Journal of Medical Diagnostic Methods
Open Access
ISSN: 2168-9784
ISSN: 2168-9784
Case Report - (2015) Volume 0, Issue 0
Antineutrophil cytoplasmic antibodies (ANCA) is usually considered to be associated with autoimmune neutropenia, but the association between ANCA and autoimmune pulmonary hemorrhage has been rarely reported. In this case, we reported a 49 year-old woman with paroxysmal cough and hemoptysis. The symptom didn’t improve from any anti-infection treatment. Further autoantibodies analysis reveals ANCA positive (MPO-ANCA 1472.3 AAU/ml, normal <180.0 AAU/ml), and negative anti-GBM antibodies. The patient was diagnosed with microscopic polyangiitis, and was treated with methylprednisolone and cyclophosphamide. After 10 days treatment, the patient’s hemoptysis and paroxysmal cough was eliminated. CT scan also revealed a miniaturized pulmonary lesion. Although rare, ANCA-associated pulmonary lesion should be kept aware when other factors such as infection and toxin cannot explain the severe symptom. Early detection and routine autoantibodies analysis are needed to prevent condition from deteriorating further and minimize mortality.
Keywords: Antineutrophil cytoplasmic antibody (ANCA); Microscopic polyangiitis; Pneumonia
Anti-neutrophil cytoplasmic antibodies (ANCA) is associated with a group of systemic small-vessel vasculitis (arterioles, capillaries, and venules; rarely small arteries) and glomerulonephritis. Granulomatosis with polyangiitis (Wegener's), microscopic polyangiitis, and Churg- Strauss syndrome (EGPA) belong to this group because they are ANCA-positive and have a pauci-immune glomerulonephritis with few immune complexes in small vessels and glomerular capillaries [1].
Microscopic polyangiitis (MPA) is the most common cause of the pulmonary-renal syndrome of alveolar hemorrhage and glomerulonephritis. Patients with MPA who are ANCA positive have antibodies directed against myeloperoxidase (MPO-ANCA) [2]. The majority of patients develop with nonspecific constitutional symptoms including fatigue, fever, glomerulonephritis, migratory arthralgias and palpable purpura [3]. MPA was initially recognized as a particular type of polyarteritis nodosa (PAN) with, in most cases, rapidly progressive necrotizing glomerulonephritis (RPGN) and rare with lung hemorrhage. The proposed feature distinguishing PAN from MPA is the absence of vasculitis in the arterioles, venules, or capillaries. Smallvessel involvement, when present, is the definitive diagnostic criterion of MPA and excludes the diagnosis of PAN, even if medium-sized arterial lesions are seen [4]. This classification minimizes the frequency of a classic PAN diagnosis because small-vessel involvement excludes it.
A 46-year-old lady was admitted to the emergency unit with weakness and fatigue for 5 months, breath-shortness and hemoptysis for 10 days 5 months ago, the patient gradually felt weakness and fatigue after physical activity. She had no cough, no fever, no night sweats and no change in appetite at that time. 4 months ago, she developed paroxysmal cough with hemoptysis after getting up in the early morning. The color of bloody sputum was dark red, and the amount of bleeding was about 2 ml for each time. She denied any fever, nausea, dizziness, and breath-shortness at that time. So she went to the local hospital for examination.
The CT scan on Dec 09, 2014 showed bilateral lung diffuse lesions (Figure 1). No medication was given at that time. 10 days ago, the symptom became worse. She developed breath-shortness, without any chest-pain or chest-tightness.
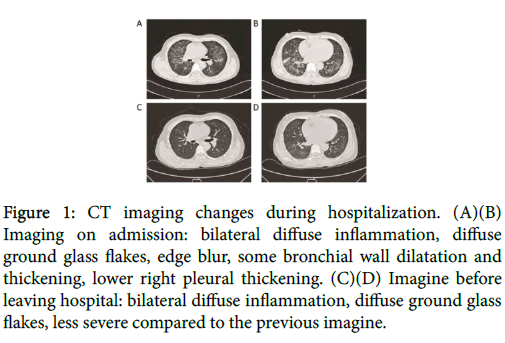
Figure 1: CT imaging changes during hospitalization. (A)(B) Imaging on admission: bilateral diffuse inflammation, diffuse ground glass flakes, edge blur, some bronchial wall dilatation and thickening, lower right pleural thickening. (C)(D) Imagine before leaving hospital: bilateral diffuse inflammation, diffuse ground glass flakes, less severe compared to the previous imagine.
The body weight loose was 5 kg in recent 3 months. In the emergency unit, she was diagnosed with pneumonia. Sulperazone 3g q12h and Mucosolvan 30 mg bid were intravenous admitted to anti-infection and loosen phlegm. On presentation, she is fatigue with anemic appearance. Physical examination is unremarkable except for left lower limb soreness. CT scan on Dec 16, 2014 revealed bilateral lung diffuse inflammation, lower right pleural thickening, Pneumocystis carinii pneumonia considered.
Laboratory studies show an elevated erythrocyte sedimentation rate (ESR, 22 mm/h), anemia (hemoglobin level, 87 g/L). The white blood count was normal (4.7 × 109/L), with a slightly elevated GRAN% (72.2%). The C-reactive protein was 1.4 mg/L (Table 1). All serum infected markers turned out to be almost normal (Table 2). After the therapy in the hospital, the hemoptysis vanished. But paroxysmal cough always existed. Further laboratory studies indicate normal antistreptolysin O (ASO, <56.90 IU/ml), rheumatoid factor (RF, <10.10 IU/ml), and a negative antinuclear antibody. Urine test reveals urine albumen +2, blood +3 and red blood cell +2. 24-hour total urine albumen is 3.242 g (Table 3). Serum creatinine is elevated (91 μmol/ L↑), but serum urea nitrogen is normal (6.50 mmol/L), indicating impaired renal function. Tumor marker test shows a rise in CEA (5.1 ng/mL↑) and CA19-9 (37.4 U/mL↑). Although enough treatment was given, there was no improvement in the symptom. Considered the impairment of kidney function, we held a consultation with the department of nephrology and department of rheumatology. The nephrologist advised to use piperazine ferulate to reduce hematuria and do renal biopsy to confirmed pathological diagnosis. The rheumatologist advised to perform further auto-immune analysis. After overall consideration, we thought the lung and kidney lesion might be explained by a single factor. Therefore, we decided to carry out a complete auto-immune analysis for the patient. The further analysis revealed positive anti-neutrophil cytoplasmic antibodies (ANCA: MPO-ANCA 1472.3 AAU/ml, normal <180.0 AAU/ml, PR3- ANCA <180.0 AAU/ml, normal <180.0 AAU/ml) (Table 4), and negative anti-GBM antibodies. The patient was finally diagnosed with ANCA-associated microscopic polyangiitis. After the diagnosis was clear, she was treated with methylprednisolone 40 mg QD7 every morning and 20 mg QD17 every afternoon by the advice of rheumatologist. Upon the completion of 1 week’s cortisone therapy, the patient’s paroxysmal cough was eliminated, without any other uncomfortable complain, no chest-tightness or breath-shortness, no fever or chill. CT scan on Dec 25, 2014 showed bilateral lung diffuse inflammation, less severe compared to the image 1 week ago. ESR dropped to a normal condition (20 mm/h), and other laboratory indicators better than before. The patient was discharged and asked to receive CTX intravenous injection 0.4 g once a month, following up in the out-patient department.
| Parameter | Normal range | Date | ||||
|---|---|---|---|---|---|---|
| On admission | Day of treatment | After admission | ||||
| 2013/12/12 | 2013/12/17 | 2013/12/19 | 2013/12/21 | 2013/12/27 | ||
| WBC | (4-10) *10^9/L | 4.7 | 4.3 | 4.8 | 5.7 | 8.8 |
| Neutrophils | (2-7)*10^9/L | 2.97 | 2.73 | 2.74 | 2.89 | 2.76 |
| Neutrophils | 50-70 | 72.2 | 70.5 | 74.4 | 74.3 | 82 |
| Lymphocytes | (0.8-4)*10^9/L | 0.74 | 0.86 | 0.86 | 1.09 | 0.95 |
| Monocytes | (0.2-1.2)*10^9/L | 0.37 | 0.35 | 0.34 | 0.34 | 0.62 |
| Eosinophils | (0-1)*10^9/L | 0.19 | 0.02 | 0 | 0 | 0.01 |
| Basophils | (0-0.1)*10^9/L | 0 | 0.03 | 0.03 | 0.03 | 0 |
| RBC | (3.7-5.1)*10^12/L | 2.97 | 2.73 | 2.74 | 2.89 | 2.76 |
| HB | (113-151)g/L | 87 | 83 | 83 | 88 | 86 |
| ESR | 0-20mm/h | 30 | 20 | |||
| CRP | 0-10 mg/l | 1.4 | 1.8 | |||
| SCr | (40-88) µmol/l | 91 | 90 | |||
| BUN | (2.8-7.2) mmol/l | 6.5 | 7.6 | |||
| Urinary protein | N/A | 2+ | ||||
| Urine occult blood | N/A | 3+ | ||||
| Quantitative Urine WBC | <23.0/µL | 15.8 | ||||
| Quantitative Urine RBC | <18.0/µL | 696.3 | ||||
Table1: Basic parameters of the patient.WBC,white blood cell; RBC, red blood cell; HB, hemoglobin;ESR,erythrocyte sedimentation rate;CRP, C reactive protein;SCr, serum creatitine;BUN,blood urea nitrogen.
| Parameter | Normal range | Value |
|---|---|---|
| Adenovirus antibody (ADV-IgM) | N/A | N/A |
| Respiratory syncytial virus antibody (RSV-IgM) | N/A | N/A |
| Influenza virus a antibodies (InfluAIgM) | N/A | N/A |
| Antibodies to influenza virus b (InflB-IgM) | N/A | N/A |
| Parainfluenza virus IgM antibody (PIV-IgM) | N/A | N/A |
| Chlamydia pneumoniae antibodies (MP-IgM) | N/A | N/A |
| Mycoplasma pneumoniaeIgM antibodies (MP-IgM) | N/A | N/A |
| Legionella pneumophila antibodies IgM (LP-IgM) | N/A | Positive |
| Rickettsia antibody (Rick IgM) | N/A | N/A |
| Antinuclear antibodies (ANA) | <1:40 Titer | N/A |
| Antibody against double-stranded DNA (Anti-dsDNA) | <100.0IU/mL | N/A |
| Anti-RNP antibodies (Anti-RNP) | N/A | N/A |
| Anti Smith antibodies (Anti-Sm) | N/A | N/A |
| Anti-SS-A (Ro) antibodies (Anti-Ro) | N/A | N/A |
| Anti-SS-A (Anti-Ro52) | N/A | N/A |
| Anti-SS-B (La) antibodies (Anti-La) | N/A | N/A |
| Anti-Scl-70 antibody anti-Scl-70 | N/A | N/A |
| Anti-PM-Scl antibody anti-PM-Scl | N/A | N/A |
| Anti-Jo-1 antibodies (Anti-Jo-1) | N/A | N/A |
| Anti-centromere antibodies (ACA) | N/A | N/A |
| Antibody against proliferating cell nuclear antigen (PCNA) | N/A | N/A |
| Anti-nucleosome antibodies (NUCL) | N/A | N/A |
| Anti histone antibodies (AHA) | N/A | N/A |
| Antibody against ribosomal p protein (AntiriboP) | N/A | N/A |
| Anti-mitochondrial (M2) antibody (AMA-M2) | N/A | N/A |
Table 2: Respiratory and self-immune antibody determination.
| Parameter | Normal range | Date | |
|---|---|---|---|
| On admission | After admission | ||
| 2013/12/12 | 2013/12/27 | ||
| Urine α-1-microglobulin | <15.0mg/g.Cr | 177.5 | |
| Urine micro-albumin | <25.0mg/g.Cr | 2583.33 | |
| Urinary IgG | <12.0mg/g.Cr | 258.33 | |
| Transferrin in urine | <2.9mg/g.Cr | 196.04 | |
| Urinary NAG enzyme | <20IU/g.Cr | 41.67 | |
| Urinary Cr (U-Cr) | g/L | 0.48 | |
| Urine α-1-microglobulin | N/A | 85.2 | |
| Urinary IgG | N/A | 124 | |
| Urine Creatinine (original) | µmol/L | 4200.6 | |
| Urinary transferrin (U-TRF) | N/A | 94.1 | |
| Urinary NAG enzyme (U-NAG) | N/A | 20 | |
| Urine micro-albumin | N/A | 1240 | |
| 24 hours urine | 800-1800mL/24h | 2800 | 1700 |
| 24-hour urinary protein excretion | 28-141mg/24h | 3242 | 4539 |
| Urinary protein | mg/dL | 115.8 | 267 |
Table 3: Urine kidney function of the patient.
| Parameter | Normal range | Date | |
|---|---|---|---|
| 2013/12/13 | 2013/12/21 | ||
| MPO-ANCA | <180.0AAU/ml | 1472.3 | 1170.1 |
| PR3-ANCA | <180.0AAU/ml | N/A | N/A |
Table 4: ANCA-associated antibody assay.
In 1982, Davies et al. revealed anti-neutrophil cytoplasmic antibodies (ANCA) while researching antinuclear antibodies in the serum samples of patients with segmental necrotizing glomerulonephritis [5]. There were two types of ANCA included PR3- ANCA which were detected mainly in Wegener's (GPA) patients and MPO-ANCA that were principally discovered in patients with microscopic polyangiitis (MPA) or Churg-Strauss Syndrome (EGPA) [6,7]. However, the vasculitis classification criteria published by the American College of Rheumatology (ACR) in 1990 did not include MPA or ANCA and comprised any abnormal chest findings, including diffuse alveolar hemorrhage and infiltrates [8]. As a consequence, in 1994, the Chapel Hill Consensus Conference (CHCC) proposed the term “MPA” to describe small-vessel vasculitis that featured absence of deposition of immune complex and presence of pulmonary capillaritis and glomerulonephritis [9].
In clinical practice, it is occasionally difficult to make a specific distinction of ANCA vasculitis because this condition includes diseases with similar general clinical characteristics, lung and renal involvement features and a positive ANCA serology. MPA is described as a pauci-immune necrotizing small-vessel vasculitis without granuloma formation [10]. The clinical characteristics of MPA are similar to those of GPA, although ear, nose, throat and lung involvements are less common, and renal involvement may be the only manifestation [10]. The histological manifestations include those of small vessel vasculitis without involvement of medium-sized arteries and eosinophilia associated with MPO-ANCA. Granuloma formation is always absent [10]. The kidneys are involved by focal segmental necrotizing glomerulonephritis with crescent formation. Other organs affected include the muscles, gastrointestinal tract, joints, eyes and nervous system [11]. The lung involvement appears in 20-40% of MPA patients, often leading to diffuse alveolar hemorrhage (DAH) and high mortality [12]. Inversely, EGPA is characterized by asthma, hypereosinophilia and the presence of ephemeral pulmonary infiltrates. Asthma is the dominating clinical feature which is present in more than 95% EGPA patients at a greater age and become severe over time. Radiological abnormalities have been reported in 87% patients, with peripherally distributed parenchymal infiltrates, pleural and pericardial effusion, cavitating pulmonary nodules, and bronchial wall thickening as well as thickened interlobular septa [13]. The vasculitis often occur in extrapulmonary organs, mostly involving the heart, peripheral nervous system, kidneys, skin, and gastrointestinal tract [9]. The typical histopathology of EGPA is characterised by eosinophil-rich granulomatous inflammation affecting the respiratory tract and necrotizing vasculitis involving small-to-medium-sized vessels. Focal and segmental necrotizing glomerulonephritis is the most common renal disease in patients with EGPA that occurs in 20-47% cases [14,15]. The rest of the renal disease forms include eosinophilic infiltration, granuloma formation and vasculitis. Nevertheless, renal failure is a rare complication of EGPA.
In this case, our patient did not present any evidence of granulomatous inflammation or asthma, and was finally diagnosed with MPA presenting with DAH and renal insufficiency. The diagnosis of MPA is mainly by exclusion. And in the case of clinical suspicion of MPA, particularly with alveolar hemorrhage and renal dysfunction, an immediate treatment should be implemented. The routine treatment for MPA usually consists of high doses of corticosteroids (metylprednisolone 7 mg/kg/day) and immunosuppressants (cyclophosphamide 2 mg/kg/day) [11,12,16]. A medication of reduced doses of corticosteroids usually takes place in 3 to 4 months until withdrawal, and cyclophosphamide is continued for 6 to 12 months [11]. For prognosis, the symptoms can be controlled by sufficient treatment, but a recurrence might also be expected. Pulmonary fibrosis and obstructive pulmonary disease is the most common chronic complications of recurring episodes of diffuse alveolar hemorrhage [17].
This is an unusual case of microscopic polyangiitis with massive pulmonary hemorrhage and renal insufficiency. An early medication of corticosteroids helped in the rapid control of severe symptoms and allowed time for the remaining long-term treatment. Hence, it is of vital importance to act routine ANCA examination for early diagnosis of microscopic polyangiitis in patients with diffuse pulmonary hemorrhage, who otherwise have a quiet high mortality rate.
YJ and CWZ were significantly involved in medical care, and drafted of the manuscript. WCH and LYC finished the work of coordination, and participated in drafting the manuscript. All authors have read and approved the final manuscript.
The authors would like to thank the patient’s family for allowing us to use the medical documentation and information leading to the present article. This work was supported by grants from the National Natural Science Foundation of China (No. 81402324), Zhejiang Provincial Natural Science Foundation of China (No. LY14H160027).