Medical & Surgical Urology
Open Access
ISSN: 2168-9857
ISSN: 2168-9857
Case Report - (2018) Volume 7, Issue 2
Primary non- pulmonary neuroendocrine tumors are extremely rare. Prostate as a site for the tumor is sparsely reported. We report a 41-year-old patient with primary neuroendocrine tumor of the prostate. The purpose of this case report is to remind and create an awareness of the existence of this rare entity and think about it as a possible differential diagnosis when dealing with prostate neoplasms.
Keywords: Neuroendocrine Tumor; Prostate; Prostate specific antigen
Primary neuroendocrine tumors of the prostate are extremely rare. They constitute <1% of all prostatic cancers [1]. Neuroendocrine differentiation of a primary adenocarcinoma of the prostate is common, but a pure and primary neuroendocrine tumor is sparsely reported.
Although neuroendocrine tumors, like small cell carcinoma, are primarily found in the lungs, prostate is one of the sites for extra pulmonary manifestation of these tumors. Approximately 10% of extra pulmonary cases noted are found to be in the prostate [1]. It is characterized by an aggressive clinical course and a poor prognosis. Locally advanced or metastatic disease is common at the time of presentation. Tissue diagnosis is essential along with immunohistochemistry and specific tumor markers. This is essential in planning management in such patients.
A 41-year- old male presented with recurrent history of acute urinary retention, with the last acute episode occurring 1 week ago. He had no history suggestive of involvement of the lower urinary tract, hematuria, fever or burning micturition. He had no history of associated comorbidities.
A digital rectal examination revealed a significantly enlarged dysmorphic prostate, with a predominance towards the left lobe. Blood investigations, urine microscopy and urine culture were within normal limits. Serum prostate specific antigen (PSA) was 0.671 ng/mL. An ultrasound scan done demonstrated a 8.5 × 8.5 × 9.5 cm hypo echoic mass with heterogeneous internal architecture at the region of prostate with a prostate size of 362 g.
Contrast Enhanced Computed Tomography (CECT) abdomen and pelvis (Figure 1) showed a 10 × 8.5 cm well defined, solid heterogeneous enhancing mass arising from the left lobe of the prostate. A double renal pelvic system on the left side with left partial duplication was also noted. It showed no evidence of bladder or rectal wall infiltration. Cystoscopy showed an enlarged prostatic urethra with a bulky left lobe of prostate pressing medially and elevating bladder neck. The trigone was lifted up, mucosa was normal and a left double ureteric orifice stretched by the mass was noted.
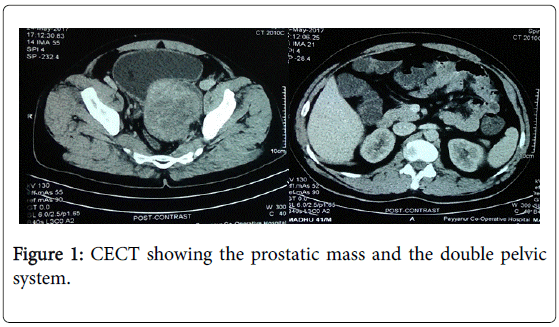
Figure 1: CECT showing the prostatic mass and the double pelvic system.
Transrectal trucut biopsy of the prostate was performed. Histopathology of the same was suggestive of poorly differentiated carcinoma of the prostate. Tumour tissue with uniform, small to medium sized, spindle shaped cells with pleomorphic nuclei was seen.
Immunohistochemistry (IHC) was done for further interpretation and confirmation of diagnosis. IHC was suggestive of Grade 1 neuroendocrine tumor of prostate (Table 1 and Figure 2).
| IHC Markers | Result |
|---|---|
| PAN CK | Positive |
| CK 7 | Scattered Positive Cells |
| CK 20 | Scattered Positive Cells |
| PSA | Negative |
| Synaptophysin | Focally Positive |
| Chromogranin | Negative |
| S-100 | Scattered Positive Cells |
| HMB 45 | Negative |
| KI | 67 5 % |
Table 1: Immunohistochemistry (IHC) Report.
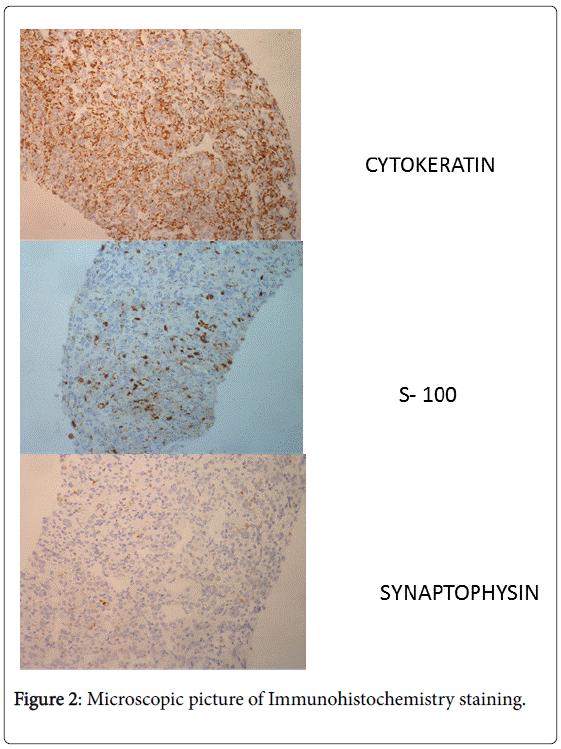
Figure 2: Microscopic picture of Immunohistochemistry staining.
A full body Gadolinium -68 PET CT scan (Figure 3) was done to rule out metastasis. A large heterogeneously enhancing lesion with areas of necrosis noted in the pelvis measuring 11.4 × 8. 8 × 14.2 cm. It showed no significant locoregional lymphadenopathy, visceral or skeletal metastasis. Patient was taken up for radical proastatectomy and pelvic lymphadenectomy.
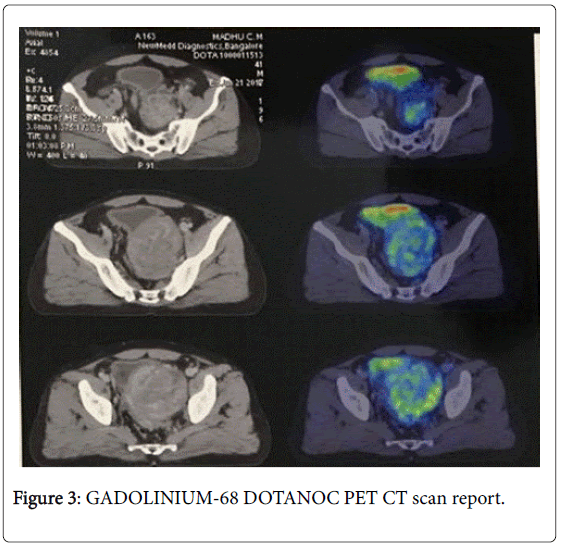
Figure 3: GADOLINIUM-68 DOTANOC PET CT scan report.
Primary and pure neuroendocrine tumors of prostate are very rare. Extrapulmonary sites of these tumors account for approximately 11% of all neuroendocrine presentations, with only 3% presenting first in the prostate [1]. These cancers represent less than 1% of all prostatic cancers [2]. Neuroendocrine tumors of prostate is an under recognized clinical condition and has an overall poor prognosis. It has an aggressive clinical course.
At diagnosis, about 75% of patients have advanced stage disease with metastasis -commonly in lung, bladder, liver, and bone [3,4]. When a prostatic cancer is detected in young men suffering from low urinary tract symptoms, the possibility of a neuroendocrine tumor should be considered.
Prostate specific antigen is not a reliable marker in diagnosing neuroendocrine tumors. The PSA levels usually remain low unless the neuroendocrine carcinoma is present along with another more common prostatic adenocarcinoma [5].
Neuroendocrine cells are frequently recognized both in normal and neoplastic prostatic tissue. The prognostic significance of this differentiation is conflicting. There is evidence suggesting that the amount of prostatic neuroendocrine elements is related to hormone resistance resulting in conversion of hormone sensitive tumor to a hormonal resistant tumor [6,7].
Chromogranin-A appears to be the best overall tissue and serum marker for neuroendocrine differentiation [8]. Other markers used are synaptophysin, neuron specific enolase (NSE) and CD56/NCAM [9].
Treatment includes surgical removal of the tumor by a radical prostatectomy with pelvic lymphadenectomy. If the diseases is metastatic, neoadjuvant chemotherapy is given.
Based on review of literature, seven cases of large cell neuroendocrine tumors of the prostate have been reported in the largest case series. Out of which 6 were in patients who had a history of adenocarcinoma treated with hormone therapy and only one was de novo [10]. Another case report was of a 48-year- old who was previously diagnosed to have adenocarcinoma with a large cell neuroendocrine tumor component. He had not been previously treated with hormonal therapy or chemotherapy, but subsequently received neoadjuvant and hormonal therapies followed by a definitive radical prostatectomy [11].
In our case, a 41-year- old presented with urinary retention. A trucut biopsy revealed malignant features with poor differentiation. Immunohistochemistry was done to confirm diagnosis. IHC was suggestive of Grade 1 neuroendocrine tumor of prostate - Grade I. A full body Gadolinium-68 DOTANOC PET CT scan was done to rule out locoregional and distant metastasis. Patient was advised radical prostatectomy with pelvic lymphadenectomy. The surgery was done at a different centre and hence details of reports were not available.
The prognostic outcomes of neuroendocrine tumor are favourable when diagnosis is made in the early stages of the disease however, there is lack of evidence to definitively conclude due to the rarity of the tumor and statistically small number of patients available for follow up.
It is important to consider the possibility of a neuroendocrine tumor whenever we come across poorly differentiated prostatic malignancy. These tumors have poor prognosis and treatment options differ from other prostate cancers [10]. Identification and documentation of these cases are necessary to come a standardized technique of evaluation and management of these tumors.