Journal of Cancer Science and Research
Open Access
ISSN: 2576-1447
ISSN: 2576-1447
Research Article - (2018) Volume 3, Issue 1
Background and objective: Carboplatin, paclitaxel, and bevacizumab (CPB) therapy is a treatment option for non-small cell lung cancer. Factors predicting the survival of patients receiving this therapy were investigated.
Methods: From 2011 to 2016, 41 patients (excluding those positive for EGFR mutation or ALK fusion gene) received first-line CPB therapy. Prognostic factors for progression-free survival (PFS) and overall survival (OS) were investigated by the Cox proportional hazards model.
Results: The median age was 70 years, 38 patients had adenocarcinoma, and 30 patients were men. Eastern Cooperative Oncology Group performance status (PS) was 0 /1 /2 in 10/ 29/2 patients. Overall PFS and OS were 6.4 and 10.9 months, respectively. According to univariate analysis, a neutrophil/lymphocyte ratio (NLR)>3.0 and hypoalbuminemia (serum albumin < 3.5 g/dL) were associated with significantly shorter median PFS and OS (NLR >3.0 vs. not: 6.3 vs. 11.2 months, p=0.00307, and 9.5 months vs. not achieved, p=0.0214; hypoalbuminemia vs. not: 5.5 vs. 9.7 months, p=0.0039, and 6.4 vs. 33.2 months, p= 0.000164). Conversely, a good PS was associated with significantly longer median PFS and OS (PS=0 vs. not: 11.1 vs. 6.1 months, p= 0.00537, and not achieved vs. 9.5 months, p=0.0343). Cox proportional analysis confirmed NLR>3.0 and hypoalbuminemia as poor prognostic factors (NLR>3.0 for PFS: hazard ratio (HR) 2.84, p=0.037; hypoalbuminemia for OS: HR 6.54, p=0.008432). However, good PS was not significant.
Conclusion: In lung cancer patients receiving CPB therapy, the prognosis might be predicted by NLR, hypoalbuminemia, and PS.
Keywords: Bevacizumab; Carboplatin; Non-small cell lung cancer; Paclitaxel; Prognostic indicator
In Japan, there are about 110,000 lung cancer patients, and 70,000 patients die of this disease each year [1,2]. Recently, epidermal growth factor receptor tyrosine kinase inhibitors (EGFR-TKI) and EML4- ALK fusion gene tyrosine kinase inhibitors have become established treatments for progressive lung cancer [3-5]. However, when these genes are negative, chemotherapy is one of the option to treat the patients with good performance status. The combination of carboplatin, paclitaxel, and bevacizumab (CPB therapy) is recommended for non-small cell and non-squamous cell lung cancer [6-9], but disease progression is frequent after recommended therapy has been completed. Although various predictors of the response of lung cancer and the prognosis have been reported [10-15] little is known about prognostic factors for chemotherapy. Therefore, we performed this study to identify prognostic factors for Japanese lung cancer patients receiving CPB therapy.
We reviewed non-small cell lung carcinoma patients receiving first-line chemotherapy with the CPB regimen (carboplatin at AUC 5, paclitaxel at 180 mg/m2, and bevacizumab at 15 mg/kg) from January 2011 to December 2016, excluding patients with tumors positive for EGFR mutation or the ALK fusion gene. Tumor response was assessed according to RECIST guidelines [16]. Progression-free survival (PFS) and overall survival (OS) were estimated by using the Kaplan-Meier method and differences between subgroups were compared by the log-rank test. We also investigated the following potential prognostic factors: Eastern Cooperative Oncology Group performance status (PS) (0 or not), neutrophil /lymphocyte ratio (NLR) (>3.0 or not), hypoalbuminemia (serum albumin <3.5 g/dL), heavy smoking (>20 pack-years), brain metastasis, and malignant pleural effusion. Cox proportional hazards analysis was employed to calculate hazard ratios for these prognostic factors. Statistical significance was accepted at P <0.05. Analyses were performed using public domain EZR software (Ver. 1.35) [17]. This study was approved by our institutional Ethics Committee. It was conducted in accordance with the Declaration of Helsinki and the Ethical Guidelines for Medical and Health Research Involving Human Subjects.
Forty-one patients were investigated and their baseline characteristics are shown in Table 1. The median age was 70 years, almost all of the patients had adenocarcinoma (n=39), and 30 patients were men. The PS was 0 in 10 patients and 1in 29 patients, with only 2 patients having a PS of 2. In addition, 23 patients had hypoalbuminemia (serum albumin <3.5g/dL), 33 patients had an NLR >3.0, 26 patients were heavy smokers, 21 patients had malignant pleural effusion, and 11 patients had brain metastasis. Twenty-seven patients had concomitant diseases, with the major complications being diabetes (n=11), cardiovascular disease (n=6), and respiratory disease (n=6).
| Age(y) | 52 – 78 (Median 70) | |
|---|---|---|
| Gender | male | 30 |
| female | 11 | |
| ECOG PS | 0 | 8 |
| 1 | 31 | |
| 2 | 2 | |
| Histology | adenomcarcinoma | 39 |
| NSCLC | 2 | |
| Clinical stage | ⅢB | 2 |
| Ⅳ | 38 | |
| Hypoalbuminemia | Yes | 23 |
| No | 18 | |
| NLR>3.0 | Yes | 33 |
| No | 8 | |
| Heavy smoke | Yes | 26 |
| (>20-pack years) | No | 15 |
| Brain Meta | Yes | 11 |
| No | 30 | |
| Malignant Pleural | Yes | 21 |
| Effusion (MPE) | No | 20 |
NLR: Neutrophil /Lymphocyte Ratio
MPE: Malignant Pleural Effusion
Table 1: Baseline characteristics.
Tumor response was assessed in 38 patients, with a partial response in 23, stable disease in 12, and progressive disease in 3. Overall PFS and OS were 6.4 months and 10.9 months, respectively (Figure 1). There were some hematologic and non-hematologic adverse events. Grade 3 or 4 adverse reactions were neutropenia in 23 patients, leukopenia in 17 patients, febrile neutropenia in 4 patients, anemia in 1 patient, thrombocytopenia in 2 patients, pneumothorax in 1 patient, and diverticulitis in 1 patient.
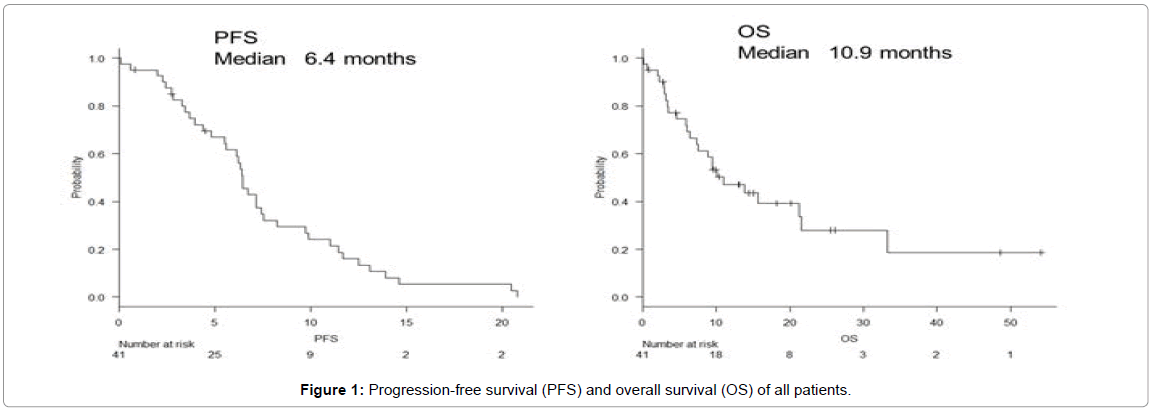
Figure 1: Progression-free survival (PFS) and overall survival (OS) of all patients.
According to univariate analysis, an NLR >3.0 and hypoalbuminemia were associated with significantly shorter median PFS (NLR >3.0 vs. not: 6.3 months [95% confidence interval (CI): 4.4-7.2] vs. 11.2 months [95%CI: 3.3-14.6], p=0.00307; hypoalbuminemia vs. not: 5.5 months [95%CI: 3.3-6.4] vs. 9.7 months 95%CI: 6.3-12.5], p=0.0039), as well as significantly shorter median OS (NLR >3.0 vs. not: 9.5 months [95%CI: 5.9-13.8] vs. not achieved (NA) [95%CI:3.5-NA], p=0.0214; hypoalbuminemia vs. not: 6.4 months [95%CI: 3.3-9.5] vs. 33.2 months [95%CI: 10.9-NA], p=0.000164) (Figure 2a and 2b). In contrast, a good PS (PS=0) was associated with significantly longer median PFS and OS (PS=0 vs. not for PFS: 11.1 months [95%CI: 2.4-13.9] vs. 6.1 months [95%CI: 3.7-6.3], p=0.00537; PS=0 vs. not for OS: NA [95%CI: 3.1-NA] vs. 9.5 months [95%CI: 4.5-21.2], p=0.0343) (Figure 2c). Heavy smoking was also associated with a shorter median PFS, but heavy smoking, brain metastasis, and malignant pleural effusion did not have a significant influence on median OS (Figures 2d-2f). The results of Cox proportional analysis are shown in Table 2. Both NLR>3.0 and hypoalbuminemia were significantly associated with a worse prognosis, with NLR >3.0 being associated with shorter PFS (hazard ratio [HR]: 2.84, p=0.037) and hypoalbuminemia being associated with shorter OS (HR: 6.54, p=0.008432). However, a good PS was not a significant prognostic factor.
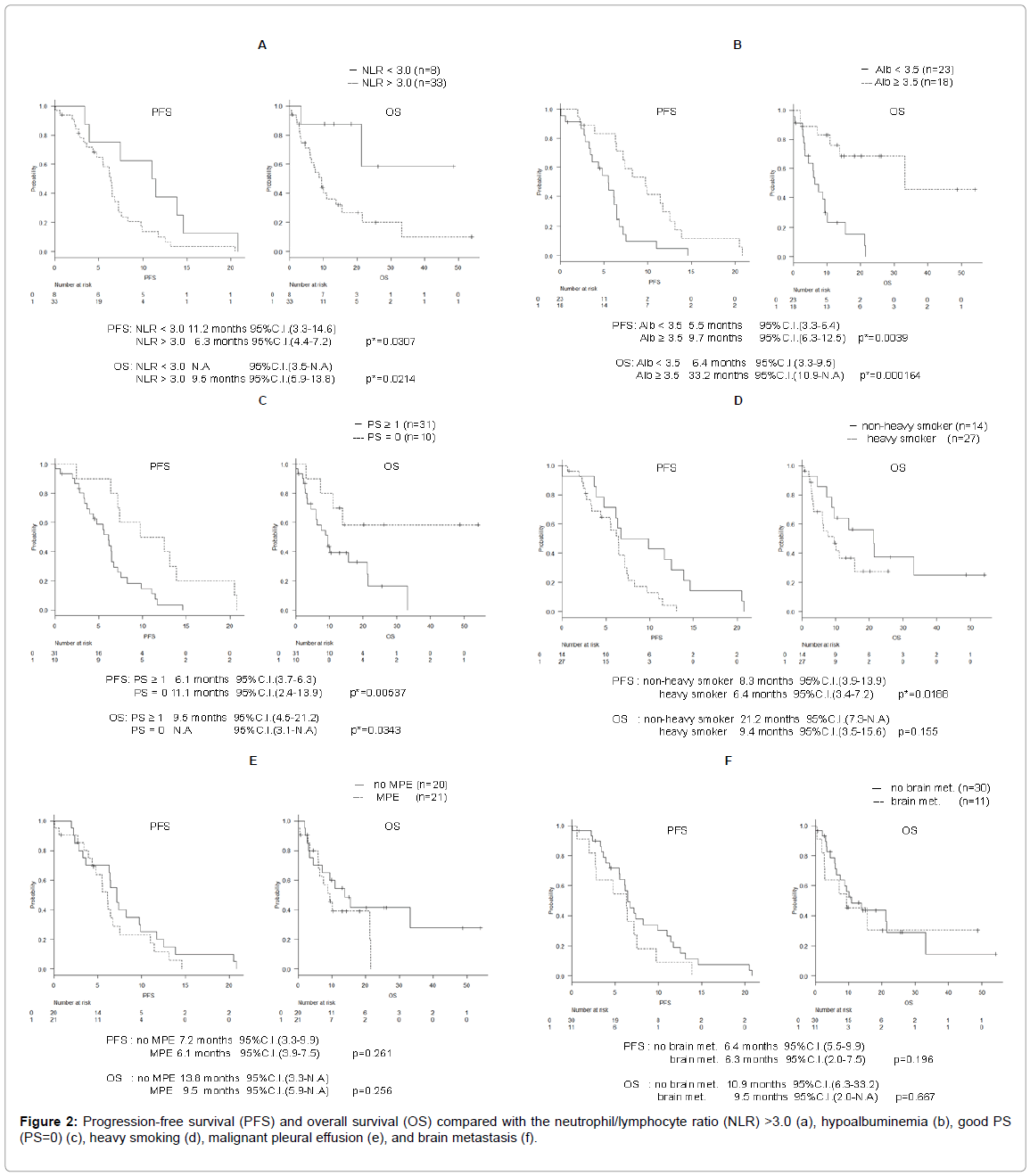
Figure 2: Progression-free survival (PFS) and overall survival (OS) compared with the neutrophil/lymphocyte ratio (NLR) >3.0 (a), hypoalbuminemia (b), good PS (PS=0) (c), heavy smoking (d), malignant pleural effusion (e), and brain metastasis (f).
| PFS | |||
|---|---|---|---|
| HR | 95% CI | P value | |
| Hypoalbuminemia | 1.881 | 0.6662-5.312 | 0.239 |
| Good PS | 0.4001 | 0.1356-1.180 | 0.09697 |
| NLR>3.0 | 2.838 | 1.0640-7.567 | 0.03711* |
| Brain metastasis | 1.416 | 0.6346-3.161 | 0.3955 |
| MPE | 0.8608 | 0.3695-2.006 | 0.7284 |
| Heavy smoking | 1.942 | 0.8240-4.577 | 0.1292 |
| OS | |||
| HR | 95% CI | P value | |
| Hypoalbuminemia | 6.535 | 1.6170-26.410 | 0.008432* |
| Good PS | 1.156 | 0.2781-4.801 | 0.8423 |
| NLR>3.0 | 3.528 | 0.7905-15.740 | 0.09856 |
| Brain metastasis | 0.9453 | 0.3684-2.426 | 0.9069 |
| MPE | 0.7585 | 0.2848-2.020 | 0.5802 |
| Heavy smoking | 1.372 | 0.5291-3.556 | 0.5157 |
NLR: Neutrophil/Lymphocyte Ratio
MPE: Malignant pleural effusion.
*P<0.05
Table 2: Results of Cox proportional analysis for PFS and OS.
In this study, factors with an influence on PFS and OS were evaluated in 41 patients who received first-line CPB therapy for nonsmall- cell lung cancer. Univariate analysis showed that median PFS and OS were shorter in patients with NLR >3.0 and patients with hypoalbuminemia, while PFS and OS were longer in patients with a PS of 0. Multivariate analysis confirmed NLR >3.0 and hypoalbuminemia as poor prognostic factors for PFS and OS, respectively. Although the doses of carboplatin and paclitaxel delivered to the patients in this study were around 15% lower than in other study (carboplatin at AUC 5 vs. 6 and paclitaxel at 180 vs. 200 mg/m2), the response to therapy and the adverse reactions were similar to those reported previously, with hematologic toxicity being somewhat reduced in this study [8]. Previous studies have suggested that poor prognostic factors for lung cancer patients include a poor PS, hypoalbuminemia, a high NLR, and malignant pleural effusion [10-15]. However, some of these studies included patients receiving surgery and others enrolled patients regardless of their treatment history. Thus, there have been few investigations focusing on lung cancer patients receiving firstline chemotherapy. In this study, all of the patients received first-line CPB therapy and the results suggested that hypoalbuminemia and a high NLR were poor prognostic factors, in agreement with previous findings. In addition, univariate analysis suggested that being a heavy smoker was associated with a worse outcome and having a good PS (PS=0) was associated with a better outcome, but multivariate analysis did not confirm these factors as independent prognostic indicators.
Hypoalbuminemia is not only an indicator of under nutrition but also an indicator of inflammation, and is incorporated into the Glasgow prognosis score to evaluate the severity of systemic inflammation [18] while NLR is also an indicator of systemic inflammation [19]. Therefore, our findings suggest that progression of lung cancer is associated with inflammation, leading to elevation of NLR and hypoalbuminemia, so these two factors are indicators of a poor outcome in patients receiving CPB therapy for non-small cell lung cancer.
Malignant pleural effusion has also been reported as a factor associated with a poor outcome [14] but we found no significant difference of PFS or OS between patients with and without malignant pleural effusion. A possible reason for this may be that bevacizumab has been reported to have a good effect on malignant pleural effusion [20] suggesting that our results could reflect the response to the bevacizumab component of CPB therapy.
This study had several limitations. First, all of the patients were treated with first-line CPB therapy, so the results are not necessarily generalizable to patients receiving other chemotherapy. However, if patients receiving multiple regimens are included in a study, there may be differences of efficacy between the regimens and differences of baseline characteristics between patients receiving each type of therapy. Accordingly, we performed analysis of a single regimen in this study to avoid such confounding factors. Second, this was a retrospective study, which limits evaluation of the applicability of the findings. Thus, further studies including prospective studies should be conducted to determine whether the prognostic factors we detected are applicable to patients receiving other chemotherapy regimens.
In conclusion, NLR >3.0 and hypoalbuminemia may be factors predicting a poor outcome in patients receiving first-line CPB therapy for non-small-cell lung cancer. These findings suggest that these factors may be useful to care the lung cancer patients receiving chemotherapy. Further investigation will be warranted.