Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
ISSN: 2167-7948
Case Report - (2013) Volume 2, Issue 3
The Radioguided Surgery (RGS) nowadays is used in many fields of oncology including thyroid tumours.
The peculiar characteristic of these procedures is the employment of isotopes that bind to the areas which need to be removed. We present a case of a residual mediastinal lesion derived from differentiated iodine negative thyroid cancer with persistent elevated thyroglobulin levels found by Scintigraphy Whole Body Scan + SPET/CT (111 In- DTPA-octreotide). RGS with radiolabeled somatostatin analogues in this case appears to be a useful method for real time tumour localization, verification of complete excision to prevent recurrence. This means that the surgery is less extent and with lower morbidity.
Integration of multiple skills in a multidisciplinary approach between surgery, nuclear medicine, endocrinology, radiology and pathologist has led to the development of a tailored procedure.
We promote further investigations of this approach to be inserted in the clinical management regarding not only neuroendocrine tumors but also thyroid cancer iodine negative with overexpression receptors for somatostatin.
<Keywords: Radioguided surgery; Differentiated thyroid cancer; Radiolabeled somatostatin analogues; Gamma probe
Exact localization of recurrent iodine negative thyroid cancer is mandatory. In patients with thyroglobulin above 10 ng/mL the diagnostic accuracy of 18F-flurodeoxyglucose positron emission tomography/computed tomography (18F-FDG PET/CT) is substantially high (72-93%). Therefore, the PET negative scan may be correlated with the presence of a residual lesion without biological aggressiveness. Thus, in the diagnostic work up the next step is represented by whole body scan (WBS) and Single Photon Emission Tomography/ Computed Tomography (SPET/CT) employing radiolabeled somatostatin analogues (111In-DTPA-octreotide: Octreoscan). RGS with a gamma probe assisted surgery is a new method of treatment in the areas of nuclear medicine, where surgery and histopathology represent an essential moment in the multidisciplinary approach. This method of surgery allows a target procedure because it permits a small area of tissue to be identified, which is further marked with a radioactive isotope, and then removed. This means that the surgery is less extent and with lower morbidity. Clearly RGS is a technically challenging method, requiring a high level of training in nuclear medicine and histopathology and a well-trained surgeon.
A 49 year old man underwent total thyroidectomy, lymphadenectomy of central compartment plus right laterocervical lymphadenectomy in February 2010 in another center. Histological examination reveals a papillary thyroid cancer with plurifocal extension in the cervical lymph node (TNM: pT3m pN1b). In April 2010, the patient underwent ablative radiometabolic therapy with 131I (5,18 GBq). In our selected case 131I Whole Body Scan performed after 72 h after Radio Iodine Therapy (RAIT), during low diet iodine (daily < 50 mcgr) kept for at least 40 days and in the absence of established pharmacological interference on iodides pool (Urinary iodine measurement in iodine insufficient area assumes prevailing epidemiological value), showed only uptake in remnant cervical post surgical tissue. No evidence of pathological uptake of Radio Iodine was demonstrated in other sites, particulary in the mediastinum (Figure 1).
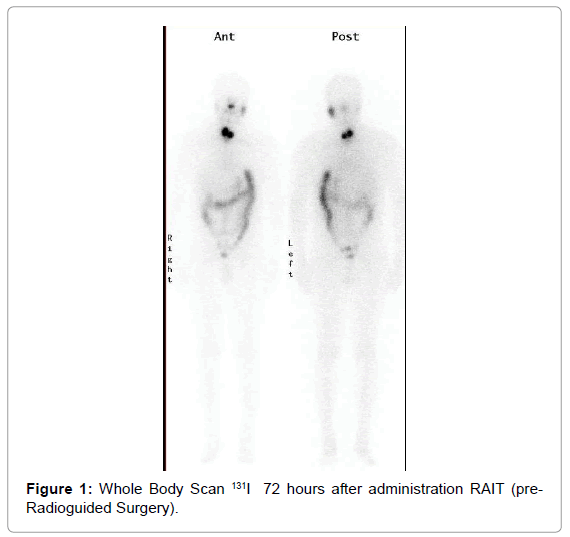
Figure 1: Whole Body Scan 131I 72 hours after administration RAIT (pre- Radioguided Surgery).
At the same time the value of thyroglobulin was 129 ng/ml and Anti bodies anti Thyroglobulin (Ab Tg): < 20 UI/ml. After radiometabolic therapy the value of thyroglobulin remain still detectable to 25.0 ng/ml and Ab Tg: < 20 UI/ml.
In June 2011, monitoring by PET / CT whole body scan 18F-FDG showed no lesion with high metabolic activity for the 18F-FDG (Figure 2).
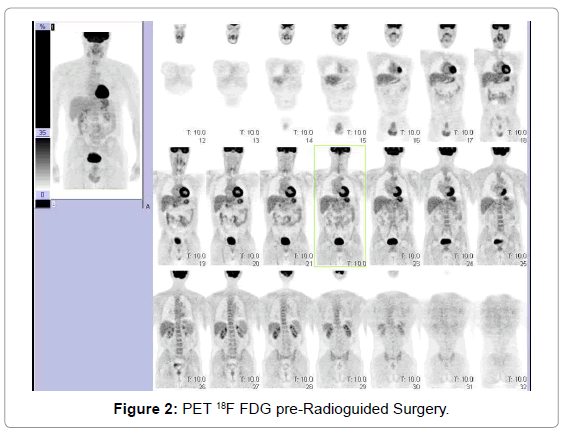
Figure 2: PET 18F FDG pre-Radioguided Surgery.
Pet protocol provides administration of 4 MBq/Kg i.v. of 18F FDG, in patient with normal serum glucose value. In order to obtain visible and evaluable images it is necessary to acquire about 2 min/bed in a 3D PET scanner. Imaging is performed after 60 minutes intravenous administration of radiotracer using hybrid scanner to have attenuation correction and better localization from the anatomical CT study.
Then we performed a Scintigraphy WBS + SPET/CT (111In-DTPAoctreotide: Octreoscan), which showed fixed radiolabeled somatostatin analogues in superior left mediastinum (Figures 3 and 4a). In the Octreoscan protocol evaluation of images is obtained at 4 and 24 hours Whole Boby Scan and SPECT/CT, after i.v injection. 111Indium DTPAoctreotide (Octreoscan: 185 MBq). Expression of radioreceptors uptake has been already showed at planar imaging. Therefore subsequent hybrid tomographic imaging SPECT/CT increases sensitivity of the study.
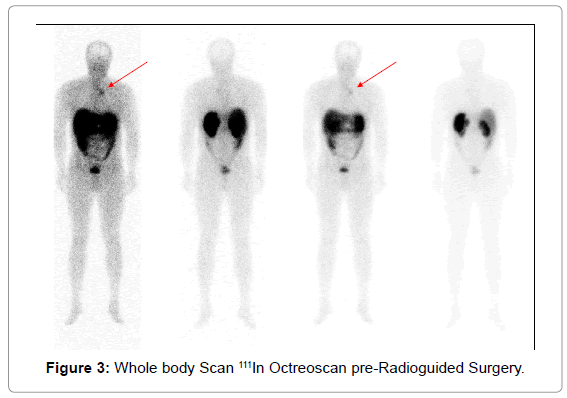
Figure 3: Whole body Scan 111In Octreoscan pre-Radioguided Surgery.
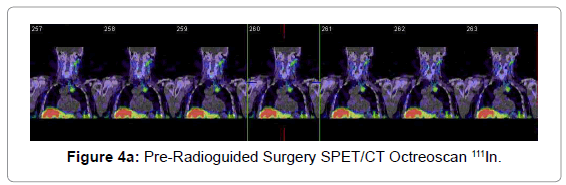
Figure 4a: Pre-Radioguided Surgery SPET/CT Octreoscan 111In.
An ultrasound examination identified that particular lesion as lymphadenopathy of 2.4 cm, placed with good approximation below the thoracic vessels. In october 2011, we performed RGS after 24 hours administration of the tracer, using an intraoperative Gamma Probe SG04 (Crystal Photonics GmbH /D-12489 Berlin, Germany - licensed in Italy by Gamma Servizi srl) (Figure 5).
A low dose (111MBq) of 111In-DTPA-octreotide was chosen to reduce absorbed doses by patient and operators. After 4 hours from injection Whole Boby Scan and SPECT/CT images were obtained. Than the patient went to the operating room. The surgical procedure allowed the removal of three areas of tissue that showed a high ratio Tumor/Background (15, 17 and 18 in vivo and >10 ex vivo - Cut off to identify pathological lesion T/B ratio > 1,3) in the retrovascular mediastinum site until the aortic arch (Figure 5). A split sternotomy was necessary to dissecate them. Six nodes out of eight retrieved in the specimen resulted positive for papillary thyroid adenocarcinoma at histological examination. Neither intra nor post-operative complication occurred. Three months after surgery Scintigraphy WBS - SPET/CT (111In-DTPA-octreotide) showed no uptake in the mediastinum (Figure 4b). Eight months later, after carrying out RGS procedure, the laboratory parameter controls provided following results: the thyroglobulin serum level decreased up to 4.5 ng/ml - Ab Tg: < 20 UI/ml (Figure 6).
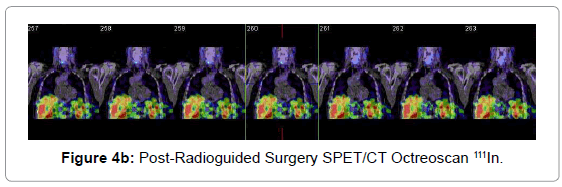
Figure 4b: Post-Radioguided Surgery SPET/CT Octreoscan 111In.
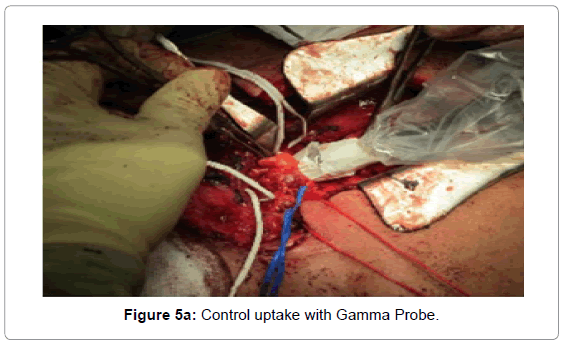
Figure 5a: Control uptake with Gamma Probe.
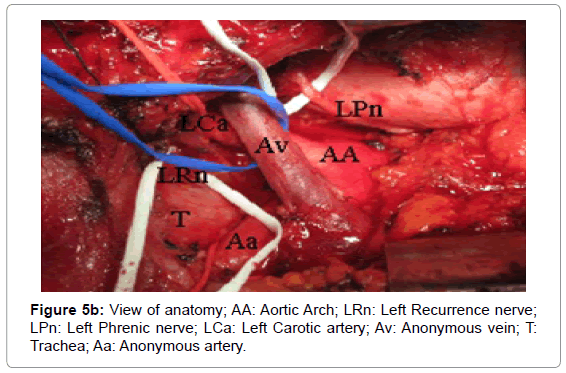
Figure 5b: View of anatomy; AA: Aortic Arch; LRn: Left Recurrence nerve; LPn: Left Phrenic nerve; LCa: Left Carotic artery; Av: Anonymous vein; T: Trachea; Aa: Anonymous artery.
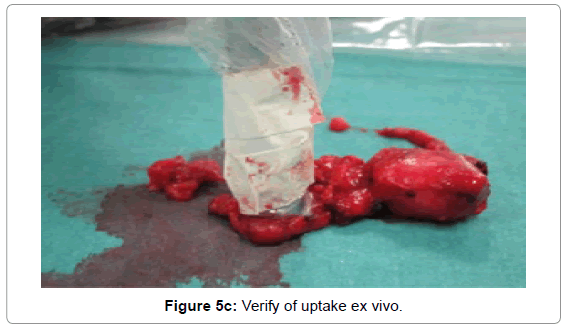
Figure 5c: Verify of uptake ex vivo.
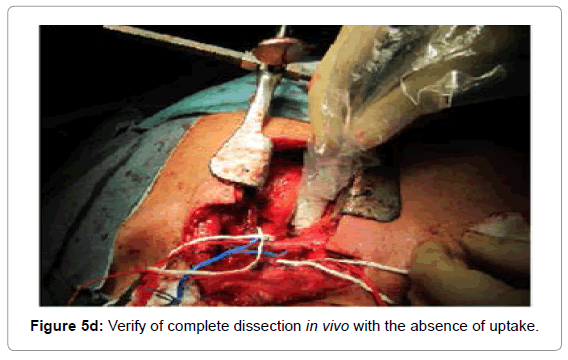
Figure 5d: Verify of complete dissection in vivo with the absence of uptake.
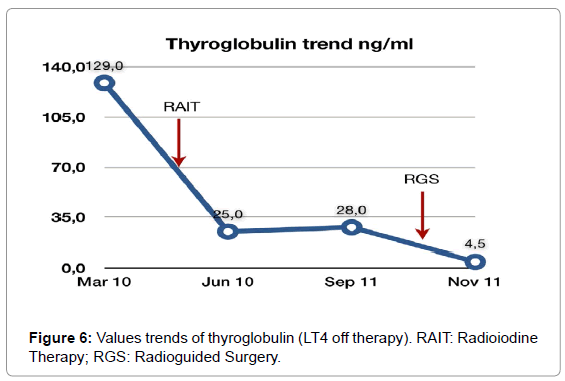
Figure 6: Values trends of thyroglobulin (LT4 off therapy). RAIT: Radioiodine Therapy; RGS: Radioguided Surgery.
Therefore, considered still detectable levels of thyroglobuin during LT4 therapy we decided to perform a PET/CT WBS 18F-FDG that was negative (Figure 7).
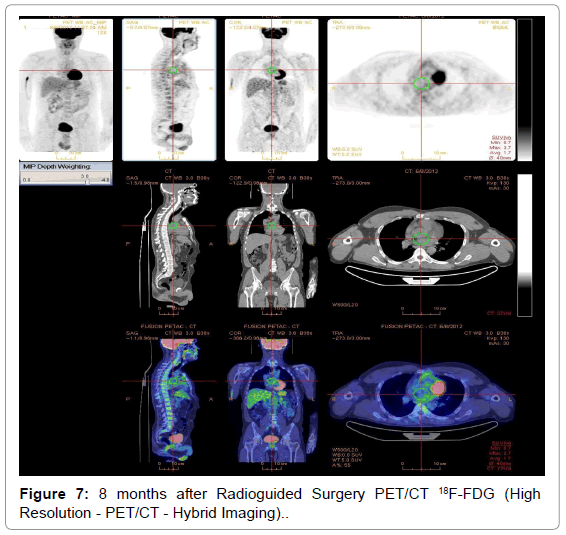
Figure 7: 8 months after Radioguided Surgery PET/CT 18F-FDG (High Resolution - PET/CT - Hybrid Imaging).
Additional controls by PET / CT WBS 18F-FDG, Scintigraphy WBS - SPET/CT (111In-DTPA-octreotide), ultrasound examination, clinical evaluation and serum level of thyroglobulin are planned at 24 months after surgery.
Radioguided Surgery (RGS) was introduced in 1985 by Martin et al. [1] RGS was utilized in the treatment of cancer of large intestine. Afterwards, this procedure was extended in the treatment of ovarian carcinoma. Today, gamma probes are widely used for localization in different kind of tumours, like ACTH-secreting bronchial carcinoid [2,3] including thyroid tumours - Differentiated Thyroid Carcinoma (DTC). Several reports showed the role of radiogioded surgery using 131I and 123I [4-6]. The general characteristic of these procedures is the employment of isotopes that bind to the areas which need to be removed. The detector transforms each gamma ray photon into an electrical signal, then the signals are transfered to read out module processed, counted and displayed. The close collaboration with the specialist in nuclear medicine allows the surgeon to localize the areas of higher activity. The management of various thyroid tumours is affected by the histological pattern, localization and spread of the tumour, and mostly by subsequent possibility of treatment with radio iodine therapy. In the recurrent lesions derived from iodine negative thyroid tumours, the proper and definitive therapy is the surgical removal of residual pathological tissue. If it is possible to remove the tumour completely, no other treatment would be necessary [7].
Dedifferentiation is associated with a worse prognosis, because the patients cannot be treated with radioiodine. In our case, in the 12 months follow up period after Radio Iodine Therapy, the persistence of detectable thyroglobuline value suggested an integrative work up with Hybrid Devices as PET/CT 18F-FDG, which was negative (Figure 1). In patients with elevated serum thyroglobulin levels with no evidence of disease on radioiodine scintigraphy after RAIT, scintigraphy with the somatostatin analog (111In-octreotide, Octreoscan; Mallinckrodt) can be an alternative imaging modality. Some authors have demonstrated uptake of 111In-octreotide in metastatic or recurrent disease in the majority of these patients [8-10]. In fact these diagnostic tool allows to identify tissue with elevated expression of radiolabeled somatostatin analogues in the anterior mediastinum back to the vessels space until the aortic arch (Figures 3 and 4a). So the patient underwent radioguided surgery using an intraoperative Gamma Probe.
In conclusion, radio guided surgery with radiolabeled somatostatin analogues appears to be a useful method for real time tumour localization, verification of complete excision to prevent recurrence.
The same advantages in RGS assisted by intra-operative PET probe in thyroid cancer are confirmed by Korean experience [11].
For this reason we promote further investigations of this approach to be inserted in the clinical management regarding not only neuroendocrine tumors but also thyroid cancer iodine negative with over expression receptors for somatostatin.