Journal of Pharmaceutical Care & Health Systems
Open Access
ISSN: 2376-0419
ISSN: 2376-0419
Review Article - (2019) Volume 6, Issue 1
Objective: Medication adherence and the assessment of patients’ adherence are known to be problematic. There is often a discrepancy between the adherence rate estimated by the physician and the actual adherence rate of the patient. This literature review gives an overview about the published studies investigating physicians’ assessment of patient adherence in comparison to the actual medication adherence.
Methods: This review was conducted in compliance with the Grade system in March 2016 and September 2018. Articles included in this review were identified by literature search in Medline and the Cochrane Library. Search terms included patient compliance, physicians, physician-patient relations and assessment. We included every type of study, in German or in English language.
Results: Out of 588 results, 41 were included in the review. Due to the language, non-availability of the article or inconsistency with the investigated topic, only 19 studies were evaluated. In most of the studies an overestimation of patients’ adherence by physicians got obvious.
Conclusion: Physicians assessed medication adherence of their patients mostly incorrect. They tend to overestimate the medication adherence of patients. Only in mental disorders they tend to underrate. A visual analog scale seems to be a good method to assess physicians’ estimation of patients’ adherence. Patients’ adherence should be measured by directs methods or MEMSTM.
Practice implications: For evaluating the non-adherence in patients the physicians have to discuss the medication regimen with the patient and have to ensure the adherence of the patients.
Keywords: Systematic review; Patient compliance; Physician-patient relations; Assessment
Medication adherence is a prerogative for the efficacy and safety of drug therapy. Low medication adherence rates of patients may lead to an increased number of consultations of medical practitioners and an increased rate and duration of hospital stays and hence higher costs for the health care system [1]. Non-adherence rates up to 50% are reported for patients with chronic diseases and medication persistence lasted only for 6 months [1-3]. WHO identified five major factors impacting medication adherence which health system, social/economic, therapyrelated, patient-related, and condition-related factors. Deficient information and teaching about medication intake by the doctors or high therapy costs are associated with health system factors on nonadherence [3]. A wrong estimation by the physician may result in more prescribed or in more expensive medication to adjust the patient to its therapy.
Medication adherence can be measured by different methods which are categorized as direct (e.g. drug concentration measurement in blood or urine) or indirect methods (e.g. self-reports, pharmacy refill, pill count or electronic monitoring). Direct methods are more valid, since medication intake is proven. But these methods are expensive due to a higher level of effort [4]. Indirect methods only assume the intake [1]. Self-reports (e.g. Morisky questionnaire) and pill count may overestimate the medication adherence.
Nowadays MEMSTM is regarded as the gold standard for the indirect measurement of medication adherence [4]. MEMSTM means Medication Event Monitoring System and is a pill container with a cap containing a microelectronic chip to register the time and date of every opening of the container automatically. The evaluation then takes place with the help of software and provides an adherence pattern.
For physicians’ assessment of medication adherence of the patients, no questionnaire exists. In the literature, there are several articles with different assessment tools, like rating scales. Usual physicians have to identify the medication adherence of their patients during a short conversation. Several studies have compiled the physicians’ estimation of the medication adherence of their patients. So far, a systematic review of studies regarding physicians’ assessment of patients’ adherence and type and effectiveness of the assessment tools is not available. Furthermore the review should determine if a correlation between physicians’ assessment and the type of disease of the patients exists.
Outcome of the review
Primary outcome: The primary outcome evaluated the differences between the adherence assessment by physicians and the adherence rates reported by patients.
Secondary outcome: This systematic review compiled the best practice method to estimate patients’ adherence by physicians and the most common method to detect patient adherence. Furthermore, the review determined, if there is a correlation between a disease and the assessed adherence by physicians.
Criteria for considering studies for this review
Types of studies: We included every type of published study, in German or in English language, that evaluate a correlation between the adherence assessments by physicians and patient’s self-assessments or any other medication adherence measuring method. Studies were excluded due to the following reasons:
a) Studies did not focus on medication adherence
b) Studies did not supply quantifiable adherence data
c) Double citations
No publication was excluded due to a low quality.
Type of participants: Studies including outpatients and inpatients who were prescribed medications for a medical disorder were considered for this review.
Types of outcome measures: Publications in which medication adherence was reported as primary or secondary outcome with any kind of assessment of the adherence.
Adherence definitions: Under “adherence” different definitions were used:
a) Dosing Adherence was defined as the percentage of Treatment days with the correct number of doses taken.
b) Taking adherence was defined as the percentage of prescribed doses taken.
c) Timing adherence was defined as the percentage of doses taken within pre-defined time window.
d) Percentage of adherent patients was based on the percentage of patients with adherence measures greater than a pre-defined value.
Out of these results a patients may also defined as adherent than a patient took 80% or more of his medication at the right dose and/or at the right time. However, if the patient only adheres to 80% to 20% of the recommended therapy regimen, he was partially adherent. Nonadherent was less than 20%.
Search methods for identification of studies
We searched the following electronic databases for evaluable papers:
a) MEDLINE
b) The Cochrane Library
All databases were searched from their start date until March 2016. In September 2018 the document and the list of sources were updated by PubMed recherche.
The search strategies were developed for MEDLINE and adapted for the other database. The 3 search strategies for MEDLINE and Cochrane Library were Patient compliance (Mesh) AND Physicians (Mesh) AND Assessment, Physician-Patient Relations (Mesh) AND Patient Compliance (Mesh) AND Physicians (Mesh) and Medication compliance (tiab) OR Medication adherence (tiab) AND Physicianpatient relations (Mesh). We also contacted authors of included but missing full text papers in electronic databases and asked them to provide these papers.
Data collection and analysis
Selection of studies: Two persons searched independently and blinded to the results of each other for eligible publications. The titles and abstracts were screened for eligibility. If a publication was assessed as potentially eligible by one of the reviewers, it was included for fulltext review. After full-text review ineligible papers were excluded and the final selection was achieved. Disagreements between the two reviewers were resolved by discussion.
Data extraction and management: For each eligible publication one author extracted all essential data. Extracted data were compiled in two tables. Table 2 provides following data:
a) Authors
b) Disease
c) Patient: adherence assessment methods
d) Physician: adherence assessment methods
e) Number of participating patients
f) Number of participating medical practitioners
g) Outcomes according to the patients
h) Outcomes according to the physicians
i) Estimation of Adherence/Tendencies
A summary of included studies contained following information in Table 3:
(1) Author name, title
(2) Participants
(3) Study design
(4) Measures of adherence (in detail)
(5) Outcomes
(6) Notes
The extraction was reviewed and confirmed by the other reviewer. If information was not provided, it was marked as “unknown” in the table.
Assessment of the risk of bias: The quality of each publication was assessed independently and blinded by each reviewer using the Cochrane Collaboration’s “Risk of bias” assessment tool [5]. The studies were assessed based on their risk of:
a) Performance bias
b) Information bias
c) Selection bias
d) Detection bias
The papers were given a score -1 (high risk of bias), 0 (unclear risk of bias) or +1 (low risk of bias) for every possible type of bias. A total score was calculated ranging from -4 to +4. Papers with a score from -4 to 0 were defined as papers of low quality, papers with a score from 1 to 2 as papers of moderate quality and papers with a score from 3 to 4 as papers of high quality. Disagreements were resolved by discussion.
The studies were evaluated on the basis of four different classifications. Performance bias means the location of the study (outpatient, inpatient, multicenter, rural or urban), as well as the duration of the study (e.g. for MEMS it should be at least six months), the specialization of the disease (specific or transmissible to other diseases) and whether the identical form of the method was used by the physicians and the patients.
In the information bias, the physician-patient relationship, i.e. whether the patient and physician have known each other for some time was assessed.
In the selection, the study population is examined more closely. The number of participants in the study, the inhomogeneity of the participant group (e.g. different ages) and the drop outs are evaluated.
In the last point, under detection bias, the definition of adherence the intention-to-treat and the doctor-blinding are evaluated with regard to the patient’s self-assessment.
Statistical analysis: All data were extracted from the retrieved articles, since the data was given in a heterogeneity form. Some given data the mean was calculated. No further statistics methods were used for this review.
General findings
In March 2016, after removal of duplicates, 505 citations were identified. Screening of the abstracts resulted in 33 publications which met the inclusion criteria. Out of these 17 studies were evaluated. At the second search, in September 2018, 83 additional publications were identified. After reading the abstracts 8 papers were reviewed and two publications met the inclusion criteria as seen in Figure 1 Details of paper evaluation [6-24].
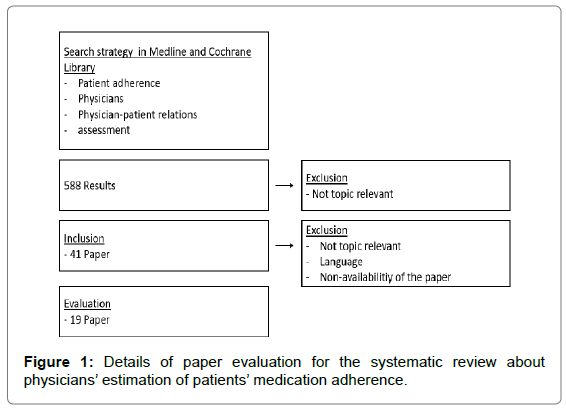
Figure 1: Details of paper evaluation for the systematic review about physicians’ estimation of patients’ medication adherence.
Study characteristics
On average 280 patients (40-1587 patients) and 123 physicians (3- 412 physicians) participated in the studies (Table 2). In eight papers the number of participating physicians was not mentioned. In one paper the response rate of participating physicians was described with 34% [23]. The adherence was evaluated for patients with inflammatory diseases as osteoporosis, colitis ulcerous, and neurological disorders, as schizophrenia or depression, metabolic diseases as diabetes and infections as HIV or tuberculosis. One study was evaluated with pediatric renal transplanted patients and their primary-caregivers and in another study several the adherence to several medications was investigated [20,23]. Furthermore a subgroup with different ethnic backgrounds were compared in two studies [11,20].
Study quality
Three studies were rated to be of high quality, eight of moderate quality and eight of low quality due to the review protocol (Table 1). Findings were a small sample size of study population, unblinded patient adherence data to the physician, a self-reported medication adherence method and a short period of follow up. Most of the studies used indirect methods for evaluate medication adherence (Table 1).
| Authors | Title | Performance Bias | Information Bias | Selection Bias | Detection Bias | Total Score |
|---|---|---|---|---|---|---|
| Macintyre et al. [12] | Patient knows best: blinded assessment of no nadherence with antituberculous therapy by physicians, nurses, and patients compared with urine drug levels. | 1 | 1 | 1 | 1 | 4 |
| Copher et al. [6] | Physician perception of patient adherence compared to patient adherence of osteoporosis medications from pharmacy claims | 0 | 1 | 1 | 1 | 3 |
| Loayza et al. [10] | Adherence to Antidepressant Treatment: What the Doctor Thinks and What the Patient Says | 1 | 1 | 0 | 1 | 3 |
| Hamann et al. [9] | Psychiatrist and patient responses to suspected medication nonadherence in schizophrenia spectrum disorders. | -1 | 1 | 1 | 1 | 2 |
| Trindade et al. [19] | Are your patients taking their medicine. Validation of a new adherence scale in patients with inflammatory bowel disease and comparison with physician perception of adherence. | 1 | 0 | &0 | 1 | 2 |
| Tucker et al. [20] | Self-regulation predictors of medication adherence among ethnically different pediatric patients with renal transplants. | 1 | 0 | 0 | 1 | 2 |
| Meddings et al. [13] | Physician assessments of medication adherence and decisions to intensify medications for patients with uncontrolled blood pressure: still no better than a coin toss. | 1 | 0 | 0 | 0 | 1 |
| Parker et al. [14] | Adherence to warfarin assessed by electronic pill caps, clinician assessment, and patient reports: results from the IN-RANGE study. | 1 | 1 | 0 | -1 | 1 |
| Phillips et al. [15] | Factors associated with the accuracy of physicians' predictions of patient adherence. | -1 | 0 | 1 | 1 | 1 |
| Roth et al. [16] | Accuracy of doctors' estimates and patients' statements on adherence to a drug regimen. | 0 | 1 | 0 | 0 | 1 |
| Zeller et al. [22] | Physicians' ability to predict patients' adherence to antihypertensive medication in primary care. | 0 | 1 | -1 | 1 | 1 |
| Gelb et al. [7] | Physician beliefs and behaviors related to glaucoma treatment adherence: the Glaucoma Adherence and Persistency Study. | -1 | 0 | 1 | 0 | 0 |
| Gross et al. [8] | Provider inaccuracy in assessing adherence and outcomes with newly initiated antiretroviral therapy. | 1 | 0 | -1 | 0 | 0 |
| Rubin et al. [17] | Impact of ulcerative colitis from patients' and physicians' perspectives: Results from the UC: NORMAL survey. | -1 | 0 | 1 | 0 | 0 |
| Ruslami et al. [18] | A step-wise approach to find a valid and feasible method to detect non-adherence to tuberculosis drugs. | 0 | 1 | 0 | -1 | 0 |
| Sidorkiewicz et al. [23] | Discordance Between Drug Adherence as Reported by Patients and Drug Importance as Assessed by Physicians. | -1 | 0 | 0 | 1 | 0 |
| Lutfey et al. [11] | Patient and provider assessments of adherence and the sources of disparities: evidence from diabetes care. | -1 | -1 | 0 | 1 | -1 |
| Curtis et al. [24] | Agreement between Rheumatologist and Patient-reported Adherence to Methotrexate in a US Rheumatoid Arthritis Registry. | -1 | 0 | 0 | -1 | -2 |
| Vincke et al. [21] | Therapy adherence and highly active antiretroviral therapy: comparison of three sources of information. | -1 | -1 | -1 | 0 | -3 |
Table 1: Study quality of the reviewed articles.
Outcomes
The adherence rates reported by the patients and the adherence rates assessed by the treating physicians are listed in Table 2.
| Estimation of Adherence/ Tendencies | Disease | Patient: Adherence Assessment Methods | Physician: Adherence Assessment Methods | Number of participating patients | Number of participating physicians | Outcomes according to patients | Outcomes according to physicians | Authors | |
|---|---|---|---|---|---|---|---|---|---|
| Overestimation | Inflammatory disorder | Osteoporosis | Medication Possession Ratio (MPR) | 4 Page-Questionnaire | 1587 | 412 | Adherent: 48.7% | Adherent: 69.2% (48,7% of patients were detected as adherent) | Copher et al. [6] |
| Rheumatoid Arthritis | Self-report | Confirmation in a self-report that their patient took methotrexate | 228 | Unknown | 8,3 % taking no MTX, 11.4% had missed one or more doses in the last 4 weeks - 13.3% in total | 100% | Curtis et al. [24] | ||
| Gastritis Ulcera | Bottle Count (actual intake), patients' self-report (Stated intake) | Estimation of the number of emptied patients' bottles | 116 | 3 | Mean actual intake: 47%+/-27%, Mean stated intake: 89%+/-17%, | 3 Doctors: 55%, 68%, 77% | Roth et al. [16] | ||
| Inflammatory bowl disease | Morisky Medication Adherence Scale (MMAS-8), Continious single-interval medication availability (CSA), Medication Possession Ratio (MPR), Questionnaire with one question | 1- Question Survey assessing the result of MMAS-8 (low, medium, high adherers to medication) | 110 | 13 | MMAS-8: 54 low adherers (85% non-persistent medication fill rates) | Agreement between physicians and MMAS-8:65%, 95% agreement of high adherers, 33% of low adherers Underestimation 5%, Overestimation 67% p<0.0001) | Trindade et al. [19] | ||
| Infectious disease | Tuberculosis | Urinary isoniazid levels, assessment with tick boxes like " always adherent" or "mostly adherent" | assessment with tick boxes like " always adherent" or "mostly adherent" | 173 | Unknown | Non-Adherent: 24% (urine INH), 76% (urine colour), 54% self-assessment | Non-Adherent: 11%, (nurses: 7%) | Macintyre et al. [12] | |
| HIV | Self report based on the protease inhibitor attitude scale | Questionnaire with one question (1: poor adherence, 5: excellent adherence) | 86 | Unknown | Mean: 2.1 +/- 1 | Mean: 4.5 +/- 0.5 Correlation: -0.25 (p=0.074) | Vincke et al. [21] | ||
| Eye disease | Glaucoma | Interview, Medication Possession Ratio (MPR) | Interview | 300 | 103 | Interview-Adherence: 89% MPR: 0.67 (50% ≤0.61) | Non-Adherent: 23% | Gelb et al. [7] | |
| Cardiovascular disease | Hypertension | Continous Multiple-interval measure of medication gabs (CMG) | 2- Question survey, answers with 1 point: "not at all" until 5 points: " a great deal" | 1064 | 92 | Non-Adherent: 20% (211 patients) | Non-Adherent: : 24% (285 patients)Physicians recognized non-adherence only 79 (37%) of the patients | Meddings et al. [13] | |
| MEMS (Timing Adherence (Primary Outcome), Visual Analog Scale (VAS) | Visual Analog Scale (VAS) | 42 | 9 | MEMS-Timing Adherence 82 +/-27 Correct dosing: 87 +/-24% Adherence: 94 +/-18 % | Adherence: 92 +/-15%, | Zeller et al [22] | |||
| Thrombose | MEMS, Self-report with yes/no-questions (Pill count in one center) | Questionnaire with yes/-no answers | 145 | (visits 812) | Non-Adherent: 37,3% | Non-Adherent: 17,2% | Parker et al. [14] | ||
| Chronic disease (mostly cardiovascular) | Medication Adherence Report Scale (MARS) | 1- Question survey | 228 | 24 | Mean: 0.0306 (0.69) | Mean: 4.04 +/- 0.75 | Phillips et al. [15] | ||
| Correctly | Inflammatory disorder | C. Ulcerosa | Internet surveys measuring adherence (49 multiple choice questions) | Internet surveys measuring adherence (30 multiple choice questions) | 451 | 300 | Non-Adherent: 46% | Non-Adherent: 41% | Rubin et al. [17] |
| Infectious disease | Tuberculosis | MEMS, Morisky questionnaire, pill count, visit attendance, patient diaries | Assesssment based on a short discussion about drug intake | 79 | Unknown | Non-Adherent: MEMS: 43% Morisky: 43%, Pill count: 47%, visit attendance: 26%, diary 23% | Non-Adherent: 50% | Ruslami et al. [18] | |
| Transplanted Patients | Renal Transplant patients | Cyclosporine level, Pill Count/Refill hystories, s, Frazier Noncompliance Inventory (FNI) | Primary Nephrologist's Adherence Rating Form (PNARF) | 68 | Unknown | African-American patients: cyclosporine level: 4,13, self-report:3,89, Pillcount/Refill:3,91 Caucasian patients: cyclosporine level: 4.44, self-report:4.37, Pillcount/Refill:3,58 | African-American patients: 4.06, Caucasian patients: 4.02 | Tucker et al. [20] | |
| Weak correlation | Various | different medications (hearth drugs, antihypertensive medications, oral blood glucose–lowering drugs and insulin and drugs for airway diseases, venous insufficiency, drugs for airway diseases, antidepressants and anxiolytics, drugs for treating bone diseases and drugs for treating symptoms such as functional gastrointestinal disorders or phlebotonic agents for venous insufficiency) | Self-report | Evaluation of each drug taken, whether its intake is essential for the patient | 128 | 256 | 68.1% patients reported good adherence 18.9% patients reported poor adherence (nonadherence) | correlation patient and physician assessments of drug adherence for 488 drugs: r = −0.25; 95% CI, −0.37 to −0.11; correlation between patient and physician assessments of drug importance (r = 0.07; 95% CI, 0.00–0.13 | Sidorkiewic et al. [23] |
| Underestimation | Mental disorder | Schizophrenia | Interview with general and specific questions | Interview with general and specific questions and 5-Point- rating scale ( 1: no role, 5: the most important role for admission as a consequence of non-adherence) | 213 | 121 | Non-Adherent: 40% | Non-Adherent: 53% | Hamann et al. [9] |
| Depression | Drug plasma concentration, Morisky questionnaire as self-reported medication-taking scale from 0-4 point score ( 4 points: poor adherence) | Rating skale on a 0-4 point score ( 0 points : very good adherence, 4 points: poor adherence) | 104 (99 adherence data estimated by physicians) | Unknown | Scale 0 points: 31%, 1 points: 37%, 2 points: 22%, 3 points: 11%, 4 points: 0 %, Blood concentration: 7% undedectable or low, 30% possibly partially non-adherent | Scale 0 points: 23%, 1 points: 46%, 2 points: 20%, 3 points: 8%, 4 points: 2% Estimation significantly different (p=0.009) 29 cases overestimation 31 cases underestimation, self-reported adherence better than estimation by physicians | Loayza et al. [10] | ||
| Metabolic disorder | Diabetes | 20-Minute telephone survey, Rating Skale of 0-10 (0: poor adherence and 10: good adherence) | 1 Page- 5- Item questionnaire, Rating Skale of 0-10 (0: poor adherence and 10: good adherence) | 156 | Unknown | Race White 7.8, Black 7.1, Other 6.6 | Race White 7.0, Black 5.4 (p<0.01), Other 6.3 | Lutfey et al. [11] | |
| Infectious disease | HIV | MEMS | Telephone assessment: e.g. estimation of of the percentage adherence over 4 months/during the study | 40 | 19 | Unknown | Overestimation: 38%, Underestimation: 55%, exact estimations: 8% | Gross et al. [8] | |
Table 2: Summary of the methods and outcomes of each reviewed article, sorted by estimation of adherence and after disease (direct adherence and MEMS measurements are highlighted).
In three out of 19 studies no difference between the adherence assessments of patients and physicians got obvious. Most of the studies showed a discrepancy of estimation the adherence and doctors tend to overestimate patients adherence as shown in Table 2. In four studies the difference of medication adherence data of patients and their physicians was statistical significant.
Physicians’ assessment of medication adherence was conducted in 15 diseases (e.g. HIV, tuberculosis, diabetes). Adherences of patients with mental disorder were underestimating by physicians. Further correlations between disease and physicians’ assessment couldn’t be found. One study showed a significance discrepancy about physicians’ estimation compared to self-assessment in adherence of black people (Table 2). In one study the physician experience was a significantly predictor of estimation the patient adherence. Physicians in practice to 10-14 years estimated 4.3% fewer patients to be adherent than physicians under 10 years in practice (p=0.038) [6]. In the study of Sidorkiewicz et al. physicians categorized 339 drugs (68.1%) as important, patients reported good adherence to these drugs. But for the other 94 drugs (18.9%), patients reported poor adherence even though their physicians evaluated them as important as for example heart drugs [23].
In 16 studies self-reported medication adherence methods and in three studies MEMSTM as indirect methods were used. Methods to detect adherence directly were conducted in three studies. Physicians mostly assessed the adherence with one- or two-question-surveys or a rating scale. In one study, the physicians and the patients assessed the adherence with the same method, a visual analog scale.
Supplementary material: Supplementary Table 1 Summary of the reviewed articles.
Only three studies were rated to be of high quality. Only one study was given 4 points. 16 studies were of moderate or low quality. Mostly the “information” and the “selection” were biased.
The sample size of patients’ and physicians’ varied for each study. As described in one study the response rate of physicians in participating was very low [23]. The simple size in studies with MEMSTM bottles was smaller due to the higher effort of conducting the study. Most studies were conducted in patients with inflammatory diseases followed by HIV and tuberculosis.
The assessments of adherence to medication treatment by patients and physicians were mostly different. They tended to overestimate the medication adherence of patients. One reason is the short or missing communication between the physician and its patient. In one study patients assessed that physicians did not inform them sufficiently about the importance of the right medication administration and about the side-effects [10]. If the patients discontinued the therapy, most of them did not share this information with their physician [10]. Physicians should also focus on the adherence during a conversation. Additional pharmaceutical care programs enhancing adherence should also be implemented. Pharmaceutical care involves cooperation with patients and health care providers. It is necessary to cooperate with the individual patient in order to improve medication adherence, the monitoring of the medication intake, and the prevention of adverse events. Studies, how pharmacists assed the adherence of the patients, are not available.
No difference in estimated adherence were found in one study since the physician assessed the adherence after a discussion about medication administration with the patient [18]. Physician assessment may depend also on the character of physician and the duration of collaboration with the patient. Physicians’ practice experience had a positive effect on assessing the adherence of their patients [6].
Studies with a low number of physician participants may be biased in both directions, since every physician wants to have good quote of adherers. In one study it was mentioned that the physician was blinded to the adherence data of the patients [19]. In the study of Parker, et al. the physicians had solely access to the INR-levels of their patients [14]. Whereas in the study of Copher, et al. the physicians had no access to the patients’ assessment. A correlation between physicians’ assessment and the type of disease exists only for mental disorders. Physicians tended to underrate the adherence rates of their patients [9,10]. Maybe they underestimate the patients in their ability. Further correlations didn’t exist. In general, physicians seemed to overestimate the adherence independent of other diseases.
Limitations of the review were the different measurement methods to detect adherence, since the results of the studies could not be easily compared. Most of the studies used self-assessment tools. These indirect methods to evaluate the adherence are less valid. Results of self-reported medication adherence showed usually higher adherence rates than using MEMSTM or direct adherence methods. In two studies the non-adherence measured by a direct method was worse than measuring by an indirect method [10,12]. It may also a reason for an agreement of the results between physicians’ and patients’ assessments. No unique process exists to evaluate physicians’ assessment on medication adherence. On a daily basis, assessments for physicians should be kept short and manageable with the work. Ranking scale to assess the adherence seemed to be a reliable tool. Furthermore if the score of the patients’ self- assessment-questionnaire is the same as the ranking, it might be easier to analyse the data.
Another limitation was the publication bias. Publications were excluded due to different language than English or German or not listed with MESH-terms in databases. In addition some publications had no more information than the title or the abstract. We contacted the authors of the publications to get further information or the full article without any response.
Physicians assessed medication adherence of their patients mostly incorrect. They tend to overestimate the medication adherence of patients. Only in mental disorders they tend to underrate. A visual analog scale seems to be a good method to assess physicians’ estimation of patients’ adherence. Patients’ adherence should be measured by directs methods or MEMSTM.
For evaluating the non-adherence in patients the physicians have to discuss the medication regimen with the patient and have to ensure the adherence of the patients.
The authors have not conflicts of interest to declare.
| Author | Copher R, Buzinec P, Zarotsky V, Kazis L, Iqbal SU, Macarios D. [6] |
| Titel | Physician perception of patient adherence compared to patient adherence of osteoporosis medications from pharmacy claims |
| Participants | 1587 patients with postmenopausal osteoporosis, mean age: 62.3 years, 412 physicians, |
| Study design | Prospective cohort study in the U.S., patients were health plan enrollees, Patients: Medication Possession Ratio (MPR), physicians: 4 Page-Questionnaire |
| Meausures of adherence (in detail) | MPR ≥80% 'adherent', MPR <80% 'non-adherent', physicians' assessment after 1 year of therapy |
| Outcomes | Patients' adherence: 48.7%, Physicians' estimation: 69.2% adherend patients (48,7% of patients were detected as adherent), physicians' experience was a statistically significant predictor for assessing patients' medication adherence |
| Notes | Conclucions: Physicians overestimate patients medication adherence to osteoporosis therapies. Suggestion: More dialogue between physicians and patients for improving physician awareness of medication non-adherence |
| Author | JR Curtis, A Bharat, L Chen, JD Greenberg, L Harrold, JM Kremer, T Sommers, and D Pappas [24] |
| Titel | Agreement between Rheumatologist and Patient-Reported Adherence to Methotrexate in a U.S. Rheumatoid Arthritis Registry |
| Participants | 1.) 228 patients were in the last six months of registration at the rheumatologist and ingested methotrexate (MTX) against their rheumatoide arthrits, , [missed 1 or more MTX dose(s): 45, mean age: 51,96 years, 15,6 % male, 84,4 % female, Clinical Disease Activity Index: 15,92 %, modified Health Assessment Questionnaire: 0,50 %, physician global: 26,31 %, Patient Global: 29,94 %, Patient Pain: 31,60 %, Disease duration: 8,85 years, Glucocorticoid use: 33,3 %, Biologics: 91.1%, Methotrexate use oral: 73.1%, Methotrexate use subcutaneous: 26.9%] [took all MTX dose(s): 183, mean age: 53,49 years, 20,2 % male, 79,8 % female, Clinical Disease Activity Index: 14,39, modified Health Assessment Questionnaire: 0,47, physician global: 23,35, Patient Global: 25,86, Patient Pain: 27,06, Disease duration: 8,23 years, Glucocorticoid use: 24 %, Biologics: 94,5 %, Methotrexate use oral: 78,1 %, Methotrexate use subcutaneous: 21,9 %] |
| Study design | Place: 984 patients were admitted to the survey, 430 responded, 228 patients have been enrolled in the last, Factors associated with RA patients missing some or all MTX doses in the last 4 weeks whose rheumatologist reported MTX use at the most recent registry visit, data from the Consortium of Rheumatology Researchers of North America (CORRONA) RA disease registry |
| Meausures of adherence (in detail) | Cross-sectional, Internet-based survey of RA patients (Patient self-report was the gold standard compared to MTX) : “Are you currently taking methotrexate for your rheumatoid arthritis? Methotrexate is usually taken once weekly” and “Many people find it sometimes difficult to take methotrexate because of side effects or other reasons. In the last 4 weeks, how many weekly doses of methotrexate do you think that you have taken?”, Physicians confirmed that their patient took methotrexate during their last visit to the doctor |
| Outcomes | 45 patients (19.7%) said on the survey that they either were not taking MTX (n=19, 8.3%) or had missed one or more doses in the last 4 weeks (n=26, 11.4%), In the subgroup analysis of patients (n=149): results were similar: 2,6 % of patients (n=4) said that they had discontinued MTX, 10.7% of patients (n=16) said that they had missed one or more doses in the last 4 weeks (13.3% in total, mainly due to one or more missed doses rather than overt discontinuation), No significant risk factors associated with adherence after multivariable adjustment |
| Notes | Conculsions: Physicans tend to overestimate the adherence |
| Author | Gelb L1, Friedman DS, Quigley HA, Lyon DW, Tan J, Kim EE, Zimmerman TJ, Hahn SR. [7] |
| Titel | Physician beliefs and behaviors related to glaucoma treatment adherence: the Glaucoma Adherence and Persistency Study |
| Participants | 1.) 300 patients with a primary open-angle glaucoma (POAG); 2.) 103 physicians, 8% female |
| Study design | Retrospective survey (data source: HealthCore Managed Care Database, Wilmington, DE) and patients' data from the Glaucoma Adherence and Persistency Study (GAPS); adherence measuring methods: (1) patients' self-report (2) physicians' estimations (3) retrospective analysis of the claims for 13,977 patients in the HealthCore Managed Care Database |
| Meausures of adherence (in detail) | (1): Telephone interview (2): 30-Minute interview |
| Outcomes | Physicians' estimations: 23% patients with nonadherence that affects clinical outcomes and ability to detect 37% of those; patients' self-report: 89% claim to take their medication every day; mean (MPR): 0.67, half of the patients interviewed with a MPR of 0.61 or lower |
| Notes | Conclusions: Physicians should seek for opportunities to adress medication adherence |
| Author | Gross R1, Bilker WB, Friedman HM, Coyne JC, Strom BL. [8] |
| Titel | Provider inaccuracy in assessing adherence and outcomes with newly initiated antiretroviral therapy |
| Participants | 1.) 40 patients with HIV, protease inhibitor naive, viral loads greater than 10 000 copies/ml, newly started on nelfinavir in standard combinations; 2.) 19 providers, mean age: 38 years, 53% female, 47% female, 15 (79%) physicians, 4 (21%) nurse-practitioners, all white, mean number of patients referred per provider: 2 |
| Study design | Prospective cohort at the University of Pennsylvania; adherence measuring methods: (1) MEMS (2) providers' assessment |
| Meausures of adherence (in detail) | (2): Telephone assessment within 7 days of enrollment: prediction, whether the patient would become undetectable after 4 months, prediction of adherence over 4 months; adherence data not available during study duration, clinically obtaine data available |
| Outcomes | No correlation between predicted and actual adherence by providers (overestimation: 38%, underestimation: 55%, exact estimations: 8%); 26 of 40 predictions (65%) missed by more than 10%; physicians' prediction of undetectable viral loads was no better than chance agreement; positive correlation between providers' estimates after 4 months and actual adherence (overestimation: 44%, underestimation: 50%, exact estimations: 6%); 16 out of 34 estimates (47%) missed by more than 10% |
| Notes | Conclusions: Providers more accurate in their post-hoc estimation of adherence than prediction of adherence although still inaccurate; HAART should not be withheld solely on providers' assessment of adherence; other predictive instruments should be contemplated when assessing adherence to HAART |
| Author | Hamann J1, Lipp ML1, Christ-Zapp S1, Spellmann I1, Kissling W1. [9] |
| Titel | Psychiatrist and patient responses to suspected medication nonadherence in schizophrenia spectrum disorders |
| Participants | 1.) 213 inpatients with either schizophrenia or a schizoaffective disorder; 2.) 121 physicians, 66 women, 55 men, mean age: 35.9 years, mean work experience: 5.9 years |
| Study design | Place: 22 psychiatric hospitals in 3 areas of Germany (city of Hamburg and urban and rural areas of both Bavaria and Saxony), state and university hospitals; adherence measuring methods: (1) patients' self-report (2) physicians' estimation |
| Meausures of adherence (in detail) | (2): Estimation of adherence in the weeks before hospital admission; both (1) and (2) performed as face-to-face interviews |
| Outcomes | Physicians' judgment: taken amount of the medication prescribed: 68% ± 37%, nonadherence rate: 53% (intake ratio of ≥ 80% defined as adherent); Patients' self-report: taken amount of the medication prescribed: 75% ± 39%, non-adherence-rate: 40%; physicians more sceptical towards adherence; physicians' estimation of adherence significantly predicted number of implemented adherence measures |
| Notes | Conclusions: Objective adherence measures (e.g. plasma levels) may be helpful for physicians to become more aware of non-adherence |
| Author | Loayza N, Crettol S, Riquier F, Eap CB. [10] |
| Titel | Adherence to Antidepressant Treatment: What the Doctor Thinks and What the Patient Says 104 outpatients with mood and/or anxiety disorder in treatment with antidepressives, 53% male (mean age: 43 years), 47% female (mean age: 39 years), further medication for 85% (8% of those with 2 different antidepressives), mean treatment duration: 12 months, 30% with anxiety disorder, |
| Participants | 37% with mood disorder, 32% with both |
| Study design | Place: Hopital de Cery, Prilly-Lausanne, Schweiz; transversal observational study; adherence measuring methods: (1) patients' interviews (investigator not involved in follow-up, but access to patients' medical charts) (2) drug plasma concentration (for all antidepressants except nefadozone and doxepine, blood sampling immediatly after recruitment and interview, patients informed that data collected would not be transmitted to treating physician) (3) doctors' assessment; furthermore measured: (4) patients' satisfaction with treatment (questionnaire) (5) strenght of patient-therapist alliance (Helping Alliance questionnaire (HAq-II)) |
| Meausures of adherence (in detail) | 4 (0: very good adherence, 4: poor adherence) for 99 patients |
| Outcomes | (8%), 4 points (2%), mean amount of points: 1 point; patients' and physicians' assessments significantly different though weakly correlated; adherence overestimation in 31% of the cases, underestimation in 29% of the cases; no significant differences between adherence assessments of patients with non-detectable or low serum levels and other patients or between patients with |
| Notes | Conclusions: Drug monitoring could be useful to assess patients' adherence |
| Author | Lutfey KE1, Ketcham JD. [11] |
| Titel | Patient and provider assessments of adherence and the sources of disparities: evidence from diabetes care |
| Participants | 156 patients with diabetes, 42.9% male, 57.1% female, 81.4% white, 17.3% black, 3.2% other |
| Study design | Telephone survey of patients and post visit survey of their providers; place: 2 endocrinology clinics in the same university-based medical center in a large Midwestern city (one clinic mainly visited by white, college educated, insured patients, the other mainly by minority, high school educated, underinsured patients); recruitment time: 3 months; adherence measuring methods: (1) providers' assessment of patients' adherence (2) patients' self-report |
| Meausures of adherence (in detail) | (1): 5-item questionnaire (2) 20 minute telephone survey containing additional questions; questions identically framed for (1) and (2), rating of the patient's adherence on a scale of 0-10 (0: poor adherence and 10: good adherence) |
| Outcomes | Providers' assessments significantly influenced by patient observable characteristics (e.g. age, race): assessment of adherence lower for black patients (1.2 points below their average assessment of white patients), absolute difference between patients' and providers' assessments greater for black patients (67% higher), patients' assessments closer to providers' assessments for patients at the age of 45-54 years than for those at the age of 18-44 years, absolute differences significantly smaller on average for patients at the age of 45-54 years than under 45 years; providers' assessments less influenced by characteristics more difficult to observe (e.g. education); |
| Notes | Conclusions: Providers' assessments rely on observable cues (e.g. age, race) but less on characteristics more difficult to explore; physicians seem to be more uncertain about black patients' adherence perhaps due to communication difficulties; physicians seem to be less uncertain about adherence of young patients than about adherence of black patients |
| Author | Macintyre CR1, Goebel K, Brown GV. [12] |
| Titel | Patient knows best: blinded assessment of nonadherence with antituberculous therapy by physicians, nurses, and patients compared with urine drug levels |
| Participants | public health TB nurses working full time fo the state TB program; 3.) 6 senior infectious diseases physicians with long-term experience treating TB |
| Study design | direct observation of therapy; recrutiment phase from April 1998 until December 2000; place: 2 clinics in the North-Western Health Care Network, Victoria, Australia; adherence measuring methods: (1) isoniazid urine drug level (2) assessment of adherence by patients, doctors and |
| Meausures of adherence (in detail) | adherence defined as all six urinary isoniazid levels greater than 0 (2): once a month, patients, doctors and nurses blinded to the urine results, diary for patients with tick boxes for the intake of daily doses, options for doctors and nurses to assess patients' adherence: "always compliant", "mostly compliant", "sometimes compliant", "rarely compliant", "never compliant" and "unsure" |
| Outcomes | (urine INH), 76% (urine colour), 54% (patient), 11% (doctor), 7% (nurse); only 10 out of 19 patients who were assessed as regularly nonadherent had negative urine isoniazid levels; only 5 out of 19 patients were assessed as nonadherent by both doctos and nurses; patient, doctor and nurse reported nonadherence for only 4 patients where urine INH level was absent; doctors' sensivity of |
| Notes | ("patient knows best"); asking patients about adherence may be helpful in detecting problems with |
| Author | Meddings J1, Kerr EA, Heisler M, Hofer TP. [13] |
| Titel | Physician assessments of medication adherence and decisions to intensify medications for patients with uncontrolled blood pressure: still no better than a coin toss |
| Participants | 1.) 1064 Patients with diabetes, lowest BP in triage ≥140/90; mean age: 65 years, 97% men, mean of classes of BP medications: 2.9, average of prescription medications for all conditions: 6.3; VA was identified as primary source of care for diabetes; at least one chronic BP medication refilled at the VA; 2.) 92 primary care providers (64 physicians, 21 nurse practioners, 7 physician assistants), mean age: 48, mean of years in practice: 11.4, median of 12 patients in the study population |
| Study design | Analysis of medication adherence using data collected in a cross-sectional cohort study of patients scheduled for primary care visits with 92 primary care providers at 9 Department of Veterans Affairs (VA) facilities in 3 med-western states; Data sources: (1) VA automated data source for BP values at the time of study enrollment; (2) VA pharmacy records for 1 year prior to 90 days after enrollment for number of medications and number and refill history for antihypertensive medication classes; (3) provider's survey for each patient after clinic session; (4) patient's questionnaire after the visit about patients' characteristics |
| Meausures of adherence (in detail) | (2): Usage of the Continious Multiple-interval Gap (CMG) measure (= how many days over the past year did the patient not possess BP medications to take as prescribed [%], CMG ≥20% = clinically significant refill non-adherence): CMG calculation for each class of antihypertensives and calculation of composite CMG; (3): questionnaire with 2 questions assessing their patients' adherence (1. "How often does your patient adhere to the BP regimen? - 1 ("none of the time") to 5 ("all of the time"), 2. "How much does adherence make it difficult to control this patient's BP?" - 1 ("not at all") to 5 ("a great deal")), continous measure with total score of 2-10 and dichotomous version |
| Outcomes | Strong correlation between providers' responses to each of the 2 questions; overall assessment of good adherence, skewed toward lower scores; sssessment of adherence of non-white patients (Ø:4.92) was higher than assessment of white patients (Ø:4.07); 258 (24%) patients were assessed as non-compliant by their providers (using the dichotomous measure); a similar proportion of patients was identified as non-adherent by the gap (CMG ≥20%) in pharmacy refills (211 patients = 20%) and by providers (285 patients =24%) though both methods identified non-adherence for different patients -> providers recognized non-adherence for only 79 (37%) of the patients who had a CMG ≥20%; among patients with a CMG ≥50% providers were able to identify 8 (44%) as non-adherent; the mean CMG for patients identified as non-adherent by providers was 14%, the mean CMG for patients not identified by providers with adherence problems was 10%; overall result: => weak correlation between refill adherence scores and providers' assessments of adherence; in general overestimation of adherence by providers |
| Notes | Suggested solution: A simpler objective measure (e.g. CMG or ReComp) to help providers assessing their patients' medication adherence |
| Author | Parker CS1, Chen Z, Price M, Gross R, Metlay JP, Christie JD, Brensinger CM, Newcomb CW, Samaha FF, Kimmel SE. [14] |
| Titel | Adherence to warfarin assessed by electronic pill caps, clinician assessment, and patient reports: results from the IN-RANGE study |
| Participants | 145 patients within 2 months of initiating warfarin therapy with a target INR of 2.0-3.0, 73.8% male, 26,2% female, mean age: 57,9 ±14,6 years |
| Study design | IN-RANGE Study: prospective cohort study, 3 anticoagulation clinics in Pennsylvania: the Hospital of the Unisversity of Pennsylvania (HUP) in Philadelphia, the Philadelphia Veterans Affairs Medical Center (PVAMC) and the Hershey Medical Clinic (HMC) in Hershey, PA; adherence measuring methods: (1) MEMS cap (minimum of 7 days, either directly on a bottle or as a "diary") (2) patients' self report at all follow-up visits (3) clinicians' estimate of adherence; both patients and clinicians were blinded to data obtained by MEMS cap but not blinded to INR level at the time of their assessment/reporting of adherence |
| Meausures of adherence (in detail) | (1): Calculation of PMEMS, incorrect (= number of the days the participant either did not open the bottle with the MEMS cap when they were supposed to take a pill or opened it more than once divided by the number of days in the monitored period) (2): patients were asked how many pills they skipped and how many extra pills they took since the last visit, calculation of Pself,incorrect (= number of pills skipped and extra divided by the number of days since the last visit) (3): PVAMC: pill counts and then estimation of adherence, HUP and HMC: no pill count was performed |
| Outcomes | Physicians were more likely to assess patients as adherent than not (717 of 812 visits = 88.3%); odds of clinician assessing the patient as nonadherent were 2 times greater for visits at which participant was assessed nonadherent by MEMS cap (using PMEMS, incorrect ≥ 20% as "nonadherent") than for visits when he was assessed adherent by MEMS cap; clinicians tend to overestimate adherence: patients at 93 of 111 visits (83,3%) were rated adherent although PMEMS, incorrect was ≥50%; subgroup analyses comparing PVAMC to HUP/HMC to determine influence of pill counts: at PVAMC nonadherent patients were less likely to be assessed adherent (76,7%) than at HUP/HMC (90%) with PMEMS incorrect ≥20%; overall result: physicians' estimates were often different from that assessed by MEMS caps, adherence measured by MEMS cap identified more nonadherence than clinican assessment, physicians were less likely to incorrectly label a patient adherent when a pill count was conducted beforehand |
| Notes | Conclusion: Adherence needs to be readressed throughout follow-up by physicians |
| Author | Phillips LA1, Leventhal EA, Leventhal H. [15] |
| Titel | Factors associated with the accuracy of physicians' predictions of patient adherence |
| Participants | 1.) 228 patients, 64% women, mean age at time of visit: 56.83 (16.50), minority status: 30%, patient chronic status: 70% 2.) 24 physicians, 10 full primary care clinic faculty members and 14 residents under the supervision of the faculty (84% of the patients were seen by faculty physicians) |
| Study design | Place: primary care clinic; physicians' data: correlational and measured cross-sectionally; patient data: measured either cross-sectionally or longitudinally; adherence measuring methods: (1) Physicians' predictions of patients' adherence in the month after their visit and factors that may have influenced their predictions (2) Patients' self-report at the 1-month follow-up interview; additionally measured: (3) physicians' perceptions of agreement with the patients about illness and treatment and patients' perceptions of agreement with the physicians about illness and treatment |
| Meausures of adherence (in detail) | (1): 1 question: "How confident are you that the patient will follow the prescribed treatment: Not at all, a little bit, somewhat, quite confident, very confident?" (2): Medication Adherence Report Scale containing 5 items, each on a 5-point scale from "always" to "never" (e.g. "Did you ever forget to do your treatment?"), 5 items were averaged into a composite |
| Outcomes | Physicians' predictions were weakly but significantly and positively correlated with patients' self-reported adherence; patients' minority status was significantly associated with phyisicians' predictions of adherence but no association with patients' chronic ill status, gender or age was found; physicians' predictions of adherence were significantly and positively correlated with physicians' perceptions of agreement with the patients |
| Notes | Physicians' predictions might be poor due to association with patients' minority status; it has to be examined whether it would be advantageous to physicians' predictions if physicians' were more aware of the effect that discussing illness/treatment specifics with patients has on patients' adherence |
| Author | Roth HP, Caron HS. [16] |
| Titel | Accuracy of doctors' estimates and patients' statements on adherence to a drug regimen |
| Participants | 1.) 116 patients with peptic ulcers taking antacides, mean age: 46 years, 77% male, 23% female, 37% white, 63% black 2.) 3 physicians trained in gastroenterology |
| Study design | Places: Cleveland Veterans Administration Hospital and outpatient clinics of University Hospitals, Mt. Sinai Hospital, and the Veterans Administration Regional Outpatient Service; adherence measuring methods: (1) bottle count ("actual intake") (2) patients' self-report at home visits ("stated intake") (3) physicians' estimations at 10 follow-up visits |
| Meausures of adherence (in detail) | (3): estimation of emptied bottles in the previous month, physician blind to his patient's adherence to the regimen |
| Outcomes | Measuring results: mean stated intake: 89%, mean actual intake: 47%, mean estimated intake: 71%; physicians' estimate too high in most cases with an overestimation of about 50%, true degree of error: 30% of the prescribed amount; physicians especially inaccurate in patients with low intake; poor correlations between estimates and actual intake; physicians based their estimations on patients' self-report in 84% of the cases; accuracy in estimation did not improve with increasing familiarity with a patient; one doctor more accurate in assessing patients with characteristics similar to his own; physicians' estimates still more accurate than patients' statements; |
| Notes | Conclusions: (1) possible reasons for poor estimations: lack of objective data on which to evaluate estimates, basing estimates on patients' statements, basing estimates on patients' demographic characteristics (2) combining pill or bottle count and blood or urine tests might be helpful to measure adherence more adequately |
| Author | Rubin DT1, Siegel CA, Kane SV, Binion DG, Panaccione R, Dubinsky MC, Loftus EV, Hopper J. [17] |
| Titel | Impact of ulcerative colitis from patients' and physicians' perspectives: Results from the UC: NORMAL survey |
| Participants | US patients and physicians; 1.) 451 patients with confirmed diagnosis of UC, 37% male, 67% female, mean age: 45 years, mean of 10 years since first diagnosis of UC, mean age at diagnosis: 35 years; 2.) 300 gastroenterologists, all of them spent at leat half of their time in clinical practice, physicians saw 11-20 patients with UC per month |
| Study design | 2 self-administered, cross-sectional national internet surveys measuring adherence among other things by (1) patients' self report and (2) physicians' assessment of patient adherence |
| Meausures of adherence (in detail) | (1): 49 multiple-choice questions (e.g. patient demographics, adherence to aminosalicylate therapy) (2): 30 multiple-choice questions (e.g. relationship with patient, patient adherence) Correspondence between self-reported adherence and physicians' estimate of patient adherence e.g. regarding the question: "I have taken all the medication I have been prescribed over the |
| Outcomes | previous 7 days." Response by patients: 54% compared to physicians' estimate: 59% |
| Notes | - |
| Author | Ruslami R1, van Crevel R, van de Berge E, Alisjahbana B, Aarnoutse RE [18] |
| Titel | A step-wise approach to find a valid and feasible method to detect non-adherence totuberculosis drugs |
| Participants | 79 pulmonary TB patients in the first 2 months of TB treatment, mean age: 32 years, 49% male, 51% female, 80% with low income and low educational level, all patients taking TB drugs and pyridoxine according to National TB program |
| Study design | Prospective study; place: outpatient urban pulmonary clinic (BP4) in Bandung, Indonesia; adherence measuring methods: (1) patients' self-assessment (2) physicians' assessment (3) pill count (4) visit attendance (5) patients' diaries for drug intake (6) MEMS bottle |
| Meausures of adherence (in detail) | (1): Morisky questionnaire (2): based on short discussion about drug intake (4): adherence 100%: patient showed up to the appointment, adherence 0%: patient didn't show up (6): for only 30 patients; adherence values below 100% or medium/low Morisky scale were considerd as non- adherence |
| Outcomes | Patients assessed as non-adherent: 43% (Morisky-scale), 50% (physicians' estimation), 47% (pill count), 26% (visit attendance), 23% (diary), 43% (MEMS); physicians' sensitivity for detecting non- adherence: 85%, specificity: 71%, positive predictive value: 69%, negative predictive value: 86% (compared to MEMS); identification of all non-adherent patients (sensitivity: 100%, highest sensitivity of all methods) by combining self-report and physician assessment; no added value by combining pill count and physician assessment |
| Notes | Conclusions: Physician assessment is considered a feasible method for assessing adherence; a combination of methods may lead to better adherence assessment |
| Author | Sidorkiewicz S, Tran VT, Cousyn C, Perrodeau E, Ravaud P. [23] |
| Titel | Discordance Between Drug Adherence as Reported by Patients and Drug Importance as Assessed by Physicians. |
| Participants | 1.) 128 patients taking 498 different medications (hearth drugs, antihypertensive medications, platelet aggregation inhibitors, cardiac agents, oral blood glucose–lowering drugs and insulin and drugs for airway diseases, venous insufficiency, drugs for airway diseases, antidepressants and anxiolytics, drugs for treating bone diseases such as osteoporosis and drugs for treating symptoms such as functional gastrointestinal disorders or phlebotonic agents for venous insufficiency), mean age: 59.8 years, 28,9 % male, 71,1 % female, Average number of drugs per patient: 3, for each patient: 2 investigators (C.C. and S.S.) identified drugs prescribed for long-term use by reviewing medical records, mean age of physicians: 57,4 years, 41,0 % male, 59 % female, general practitioners: 94,9 %, 2.) from 6 general practices and 6 care units of university hospitals in France |
| Study design | Place: 6 general practices and 6 care units of university hospitals in France (1) data collection by means of questionnaires for patients and doctors respectively |
| Meausures of adherence (in detail) | (1):questionnaires: 1. self-report: adherence to the drug - levels ranging from 1 (high drug adherence) to 6 (drug discontinuation) 2. “I am convinced of the importance of my prescription medication,” - levels ranging from 6-step scale from “agree completely” to “disagree completely.”3. “If you happen to skip doses, why? (eg, omission, drug side effect, too much medication to take).” Physicians should evaluate each drug taken, whether its intake is essential for the patient - levels ranging from 11-steps from 0 (not important) to 10 (very important), they got less and other questions than the patients. |
| Outcomes | Discordance between patient and physician evaluations of drug adherence and drug importance. For 339 drugs (68.1%), patients reported good adherence to drugs evaluated as important by their physicians, but for 94 drugs (18.9%), Patients reported poor adherence (nonadherence) even though their physicians evaluated them as important |
| Notes | Only 34% of physicians participating in the study |
| Author | Trindade AJ1, Ehrlich A, Kornbluth A, Ullman TA. [19] |
| Titel | Are your patients taking their medicine? Validation of a new adherence scale in patients with inflammatory bowel disease and comparison with physician perception of adherence |
| Participants | 1.) 110 patients with Inflammatory Bowel Disease (IBD), 49% male, 51% female 2.) 13 gastroenterologists specializing in IBD |
| Study design | Places: IBD-specializing gastroenterology offices in New York and a single tertiary-care medical center in NY; adherence measuring methods: (1) patients' self-report (2) pharmacy fill rates (3) physicians' perception |
| Meausures of adherence (in detail) | (1): Morisky Medication Adherence Scale (MMAS-8), questionnaire administered within 24 hours of admission, physicians blinded to the questionnaire and the results, assessment: fewer than 6 points: low adherence, 6-7 points: medium adherence, 8 points: high adherence (medium and high adherers combined into a single group "medium and high adherers" for analysis) (2) pharmacy records for refill dates for a 1-month supply of medication, each patient 4 one-month-supply refill dates, calculation of the continous single-interval medication availability (CSA = dividing the day's supply obtained at a pharmacy fill by the number of days before the next pharmacy fill for that same medication) and mean possession ratio (MPR= sum of the day's supply obtained between the first pharmacy fill and the last fill, divided by the total number of days in this period), CSA and MPR < 0.8 defined as low adherence (3) 1-question survey to divide patients into the 4 groups patients belong to in accordance to MMAS-8: low adherer, medium adherer, high adherer, not determined |
| Outcomes | MMAS-8: 54 low adherers (85% with nonpersistent medication fill rates as per CSA) and 56 medium or high adherers (11% with nonpersistent medication fill rates), similar results for MPR; rate of agreement between phyisicans' assessment and MMAS-8: 65%, 95% agreement for high adherers but only 33% for low adherers; underestimation of adherence by physicians in only 5% of the cases, overestimation in 67% of the cases |
| Notes | Conclusions: Physicians should systematically measure adherence at every visit e.g. by using adherence surveys such as the MMAS-8 or specific questions out of it |
| Author | Tucker CM1, Petersen S, Herman KC, Fennell RS, Bowling B, Pedersen T, Vosmik JR. [20] |
| Titel | Self-regulation predictors of medication adherence among ethnically different pediatric patients with renal transplants |
| Participants | 68 pediatric patients with renal transplants (functional for at least 6 months) and their primary caregivers, 26 African American patients (6 female, 20 male, mean age: 12.90), 42 Caucasian patients (21 female, 21 male, mean age: 15.00), over half of the participants in both ethnic groups with low incomes |
| Study design | Place: 4 Southwestern pediatric nephrology clinics; adherence measuring methods: (1) patients' self-report (2) physicians' assessment (3) pill count/refill histories (4) cyclosporine levels; furthermore measured: (5) motivation to be adherent, perceived control of/responsibility for adherence, perceived support of adherence from primary caregiver (all via the Self-Regulation of Medication Adherence Battery (SRMAAB)) |
| Meausures of adherence (in detail) | (1): Frazier Nonadherence Inventory (FNI), 11 items rated on a 5-point Likert scale assessing how often patient does not take medication for general reasons (1 = very often, 5 = very adherent) (2): Primary Nephrologist's Adherence Rating Form (PNARF) assessing the patient's overall adherence (1 = very non adherent, 5 = very adherent) (3): obtained by pharmacy refill history data (zathioprine, cyclosporine and prednisone pills), adherence rating from 1 = very non adherent to 5 = very adherent (4): recording of each patient's most recent cyclosporine level, adherence rating from 1 = very nonadherent to 5 = very adherent |
| Outcomes | Mean adherence ratings: 1.) African American patients: 4.13 (cyclosporine levels), 3.89 (self- report), 4.06 (nephrologist's rating), 3.91 (pill count/refill hisstory), 2.) Caucasian patients: 4.44 (cyclosporine levels), 4.37 (self-report), 4.02 (nephrologist's rating), 3.58 (pill count/refill history); significant positive correlation between cyclosporine levels and medication adherence ratings by nephrologists for African American patients; motivation to be adherent and perceived control of medication adherence significantly predicted adherence as rated by nephrologists for African American patients |
| Notes | Conclusions: Use of multiple measures of medication adherence is recommended |
| Author | Vincke J1, Bolton R. [21] |
| Titel | Therapy adherence and highly active antiretroviral therapy: comparison of three sources of information |
| Participants | 86 patients with HIV, 78.6% male, 21.4% female, mean age: 41.2 ± 9.1 years, almost 30% with income below the poverty level |
| Study design | Place: French- and Flemish-speaking areas of Belgium; adherence measuring methods: (1) patients' self-report (2) evaluation by the patient's designated most significant other (3) evaluation by the medical staff |
| Meausures of adherence (in detail) | (1): based on the protease inhibitor attitude scale developed by Weiss, 3 questions, total score calculated by dividing the sum of all three questions by 3 (2): same 3 questions as (1) (3): 1 question about their estimation of adherence; all three measuring methods referred to the adherence of the last 4 weeks |
| Outcomes | Mean score of medical staff's estimation of adherence 4.5 (SD=0.5) indicates high adherence; weak correlations between medical staff's estimation and either self-report or report by one's most significant other; doctors report higher adherence for female patients, patients with higher benefits, patients with lower barriers, patients with medical treatment that is not too complex and patients who are less satisfied with the doctor-patient relationship |
| Notes | Conclusions: When using a theoretical framework such as the health belief model as standard to evaluate variations in adherence, the use of physicians' estimations seems to be the most reliable method as they have access to medical files |