Gynecology & Obstetrics
Open Access
ISSN: 2161-0932
ISSN: 2161-0932
Research Article - (2018) Volume 8, Issue 1
Background: Globally, large disparities exist on utilization and access to the most effective contraceptive methods and women continue to have unmet need and experience unintended pregnancy. Even though Long Acting and Permanent Methods (LAMPs) are the most effective, safe and convenient methods, they are the least utilized than short acting methods in most of sub Saharan Africa. Information regarding intention to use and utilization of LAMPs and its associated factors in the study area were lacking.
Methods: Community based cross sectional study was conducted in Debre Markos town, April, 2012. A systematic random sampling technique was used to select study subjects and data was collected through face to face interview. To determine associated factors Bivariate and multiple logistic regressions were used.
Results: From 519 respondents 62.2% were currently using modern FP methods in which only 101 (19.5%) were using LAPMs. Two hundred thirty eight (45.9%) of women have intention to utilize LAPMs of contraception in the future. Being older age (35-49 years) (AOR= 3.81), having ever discussed about LAPMs with health care provider (AOR=6.20), spousal discussion about Family Planning (AOR=2.31) and having perception of their husband approves use of LAPMs (AOR=4.62), were significantly associated with utilization of LAPMs. Having Knowledge of LAPMs (AOR=4.42), currently using LAPMs (AOR=2.19), spousal discussion about Family Planning (AOR=1.78), and having perception that their spouse approves using LAPMs (AOR=2.27), were factors associated with having intention to use LAPMs in the future.
Conclusion: Majority of women knows at least one method of LAPMs, but permanent methods were the least known methods. The overall practices of LAPMs were relatively higher compared with other previous studies in the country. Therefore, it is better to address barriers to utilization and strengthening their knowledge and spousal discussion about family planning methods specifically LAPMs through mass media, health education and FP counseling.
Keywords: Intention to use; Utilization; Long acting; Permanent methods
AOR: Adjusted Odds Ratio; CI: Confidence Interval; IUDs: Intra Uterine Devices; FP: Family Planning; LAMPs: Long Acting and Permanent Methods; SSA: Sub Saharan Africa; WRA: Women of Reproductive Age.
Family Planning (FP) is a fundamental means of promoting the health of women families and communities. Modern contraception is highly effective in preventing unintended pregnancy, and is part of a strategy to reduce the high levels of maternal, infant, and child mortality [1,2]. More than half of all pregnancies are unintended, and globally, large disparities exist in access to the most effective methods of contraception [3-5].
Cultural preferences for having large family size as a norm were associated with having high fertility, maternal, infant and child mortality rates [3,6,7]. Ethiopia is among those countries having high total fertility rates (4.8), high maternal mortality ratio (676/100,000 live births) and unwanted pregnancy rate of 42% [8-11]. Unintended pregnancy with unsafe abortion and its complications was found a major reproductive health problem in Ethiopia, showing the high unmet need for FP [10,12,13].
Couples have a right to decide freely and responsibly on the number, spacing, and timing of their children and have access to the means to do so. Better availability of Family Planning services, including LAMPs might fulfill the need for healthier timing and spacing of pregnancies [13,14]. Despite progresses in family planning worldwide over the last several decades, unmet need for FP service continues to grow [13-15]. Access to FP services in general and LAPMs in particular which includes: intrauterine devices (IUDs), implants, male and female sterilization can enable women to achieve their fertility desires [1,2,16,17].
Globally LAPMs are highly popular; with female sterilization (20%) of all contraception, followed by IUD (150 million), vasectomy is the fourth most popular method (43 million women’s partner) after oral contraceptives [18,19]. LAPMs are the most effective methods available and are very safe and convenient for protection against unintended pregnancy than short term methods. According to world health organization eligibility criteria, almost all women are eligible for IUDs, implants and sterilization. LAPMs are cost effective for programs over time and with lowest discontinuation rates, but they remain relatively small and sometimes missing component of many national reproductive health and family planning programs [14,16,17,18,20].
In Ethiopia the government; on its Health Sector Development Plan IV has set its own goals to achieve a total fertility rate of 4.0 and a Contraceptive Prevalence Rate of 65% by 2015 [2]. In Ethiopia studies have shown women were more commonly using short term family planning methods, and despite the advantages utilization of LAMPs were found to be low [9,21-24].
The factors that influence contraceptive practice and intention to use were multifaceted and exist at different levels in the health care system. Examples, myths and misperceptions persisted among women, men and families. From study done in Mekele out of 63.9% of married women had heard about LAPMs in general, 80.7%, 55.3%, 39.8% and 15.6% had heard myths and misperceptions about implants, IUD, female and male sterilization respectively [9,14,20-30].
Currently, no matter how the government of Ethiopia in collaboration with different organizations is working to increase utilization of contraceptives including LAPMs, the practice of modern FP is found to be lower and it is only limited to those of short acting methods. Though previous few studies in Ethiopia have tried to determine the level of contraceptive practices, there is no study done on intention to use and practice of LAPMs and its associated factors in the study area. Therefore it might serve as an important tool for developing possible interventions to address the women or couples need of effective FP method choices and service provision.
Study area and Design
Community based quantitative descriptive cross sectional study was conducted in Debre Markos town, East Gojjam zone, North West Ethiopia, from April 08-19, 2012. The town is located 300 kilometers Northwest of Addis Ababa. The town is divided in to seven kebeles (small administrative units) having estimated total populations of 83,384 with 43,439 of them were females. Women of reproductive age group accounts 19,729 and the number of households in the town is estimated to be 19,392.
All randomly selected married women of reproductive age group who are fecund and living in the town during data collection period were included in the study. Those married women of reproductive age who are seriously ill and unable to respond were excluded from the study.
Sampling Procedure and Sample size calculation
Samples of 523 married women of reproductive age were participated in the study. The sample size was calculated by using single population proportion formula with the following assumptions: Proportion of 50%, level of significance 5% or 95% confidence interval (Zα/2 =1.96), margin of error 4.5% (d =0.045) and 10% non-response rate. Systematic random sampling was used to select the households by using their number of households as a sampling frame at each administrative unit’s. The first respondent to be interviewed from the town was determined from the town’s house number register using lottery method.
Data quality control and collection techniques
Pre tested structured Amharic version questionnaire were used to collect data from study subjects through face to face interview. The questionnaire was adapted from review of different related literatures with variables like, socio demographic characteristics, reproductive history and family planning related factors. Training was given for data collectors and supervisors on tools and overall data collection procedure. Daily supervision was done during entire period of data collection. Pretesting of the questionnaire was done on 27 married women of reproductive age and necessary corrections were made.
Data processing and analysis
The collected data were checked for completeness and entered in to EPI info version 3.5 and exported to SPSS version 20 for further analysis. Both descriptive and analytic statistics were computed and data were presented by tables, graphs, charts, percent and texts. Bivariate analysis was done primarily to identify those variables which are found to have association with the dependent variables at p value <0.2, then entered in to multiple logistic regression and variables which have association were identified on the basis of Odds ratio, with 95% CI and P value.
Ethical considerations
Ethical clearance was obtained from the ethical review board of College of medicine & health sciences, University of Gondar. Written formal letter of cooperation was also written by the town health office to all administrative units and verbal informed consent was taken from each study participants after explaining the objectives of the study.
Socio demographic characteristics of respondents
A total of 519 married women of reproductive age were included in the analysis making the response rate of 99.24%. The mean age of respondents was 29.64years with standard deviation of 7.65 years. One hundred fifty six (30.1%) of respondents were educated to secondary school and 235 (45.3%) of respondents were housewife (Table 1). Three hundred eighty five (74.2%) of them had ever given birth to one or more children. Three hundred thirty six (64.7%) of them wants to have a child and 183 (35.3%) of them don’t want to have a child in the future.
| Socio-demographic characteristics | Number (N=519) | Percent (%) |
|---|---|---|
| Age in years 15-19 | 30 | 5.8 |
| 20-24 | 120 | 23.1 |
| 25-29 | 129 | 24.9 |
| 30-34 | 85 | 16.4 |
| 35-39 | 84 | 16.2 |
| 40-44 | 52 | 10 |
| 45-49 | 19 | 3.7 |
| Ethnicity | ||
| Amhara | 484 | 93.3 |
| Oromo | 12 | 2.3 |
| Tigre | 10 | 1.9 |
| Agawu | 10 | 1.9 |
| Others* | 3 | 0.6 |
| Religion | ||
| Orthodox | 422 | 81.3 |
| Muslim | 67 | 12.9 |
| Protestant | 20 | 3.9 |
| Catholic | 10 | 1.9 |
| Respondents educational status | ||
| can’t read & write | 101 | 19.5 |
| Read and write only | 71 | 13.7 |
| Primary school(1-8) | 95 | 18.3 |
| Secondary( 9-12) | 156 | 30.1 |
| 12+1 and above | 96 | 18.5 |
| Husbands education status | ||
| can’t read & write | 36 | 6.9 |
| Read and write only | 74 | 14.3 |
| Primary school(1-8) | 83 | 16 |
| Secondary( 9-12) | 132 | 25.4 |
| 12+1 and above | 194 | 37.4 |
| Respondents occupational status | ||
| House wife | 235 | 45.3 |
| Merchant | 101 | 19.5 |
| Farmer | 12 | 2.3 |
| Daily laborer | 50 | 9.6 |
| Government employee | 100 | 19.3 |
| Student | 21 | 4 |
| Husband’s occupation | 139 | 26.8 |
| Merchant | 45 | 8.7 |
| Farmer | 95 | 18.3 |
| Daily laborer | 219 | 42.2 |
| Government employee | 21 | 4 |
| Private work |
*Gurage, wolayita
Table 1: Socio-demographic data of married women of reproductive age (15-49 years) in Debre Markos town, East Gojjam zone, North West Ethiopia, April 2012.
Concerning their Knowledge or awareness; about 502 (96.7%) of the respondents knows at least one methods of modern FP and 423 (81.5%) of respondents knows at least one methods of LAPMs of contraception and 96 (18.5%) didn’t know the methods. Among the methods Injectable was mentioned by 501 (96.5%) respondents followed by daily pills 417 (80.3%), Jadelle 384 (74%), Implanon 367 (70.7%), IUD 294 (56.6%), female sterilization 133 (25.6%) and vasectomy with only 56 (10.8%) was the least known method. Health workers 331 (63.8%), television 319 (61.5%), radio 169 (32.56%), health extension workers 167 (32.18%), friends/relatives 95 (18.3%), family members 70 (13.49%) were the commonly mentioned source of information.
Almost half 273 (52.6%) of respondents had ever discussed about LAPMs at least once with their health care providers and commonly discussed methods were Implants 175 (33.7%), IUD 120 (23.1%), female sterilization 63 (12.1%) and vasectomy 16(3.1%).
Contraceptive Utilization among married women of reproductive age
From a total of 519 respondents, 406 (78.2%) had ever used modern contraceptive methods ranging from 4 to 180 months and with the median duration of 36 months. Three hundred twenty three (62.2%) respondents were currently using modern family planning methods of which 235 (45.2%) were using current method to postpone pregnancy or for spacing and 88 (17.0%) were using for limiting. One hundred one (19.5%) were using LAPMs (11.0% for spacing & 8.5% for limiting) [95% CI: 16.4-22.7]. Injectable 196 (37.8%) were commonly used followed by implants 82 (15.8%), daily pills 24 (4.6%), IUD 17 (3.3%), 2 (0.4%) for both female sterilization and vasectomy and 2 (0.38%) were using condom.
Intention to use LAPMs, and reasons for not currently using LAPMs
From a total of 519 respondents, 238 (45.9%) [95% CI: 41.4- 50.3%] of women had intention to use one of the LAPMs of contraception in the future, 194 (37.4%) don’t want to use and 87 (16.8%) of them haven’t decided. Ninety eight (18.9%) of them want to use implanon in the future, followed by Jadele 67 (12.9%), IUD 60 (11.6%) and female sterilization 13 (2.5%). They intended to use LAPMs mainly for spacing longer interval between pregnancies 133 (55.9%) and don’t want any more child (limiting) 67 (28.2%).
Regarding spousal discussion 235 (45.3%) of respondents had discussed about FP with their husband in the last 6 months of interview. Almost half 281 (54.1%) of study subjects perceive their husband approves using LAPMs and 130 (25.0%) of them responded I didn’t know. In only 390 (75.1%) of respondents their husband knows whether they are using or not using contraceptive methods and 336 (64.7%) of them had discussed with their spouse about which method to use. Majority 366 (70.5%) of respondents believe joint decision about to use LAPMs with their partner.
Out of 418 respondents who are not currently using LAPMs, the main reasons mentioned for not using LAPMs were fear of side effects 175 (41.9%), followed by 162 (38.8%) prefers short term and 135 (32.3%) health concerns. Fear of side effects from LAPMs 164 (58.4%), respondents opposition 116 (41.3%), health concerns from using LAPMs 104 (37.0%) and preferring short term methods 102 (36.3%) were the main reasons mentioned for not intending to use LAPMs in the future (Figure 1).
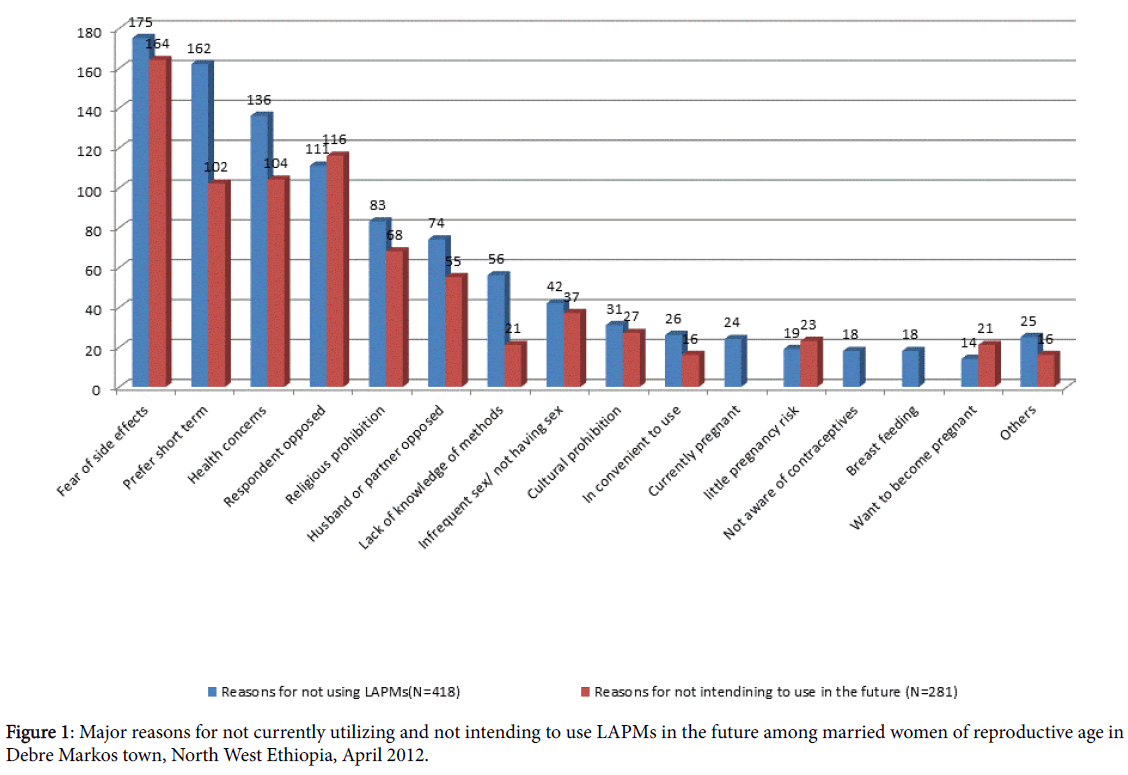
Figure 1: Major reasons for not currently utilizing and not intending to use LAPMs in the future among married women of reproductive age in Debre Markos town, North West Ethiopia, April 2012.
Almost half 246 (47.4%) of respondents had heard myths/beliefs and misconceptions about at least one methods of LAPMs.
Factors associated with utilization of LAMPs
Respondents’ age, occupation, ever had discussion with health care professionals, spousal discussion in the past 6 month about FP and perception of spousal approval of LAPMs were finally found to be significantly associated with utilization of LAPMs on multiple logistic regression model.
In this study those women whose age was 35-49 years were almost four times more likely to use LAPMs than those of age 15-24 [AOR= 3.81, CI: 1.84, 7.91]. Those women who were merchant and daily laborer were 2.39 and 3.75 times more likely to currently use LAPMs than those who were house wife [AOR=2.39, CI: 1.23, 4.66] and [AOR=3.75, CI: 1.57, 8.93] respectively.
Those women who had ever discussed about LAPMs with health care provider were more than six times more likely to currently use LAPMs than those who didn’t [AOR=6.20, CI: 3.20, 12.22]. Also those women who had spousal discussion about FP in the last 6 months were 2.31 times more likely to use LAPMs than those who didn’t [AOR=2.31, CI: 1.03, 5.15] and those women who perceives that their husband approves use of LAPMs were 4.62 times more likely to use LAPMs than those who didn’t know their husbands attitude [AOR=4.62, CI: 1.45, 14.70] (Table 2).
| Independent variable | Practice of LAPMs | Crude OR (95%CI) | Adjusted OR (95% CI) | |
|---|---|---|---|---|
| Yes | No | |||
| Age in years | ||||
| 15-24 | 20 | 130 | 1 | 1 |
| 25-34 | 40 | 174 | 2.338(0.834, 2.676) | 1.735(0.882, 3.412) |
| 35-49 | 41 | 114 | 0.154(1.295, 4.22) | 3.816(1.84, 7.917)* |
| Religion | ||||
| Orthodox | 74 | 348 | 1 | 1 |
| Muslim | 12 | 55 | 1.026(0.52, 2.01) | 0.791(0.368, 1.701) |
| Protestant | 11 | 9 | 5.748(2.30, 14.36) | 4.408(1.553, 12.50)* |
| Catholic | 4 | 6 | 3.135(0.86, 11.38) | 0.87(0.184, 4.191) |
| Respondents occupation | ||||
| House wife | 32 | 203 | 1 | 1 |
| Merchant | 23 | 78 | 1.87(1.03, 3.395) | 2.395(1.23, 4.66)* |
| Farmer | 1 | 11 | 0.577(0.072, 4.62) | 0.971(0.11, 8.597) |
| Daily laborer | 11 | 39 | 1.789(0.83, 3.849) | 3.751(1.575, 8.93)* |
| Govern’t employee | 29 | 71 | 2.59(1.465, 4.584) | 1.30(0.595, 2.842) |
| Student | 5 | 16 | 1.982(0.679, 5.78) | 1.637(0.434, 6.179) |
| Discussion with health care provider about LAPMs | ||||
| Yes | ||||
| No | 90 | 183 | 10.50(5.45, 20.23) | 6.20(3.20, 12.224)* |
| 11 | 235 | 1 | 1 | |
| Discussion with partner about FP in the last 6month | ||||
| yes | ||||
| No | 65 | 170 | 2.63(1.67, 4.13) | 2.31(1.036, 5.158)* |
| 36 | 248 | 1 | 1 | |
| Perception of Spousal approval of LAPMs | ||||
| Approve | 90 | 191 | 14.84(5.31, 41.43) | 4.62(1.45, 14.70)* |
| Didn’t approve | 7 | 101 | 2.18(0.62, 7.66) | 2.96(0.787, 11.17) |
| I don’t know | 4 | 126 | 1 | 1 |
Backward LR stepwise logistic regression
Table 2: Factors associated with utilization of Long Acting and Permanent contraceptive Methods among married women of reproductive age in Debre Markos town, North West Ethiopia, April 2012.
Factors associated with Intention to use LAMPs
On bivariate analysis women’s, age, educational status, occupations, knowledge of LAPMs, knowledge of place where LAPMs can be found, knowledge of advantages of LAPMs, discussion with health care providers about LAPMs, ever use of modern FP methods, currently using modern FP, approving others using LAPMs, duration of FP use, currently using LAPMs, source of information, decision about using FP, perception of partner approval, discussion with partner, husbands knowledge about contraception status and heard myths or misconceptions were significantly associated with intention to use LAPMs at p-value of less than 0.2.
This study revealed that those women in the age group of 15-24years were 2.24 times more likely to intend use of LAPMs than 35-49years [AOR=2.24, CI: 1.17, 4.28]. Those women who have knowledge of those LAPMs and currently using LAPMs were 4.4 times and 2.9 times more likely to have intention than those who didn’t [AOR=4.42, CI: 1.93, 10.15] respectively.
This study also indicated that discussion with partner about FP in the last 6 months were almost twice more likely to have intention than who didn’t [AOR=1.78, CI: 1.10, 2.86]. On the other hand those women who perceive that their spouse approves using LAPMs were 2.27 times more likely to have intention to use LAPMs than those who didn’t know [AOR=2.27, CI: 1.29, 4.01] (Table 3).
| Independent variable | Intention to use LAPMs | Crude OR (95%CI) | Adjusted OR (95% CI) | P- Value | |
|---|---|---|---|---|---|
| Yes | No | ||||
| Age in years | |||||
| 15-24 | 79 | 71 | 1.62(1.03,2.55) | 2.24(1.17,4.28) | 0.014 |
| 25-34 | 96 | 118 | 1.18(0.78,1.80) | 1.01(0.57,1.79) | 0.94 |
| 35-49 | 63 | 92 | 1 | 1 | 0.014 |
| Knowledge of LAPMs | |||||
| Yes | 229 | 194 | 11.41(5.5,23.2) | 4.42(1.93,10.15) | |
| No | 9 | 87 | 1 | 1 | 0 |
| Currently using LAPMs | |||||
| Yes | 79 | 22 | 5.84(3.5,9.76) | 2.19(1.18,4.07) | |
| No | 159 | 259 | 1 | 1 | 0.012 |
| Discussion with partner about FP in the last 6month | |||||
| Yes | 148 | 87 | 3.66(2.54,5.27) | 1.78(1.10,2.86) | |
| No | 90 | 194 | 1 | 1 | 0.017 |
| Women’s approval of couples using LAPMs | |||||
| Yes | 236 | 135 | 127.6(31.1,523.3) | 65.74(15.7,274.4) | |
| No | 2 | 146 | 1 | 1 | 0 |
| Perception of Spousal approval of using LAPMs | |||||
| Approve | 137 | 54 | 4.22(2.69,6.62) | 2.27(1.29,4.01) | 0.004 |
| Didn’t approve | 41 | 127 | 0.53(0.33,0.86) | 0.83(0.45,1.52) | 0.55 |
| I don’t know | 60 | 100 | 1 | 1 | 0.002 |
Table 3: Factors associated with intention to use LAPMs among married women of reproductive age in Debre Markos town, North West Ethiopia, April 2012.
Knowledge about FP is an important step toward gaining access to and using a suitable contraceptive method in a timely and effective manner. The knowledge of modern FP was high in the study area with 502 (96.7%) of respondents at least knows one modern method and 423 (81.5%) of respondents knows at least one LAPMs. This is higher than study done in Mekelle (63.9%); Goba (66.9%) and Batu (58.3%) towns each knows at least one LAPM. The commonly known LAPMs were; 74% Jadele followed by 70.7% Implanon, 56.6% IUD, 25.6% female sterilization and 10.8% vasectomy. This is also higher than study done in Mekelle, Batu (except for implant), India and Ghana except for female sterilization and vasectomy in which it was higher in India & Ghana. This can be explained by the difference in time, study setting and acceptance of non-hormonal or permanent methods in those areas [23,24,31-33].
In this study overall 101 (19.5%) were currently using LAPMs [95% CI: 16.4-22.7] (11.0% for spacing and 8.5% for limiting) in which majority of them were using implants (15.8%), followed by IUD (3.3%), only one were using FS and vasectomy each. This is higher than study done in Goba town where 8.72% were using LAPMS (6.5% were using implant, 1.5% IUD and 0.7% were using tubal ligation) and Mekelle town where 12.3% were using LAPMs (10.6% using implant, 1.5% IUD and none were using male or female sterilization). It is also higher than that of EDHS 2011 (implants 3.4%, IUD 0.3%, FS 0.5%), study in Hetosa district (none) and north Gondar zone (1.1% IUD, 0.4% implant) [9,21,23,24,34]. In this study IUD users were almost comparable with study in Nigeria (4.5%), but lower than study in India 10.3%. In this study female sterilization were almost comparable with EDHS 2011 (0.5%) and Goba town (0.7%); and lower than study in Nigeria (4.5%) [9,28,31]. The possible reasons for this is may be due to geographical and time variations in which the current study is localized to town with more knowledge, information and access to different methods, and the difference for female sterilization is mainly attributed to geographical difference in which they have more knowledge & it has acceptance in those areas than the current.
The main reasons mentioned for not currently using LAPMs were fear of side effects 41.9%, prefers short term 38.8%, health concerns 32.3%, respondents opposed 26.6% and religious prohibition 19.9%. This is in line with study done in Congo, Ghana and Uganda that the main reasons for non-use of contraceptives were; risk of health consequence, religious convictions, lack of knowledge of methods, rumors about side effects, personal dislike, and having no or infrequent sex [35-37]. From study in Hosanna town the main reasons for not using contraceptives includes desire to have more children (32%), husband opposition (23.2%), and fear of side effects (15%) (38). From study in Mekelle town main reasons for not using LAPMs were using another method (93.3%) and developing side effect (3.9%) [24].
Myths and misconceptions were predominant in the study area in which 47.4% had heard at least towards one or more LAPMs. This is higher than study done in Batu town in which 33.2% of women had heard myths and misconception towards LAPMs [32]. This is due to the difference in the study subjects in which study in Batu were among FP service users.
In this study those women whose age was 35-49 years were almost four times more likely to currently use LAPMs than those of age 15-24 years. In agreement with this study done in south Wollo zone showed that 81% of the clients who had used long term and permanent methods were in the age group of 25-44 years [22]. The might be due to those women who are older were having more number of children and have more intention to limit childbearing than those who are younger, which is also supported by study in Oromia region [30].
In current study those women who had discussed about LAPMs with health care provider were more than six times more likely to currently use LAPMs than those who didn’t. Also those women who have knowledge of those LAPMs and currently using LAPMs were 4.4 times and 2.9 times more likely to have intention than those who didn’t respectively. Which is in line with study done in Dawro zone; having better knowledge about modern contraceptive methods, gender equitable attitude and better involvement in decisions were factors for better decision making power of women to use modern contraceptive methods in urban setting [25]. The possible reasons for this is may be due to those who had discussed with health care providers have more knowledge about available FP methods and advantages or benefits and effectiveness of LAPMs than those who didn’t.
Those women who had spousal discussion about FP in the last 6 months were 2.31 times more likely to use LAPMs than those who didn’t and those women who perceive that their husband approves use of LAPMs were 4.62 times more likely to use LAPMs than those who didn’t know their husbands attitude. This study also showed that discussion with partner about FP in the last 6 months were almost twice more likely to have intention than who didn’t. On the other hand those women who perceive that their spouse approves using LAPMs were 2.27 times more likely to have intention to use LAPMs than those who didn’t know.
This result is in line with study in Jimma by Haile showed that couples who openly discuss about FP and wives who perceive that their husbands approve of FP, were more likely to be current contraception users than their counterparts (OR, 2.5 & 6.8 respectively). Another study done in Jimma indicated that contraceptive practice was strongly associated with spousal discussion about FP [38-40]. From study in Pakistan barriers to a woman’s intention to use contraceptive methods was her belief that family planning decisions were made by the husband [29]. The possible reasons could be due to those women who discusses about FP were more likely to discuss about their desired family size, timing and methods of contraception to be used than those who didn’t.
Limitations of this study were; on calculating the sample size we considered to use proportion of 50% which yields a maximum sample size since the utilization of LAPMs from the existing literatures at the moment were very low and the study is only localized to town which limits generalizability for a larger population.
In conclusion, majority of women knows at least one method of LAPMs, but permanent methods were the least known methods. The overall practice of modern family planning and LAPMs were relatively higher compared with other studies in the country. Significant number of women had intention to use LAPMs in the future and had heard myths and misconceptions towards LAPMs. Fears of side effects, preferring short term methods, health concerns, respondents’ opposition, religious prohibition, husband or partner opposition and lack of knowledge of methods were the main barriers for not currently using and intending to use LAPMS in the future. In this study being older age, respondent’s occupation, having discussed about LAPMs with health care providers, spousal discussion and perception of spousal approval of LAPMs were significantly associated with utilization of LAPMs. Having Knowledge of LAPMs, currently using LAPMs, spousal discussion about Family Planning and having perception that their spouse approves using LAPMs were factors associated with having intention to use LAPMs in the future.
Therefore, health education/information’s better provided through mass Medias and health care providers regarding all methods, their advantages, expected side effects and efforts should be made to address clients’ concerns and fears about methods. Strengthening women’s knowledge on LAPMs and encouraging spousal discussion’s about family planning methods specifically LAPMs through community conversation and during family planning counseling. Further studies on wider areas including rural populations and institutional and service provider related factors that affect the utilization of LAPMs were recommended.
The authors declare that they have no competing interests.
GAB has designed the study, supervised data collection, entered and analyzed data and drafted the manuscript DBD have revised the proposal, supervised data collection, and participated on the analysis and subsequent revisions of the manuscript.
Author’s read and approved the final manuscript.
We would like to express my gratitude to University of Gondar for funding this research. We would also like to acknowledge Debre Markos city administration; all study respondents who participated in the study, supervisors and data collectors.