors, and sodium–glucose cotransporter inhibitors to treat Type 2 diabetes Mellitus. Conclusion Current standard of care for diabetes management is not sufficient to provide long run benefits to diabetes patients. Therefore, future remedies with the modifications in insulin delivery system and pharmacogenetic therapeutic approaches could possibly provide the much nodded effect and changes the outcome of diabetes management with new outlook.
<Keywords: Advancements in diabetes pharmacotherapy, Recent advances in diabetes management, Advances in diabetes management, Novel diabetes management, Novel diabetes management approaches
Diabetes mellitus (DM) is a group of metabolic disorders characterized by a complete lack of insulin, a relative lack of insulin, or insulin resistance [1,2] and accompanying with hyperglycemia [3]. DM is likely to become one of the most prevalent and economically important diseases of the twenty 1st century [3]. It has reached epidemic proportions in many countries [4] and is the 3rd leading cause of death for older adults only next to Alzheimer’s and influenza/pneumonia [5].
The prevalence of type 2 DM (T2DM) is predicted to increase dramatically over the coming years [6]. The number of people affected by DM is expected to rise up to 35% by the year 2025 globally [1]. In the US, approximately 1 to1.5 million patients, most of them children, have been diagnosed with type 2 DM (T1DM). The economic cost in the US is estimated at $8 to $14 billion per year [7].
The increase in prevalence of DM is due to three influences: lifestyle, ethnicity, and age [1]. A number of developments has been tried to counteract the resulting impact on morbidity and mortality. Despite the known benefits of lifestyle modification, many individuals still find it harder to maintain a healthier life because of the higher possibilities of sedentary behavior and overeating in the modern world [6].
Patients who are diagnosed with diabetes have a glycated hemoglobin (HbA1c) level of 6.5% or more, fasting plasma glucose (FPG) of 126 mg/dl (7.0 mmol/l) or more, 2 hour postprandial glucose (PPG) of 200 mg/dl (11.1 mmol/l) or more, or random plasma glucose level of 200 mg/dl (11.1 mmol/l) or more [8,9].
Current challenges in diabetes management include: optimizing the use of currently available therapies to ensure adequate glycemic, blood pressure, and lipid control and to reduce complications; educating patients on diabetes self-management; improving patient adherence to lifestyle and pharmacologic interventions; reducing barriers to the early use of insulin; and improving the delivery of health care to people with chronic conditions [10].
The past 10 years have seen an explosion in the number of new treatments available for diabetes and there are a number of exciting new drugs in development to achieve these goals [11]. Technological solutions are focused on the delivery of insulin and glucagon via an artificial pancreas, and components of the system are already in use, suggesting this option may well be available within the next 10 years [6]. The aim of this article is to provide a brief overview of current updates on diabetes management for clinical usage.
Although diabetes has been recognized since antiquity, treatments of diabetes has only been understood experimentally since about 20th century. The discovery of insulin in 1921 by two Canadian researchers, Sir Frederick Banting and Charles Best set about a series of global events that continue to influence the development of diabetes treatment today [12] (Figure 1). Fifty years ago patients with diabetes were mostly treated in hospitals by specialists, but the sharp rise in the prevalence of T2DM means that this is no longer practical. Since the 1970s increasing numbers of primary and community healthcare professionals have assumed responsibility for the routine review, monitoring and management of patients with diabetes [13].
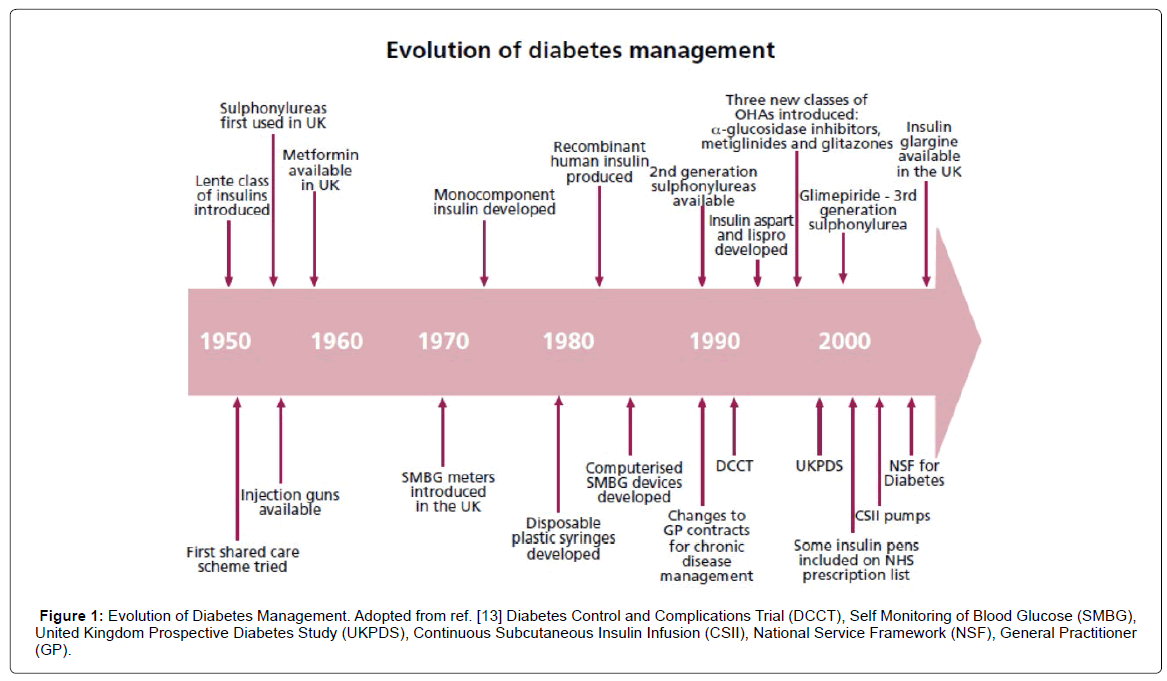
Figure 1: Evolution of Diabetes Management. Adopted from ref. [13] Diabetes Control and Complications Trial (DCCT), Self Monitoring of Blood Glucose (SMBG), United Kingdom Prospective Diabetes Study (UKPDS), Continuous Subcutaneous Insulin Infusion (CSII), National Service Framework (NSF), General Practitioner (GP).
Pathogenesis
The distinction between T1DM and T2DM was first clearly made by Sir Harold Percival Himsworth, and published in January 1936 [14]. The loss of insulin secretion in T1DM results from autoimmune destruction of the insulin-producing β-cells in the pancreas, which is thought to be triggered by environmental factors, such as viruses or toxins, in genetically susceptible individuals. This form of diabetes is associated closely with histocompatibility antigens (human leukocyte antigen [HLA]-DR3 or HLA-DR4) and the presence of circulating insulin antibodies, including insulin antibody, glutamic acid decarboxylase antibody, islet cell antibody (ICA), and islet cell antibody 512 (a tryosine phosphatase antibody) [15,16].
T2DM is characterized by impaired insulin secretion and resistance to insulin action. In the presence of insulin resistance, glucose utilization by tissues is impaired, hepatic glucose production is increased, and excess glucose accumulates in the circulation. Genetic predisposition may play a role in the development of T2DM. People with T2DM have a stronger family history of diabetes than those with type 1. There is no association with HLA types, however, and circulating ICAs are absent [15-17].
Current Therapeutic Approaches
Research activity in the field of diabetes has increased greatly in recent years [3] and current standard of care for T2DM consists of screening for elevated HbA1c levels or, in some cases, fasting plasma glucose, with diagnosis followed by management with lifestyle modifications and metformin except where contraindicated (Figure 2) [6].
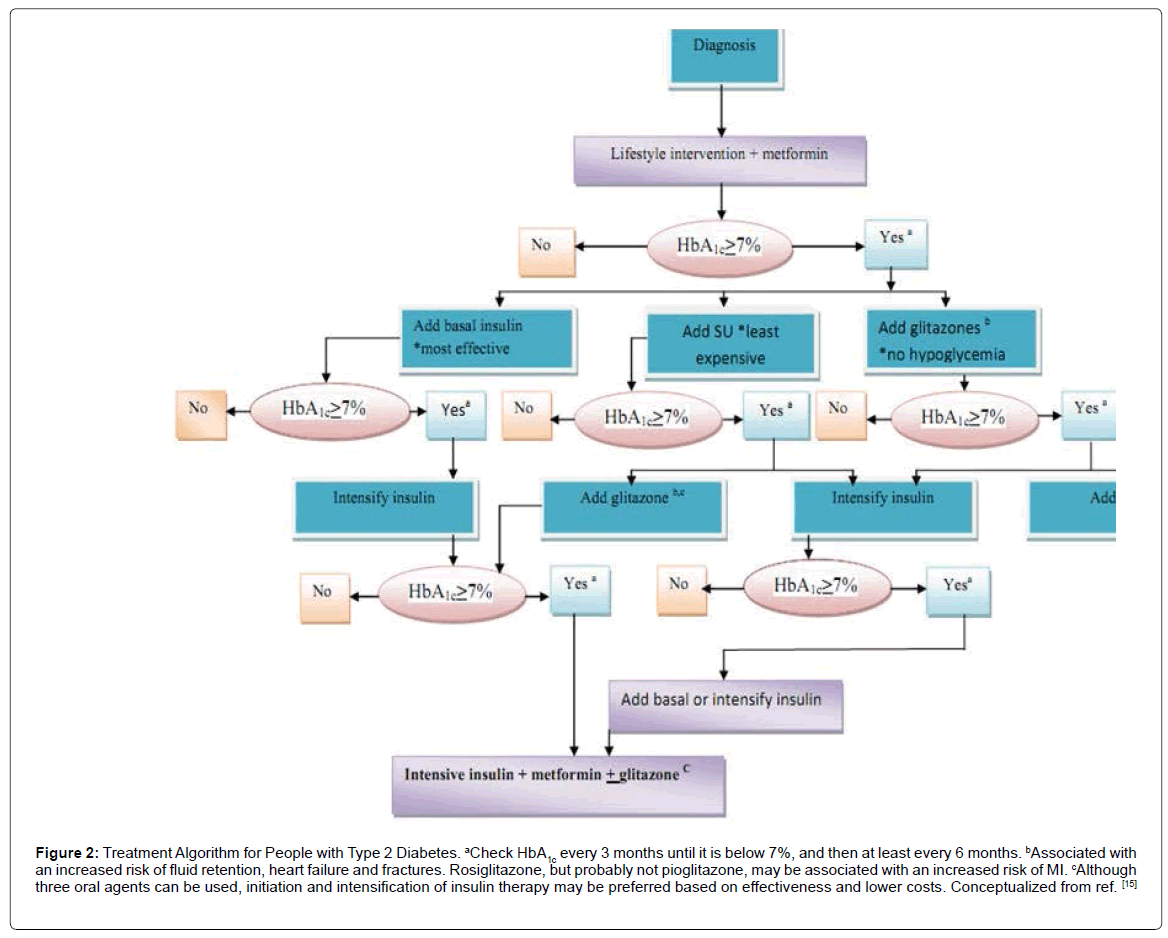
Figure 2: Treatment Algorithm for People with Type 2 Diabetes. aCheck HbA1c every 3 months until it is below 7%, and then at least every 6 months. bAssociated with an increased risk of fluid retention, heart failure and fractures. Rosiglitazone, but probably not pioglitazone, may be associated with an increased risk of MI. cAlthough three oral agents can be used, initiation and intensification of insulin therapy may be preferred based on effectiveness and lower costs. Conceptualized from ref. [15]
Insulin, along with diet, is crucial to the survival of individuals with T1DM. Insulin can also be used for patients with T2DM during periods of intercurrent illness or stress (e.g., surgery, pregnancy). The use of antidiabetic agents is reserved for the treatment of patients with T2DM whose symptoms cannot be controlled with diet and exercise alone [15].
For patients who do not achieve HbA1c targets, antidiabetes medications are added to metformin; subsequently, patients are monitored and further oral antidiabetes drugs or insulin are added if needed [6]. Sulphonylureas like glipizide, glimepiride and gliclazide, as second-generation oral hypoglycaemic agents (OHAs) are effective at lowering glucose level, but are designed to have a shorter duration of action and so are associated with a reduced risk of hypoglycaemia [11].
The success of OHAs is limited by their mechanisms of action, which often address the symptoms of diabetes rather than its underlying pathophysiology. OHAs may also have undesirable side effects. For instance, up to 2.5% and 17.5% of sulfonylurea (SU) treated patients experience major and minor hypoglycemia, respectively, while GI problems affect up to 63% of metformin, 36% of thiazolidinedione (TZD), and 30% of acarbose treated patients. Peripheral edema is observed in up to 26% of TZD-treated patients, and body weight increases of 2.2 to 11.0 lb (1 to 5 kg) are common with both SU and TZD therapy. These side effects can have a negative impact on patient adherence to treatment, resulting in higher HbA1c levels and increased risk for all-cause hospitalization and all-cause mortality [18-20].
The last 20 years have seen an astonishing pace in research into the molecular pathology of diabetes. The current improved understanding of diabetes has facilitated the development of drug classes that target specific metabolic pathways such as the incretins, dipeptidyl peptidase-4(DPP-4)inhibitors, amylin, pramlintide, peroxisome proliferator-activated receptor(PPAR), endocannabinoids, sodiumglucose co-transporter-2(SGLT2) inhibitors and 11B hydroxysteroid dehydrogenase type 1(11BHSD1) inhibitors (Table 1). A number of studies also trying to address with improved utilization of insulin and modification of the metabolic pathways through pancreatic and isletcell transplantation, generate mature β-cells from embryonic stem cells, gene therapy, implantable insulin pumps with continuous glucose sensing, pulmonary delivery of inhaled insulin and oral insulin [15,16]. In the next 10 years, based on current research, a number of treatment alternatives will be the future options for DM management [6,15,17].
| Sl.no | Antidiabete’s Mechanism | Example of novel drug(s) | status | Ref |
|---|---|---|---|---|
| 1 | Insulinotropic hormones (Incretins) | Exenatide | has been shown to reduce HbA1c in patients with T2DM failing to achieve glycemic control | [53] |
| 2 | SGLT2-inhibitors | Dapagliflozin | Approved by the European Medicines Agency (EMA) | [60] |
| 3 | Inhibitors of 11b hydroxysteroid dehydrogenase type 1 (11BHSD1) | KR-67500 | Potential as treatment for osteoporosis as well as metabolic syndrome DM | [62] |
| 4 | VEGF Inhibitor and Anti-CTGF short hairpin RNA (shRNA) | Ranibizumab and CTGF shRNA | Improves Retinal Gene Expression and Microvessel Ultrastructure in a Rodent Model of diabetes | [63] |
| 5 | Peroxisome proliferator-activated receptor (PPARs) inhibitors | LT175 | the compound improved glucose homeostasis and insulin sensitivity | [59] |
| 6 | Amylin Receptor Agonists (Amylinomimetics) | pramlintide | Stimulate insulin secretion, delays gastric emptying, reduces postprandial glucagon levels, improved satiety | [53] |
| 7 | DPP-4 inhibitors | Sitagliptin | Reduce DDP-4 activity by 80% | [17] |
Table 1: Summary of Some of the Novel Antidiabetic Medications to Treat T2DM Vascular Endothelial Growth Factor (VEGF), Short hairpin RNA (shRNA), Connective Tissue Growth Factor (CTGF), Sodium-glucose co-transporter-2 (SGLT2).
Oral insulin
New approaches for oral administration of insulin are strongly related to novel insulin carriers [21]. Oral route would be the most convenient and preferred route if it is available [22]. The development of improved oral insulin administration is very essential for the treatment of diabetes mellitus to overcome the problem of daily subcutaneous injections. Insulin, when administered orally, undergoes degradation in the stomach due to gastric enzymes [23]. Beside, nanoencapsulated insulin has been found bioactive, as demonstrated through both in vivo and in vitro bioassays [24].
In diabetic patients oral administration of insulin can be beneficial not only to alleviate the pain and trauma caused by injections, but it can mimic the physiological fate of insulin as well [25,26]. The nanomedicine technologies that may be employed for oral insulin delivery include pro-drugs (insulin–polymer conjugation), micelles, liposomes solid lipid nanoparticles (NPs) and NPs of biodegradable polymers [25,27].
Intranasal insulin delivery
Study showed that nasal administration of insulin-loaded, chitosan reduced gold nanoparicles (GNPs) improved pharmacodynamic activity of insulin [28]. These NPs showed good insulin-loading capacity, providing the release of 75% to 80% insulin within 15 minutes after administration [29].
Pulmonary delivery of inhaled insulin
The large alveolar surface area of lung coupled with the thin epithelial barrier and extensive vascularization might enhance drug transport and uptake [30]. The sizes of particles which are used for inhalation therapy are usually expressed in terms of the mass median aerodynamic diameter [31]. Results from phase III clinical trials with insulin administered by the dry-powder inhaler system of Exubera indicate that inhaled insulin formulation given before meals is as effective as mealtime insulin injections [32].
Implantable insulin pumps with continuous glucose sensing
Implantable biological micro electromechanical systems (BioMEMS) can be used as insulin pumps for controlled release of insulin. Interest in BioMEMS is growing rapidly, with opportunities in areas such as biosensors, pacemakers, immunoisolation capsules, and drug delivery [33]. BioMEMS device has a drug reservoir compartment filled with insulin molecules [29]. The small size scale of MEMS, therefore, offers a unique opportunity to take advantage of the capabilities of responsive hydrogels in sensing and valving applications. Hydrogels that swell in response to changes in osmotic pressure, pH or temperature or analyte concentration could be quite useful for sensing applications in vivo [34].
Pancreatic and Islet-cell transplantation
Pancreatic islet allo-transplantation is a procedure in which islets from the pancreas of a deceased organ donor are purified, processed, and transferred into another person [35] to treat T1DM [36] and have been a promising cellular-based therapy [8] (Figure 3); however, it is still viewed as experimental, although utilization of the procedure is growing [37]. This procedure involves portal venous injection of islet cells and affords 1 year insulin independence in as many as 80% of recipients [8].
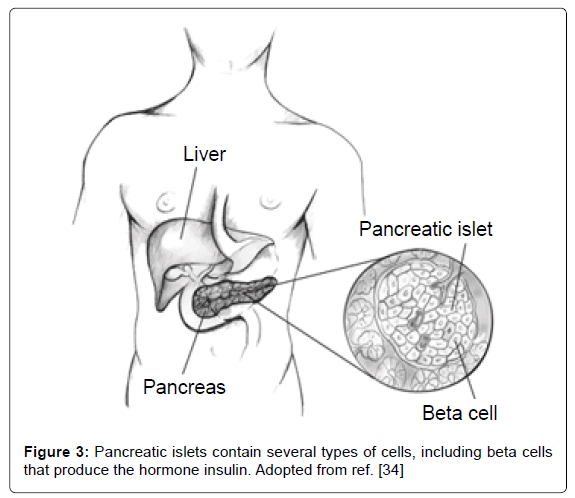
Figure 3: Pancreatic islets contain several types of cells, including beta cells that produce the hormone insulin. Adopted from ref. [34]
Significant obstacles remain including the need for safe and cost-effective differentiation methods for large-scale generation of transplantation quality β-cells, methods to prevent immune rejection of grafted tissues and amelioration of the risks of tumorigenesis [38]. These problems can be tackled by using immunosuppressive medications [35]. Therefore, with the advent of improved immunosuppressive regimens, islet transplantation will become a feasible treatment option for T1DM patients (Figure 4) [39].
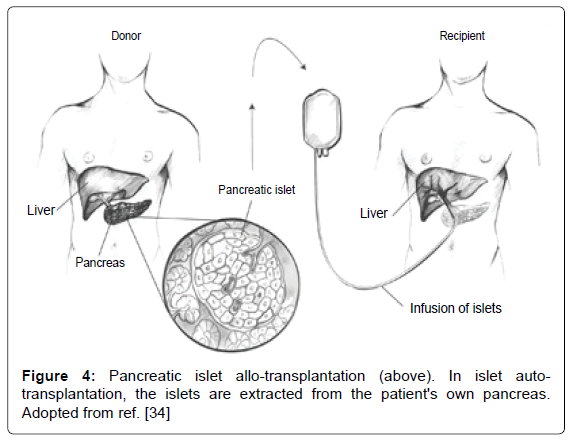
Figure 4: Pancreatic islet allo-transplantation (above). In islet auto-transplantation, the islets are extracted from the patient's own pancreas. Adopted from ref. [34]
Generate mature β-cells from embryonic stem cells
Over the last 15 years, stem cells that can differentiate into all cell types of the human body, including insulin-producing β-cells, have been identified [39]. Generation of mature pancreatic β-cells from embryonic stem (ES) cells in vitro could also provide a therapy for insulin-dependent diabetes mellitus. Recent ES cell differentiation protocols have improved the differentiation efficiency toward β-cells by recapitulating in vivo pancreatic development [40].
Gene therapy
Gene therapy investigators are currently studying approaches to efficiently transfer the insulin gene into other cells such as the liver, stomach, or intestines [41]. A research group in Spain reported that they replaced two genes to cure a dog of T1DM and the result was successful. However, the technology requires more testing before human clinical trial is initiated [42]. Gene therapy investigators are currently studying approaches to efficiently transfer the insulin gene into other cells such as the liver, stomach, or intestines [41].
Incretins
The most recent advances in therapy for T2DM have revolved around the discovery and exploration of the effects of incretins. Incretins are insulinotropic hormones secreted from specialized neuroendocrine cells in the small intestinal mucosa in response to carbohydrate ingestion and absorption [15]. Insulin secretion can be stimulated by the incretin gut hormones glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP) without leading to hypoglycemia. Incretin action is efficient, but short lived [43]. As they enter the blood vessels, incretin undergo rapid metabolism via proteolytic cleavage by dipeptidyl peptidase-4 (DPP-4) to inactive metabolites [15]. Stable analogs of these incretins have been developed with a longer half-life. Exenatide, when injected subcutaneously has been shown to reduce HbA1c in patients with T2DM failing to achieve glycemic control on maximal doses of either metformin alone or metformin/sulfonylurea combination [43].
Dipeptidyl peptidase-4 (DPP-4) inhibitors
The DDP-4 inhibitors inhibit the degradation of GIP and GLP-1 upon entering the GI vasculature, thus increasing the effects of these endogenous incretins on first-phase insulin secretion and glucagon inhibition [44]. Inhibitors of DPP-4 have also been developed and have reached an advanced stage of clinical trial [43]. Both sitagliptin and vildagliptin reduce DDP-4 activity by 80%, with some inhibition maintained for up to 24 hours after an oral dose [15].
Amylin mimetics
Amylin (islet amyloid polypeptide), which is, a glucoregulatory synthesized by the islet β-cells and co-secreted with insulin and deposited within pancreatic islets of diabetics patients [45]. It appears to act centrally to induce satiety, slow gastric emptying and suppress pancreatic glucagon secretion [43]. It also activates G-proteincoupled receptor and triggers multiple common intracellular signal transduction pathways that can culminate in apoptotic cell death. Moreover, amylin receptor antagonists can block both the biological and neurotoxic effects of human amylin. Amylin receptors thus appear to be involved in the pathophysiology of diabetes, and could serve as a molecular link to the epidemiology of the problem [45].
Amylin is absent in patients with T1DM. In patients with T2DM, its concentrations are altered at different points in the progression of the disease [15].
Pramlintide
Pramlintide is a soluble analog of amylin with amylin-like effects which last for about 3 hours after subcutaneous administration prior to a meal. It has been launched in the USA as Symlin®, Amylin pharmaceuticals and is licensed in both T1DM and T2DM as an adjunct to meal-time insulin therapy in those who have failed to achieve desired glucose control despite optimal insulin therapy. One of the main advantage of pramlintide is that, it is not associated with weight gain [3]. Addition of pramlintide to continuous subcutaneous insulin infusion (CSII) therapy was safe and effective in patients with T1DM [46].
Peroxisome Proliferator-Activated Receptor (PPAR) agonists
PPARγ is a nuclear hormone receptor that functions as a master regulator of adipocyte differentiation and development [47]. These receptors are transcriptional factors belonging to the ligandactivated nuclear receptor super-family which directly regulate the expression of a large number of genes involved in adipocyte differentiation, lipid and carbohydrate metabolism as well as adipokine synthesis; thereby they are implicated in various metabolic disorders, including obesity, insulin resistance, dyslipidemia and hypertension [48].
Other exciting drugs in development under PPAR are dual PPAR α and γ agonists, which may treat both hyperglycemia and dyslipidemia, and rimonabant which acts on the endocannabinoid system [3]. These dual PPARα/γ agonists are devoid of the side effects of the marketed antidiabetic agents, thiazolidinediones and the dual-agonists glitazars [49]. Similarly, pseudoginsenoside F11 (p-F11), an ocotillol-type ginsenoside isolated from Panax quinquefolium L. (American ginseng) was found to activates PPARγ with modest adipogenic activity. It also inhibits obesity-linked phosphorylation [47].
Cannabinoid receptor blockers
Endocannabinoids act on cannabinoid type 1 (CB1) and type 2 (CB2) receptors. The endocannabinoid system plays a key role in the regulation of energy balance and fat accumulation and overactivity of the system is associated with increased food intake and fat accumulation. Rimonabant acts as a selective CB1 blocker inducing weight loss, reducing triglyceride levels and improving glucose tolerance. It presents a novel tool to reduce cardiovascular risk factors of the metabolic syndrome including dyslipidemia and T2DM (as well as nicotine dependence). Rimonabant has already obtained regulatory approval as an adjunct to diet and exercise for the treatment of obese patients or over-weight patients with associated risk factors [3].
Sodium-Glucose Co-Transporter-2 (SGLT2) inhibitors
Inhibiting SGLT2 blocks reabsorption of filtered glucose in the kidney, increasing urinary glucose excretion and reducing blood glucose levels. Its mechanism of action is independent of pancreatic β- cell function and modulation of insulin sensitivity [50]. Clinical results are promising with significant lowering of HbA1c without increased risk of hypoglycemia, reduction of body weight and reduction of systolic blood pressure [51].
11B Hydroxysteroid Dehydrogenase Type 1 (11BHSD1) selective inhibitors
11BHSD1 inhibitors have considerable potential as treatment for osteoporosis as well as metabolic syndrome including T2DM. 11BHSD1 inhibitors possess anti-diabetic, anti-adipogenic and anti-osteoporotic activity [52].
Vascular Endothelial Growth Factor (VEGF) Inhibitors
Anti-vascular endothelial growth factor (VEGF) treatment was tried to treat neovascularization and macular edema in diabetes rat. However, it resulted in up-regulation of connective tissue growth factor (CTGF) in the retina, increasing the risk of fibrosis and tractional retinal detachment. A novel dual-target intervention that involves intravitreal injection of the VEGF inhibitor suggest the advantages of dual-target over single-target interventions in diabetic retina and reveal a novel therapeutic modality for diabetic retinopathy .
Safety and Limitations
The major limitations and technological hurdles faced by nanotechnology and its applications in the field of drug delivery should be addressed [54]. Estimating the dose of inhaled particles (dosimetry) requires the knowledge of several mechanisms including regional deposition, retention, solubility, redistribution, translocation into the circulation, metabolism, accumulation in certain organs and the excretion pathways via urine and faeces. The factors that control or affect particle deposition include the particle characteristics themselves, the respiratory tract geometry and individual features of ventilation such as the mode of breathing [55].
The major factors limiting the bioavailability of nasally administered insulin include poor permeability across the mucosal membrane and rapid mucociliary clearance mechanism that removes the non-mucoadhesive formulations from the absorption site. To overcome these limitations, mucoadhesive NPs made of chitosan/ tripolyphosphate [56].
The temporal correlation between rimonabant initiation and onset of depressive symptoms and improvement of depressive symptoms on withdrawal of drug points towards possibility of depressive symptoms due to rimonabant. Therefore, rimonabant can result in new onset depression in patients with schizophrenia and one has to be cautious in initiating rimonabant in such patients [57].
Recent studies have demonstrated the association of endocannabinoid with diabetic nephropathy. Therefore, future investigations should clarify the role of the endocannabinoid system in the development of diabetic nephropathy and within this system, identify potential therapeutics to reduce the burden of this disease [58].
Current standard of care for diabetes management consists of screening for elevated HbA1c levels and fasting plasma glucose followed by management with lifestyle modifications, metformin, insulin, along with diet. However, despite the known benefits all these many individuals still find it harder to maintain a healthier life. A number of diabetes management approaches have been introduced in the past 10 years which will have a real impact on the current therapeutic approaches.
The authors would like to thank Ambo University, for the real effort made and anticipated to be continued; on making available the clinical pharmacy services for Ambo community.
The authors declare no conflict of interests.