Cell & Developmental Biology
Open Access
ISSN: 2168-9296
ISSN: 2168-9296
Research Article - (2012) Volume 1, Issue 1
Cardiac and respiratory systems malformations are some of the most common and severe congenital defects and they often co-exist with anomalies of neck and chest wall – the multiple malformations phenotypes. In this study, a survey was performed on the incidence of such defects in the database of the Estudio Colaborativo Latino Americano de Malformaciones Congenitas, in live-born infants of the Complexo Hospitalar da Irmandade Santa Casa de Misericórdia de Porto Alegre (Porto Alegre, Rio Grande do Sul State, Brazil), from January 2004 to December 2006. From a total of 259 newborns found in this period containing malformations, 30 had anomalies in the thoracic region (here named “thoracic malformations group”) of multiple and simultaneously occurring subtypes: cardiac, pulmonary, neck and chest wall. Among the analyzed variables, it was observed that live-born infants of the thoracic malformations group have reduced birth weight, are more frequently girls, have shorter gestational age at birth, have older fathers and have mothers that smoke less but that have more chronic diseases during pregnancy, in relation to the control group. The conclusion of the present work is that paternal-maternal-dependent variables seem to significantly contribute as causing agents of thoracic defects in general.
<Keywords: Congenital abnormalities, Congenital heart defects, Respiratory system abnormalities, Musculoskeletal abnormalities
MF: malformation; LBI: Live-Born Infants; ECLAMC: Estudio Colaborativo Latino Americano De Malformaciones Congenitas; ISCMPA: Irmandade Santa Casa de Misericórdia de Porto Alegre; MG: Malformed Group; CG: Control Group; GA: Gestacional Age; PA: Paternal Age
The thorax is one of the most complex structures of the human body, containing several systems that are responsible for many vital functions. The upper and lower airway systems and the cardiac system, work together, aided by the thoracic wall, in order to allow adequate nutrition and exchange of substances between blood and tissues. The esophagus, on the other hand, is the organ responsible for taking food to the lower digestive tract.
It is very well known that these organs and structures are closely related embryologically, either spatially and temporally, since they develop in approximately the same embryological period and are originated from the same tissue layers [1-6]. Although this suggests similar etiologies and risk factors for thoracic MFs occurring in each separate above mentioned organ or structure, there is no available data regarding population prevalence and incidence of pooled thoracic MFs (in example, MFs of the subtypes: cardiac, pulmonary, neck and chest wall analyzed as a whole entity). On the other hand, there is plenty of data concerning individual subtypes of thoracic MFs. For example, it is known that, among the chest wall anomalies, pectus excavatum corresponds to 90% of them, being characterized by depression of sternum and adjacent ribs and occurring at a frequency of aproximately 1:300, more commonly in males than in females (5:1) [7]. Pectus carinatum, on the other hand, is characterized by protrusion of sternum and adjacent ribs, corresponding to 10-15% of congenital chest wall defects and also occurring more frequently in males (4:1) [8]. Ribs MFs are rarer, although case reports are available [9].
About upper airway MFs, they occur from the nasal opening to the subglotis and can cause severe respiratory disfunction; among them, the ones present in the thorax are larynx and subglotis defects. The most common upper airway and larynx MF is laringomalacia – which consists on the collapse of supraglotic structures, epiglottis, aryepiglottic folds and mucosa aritenoidea during inspiration - corresponding to 60% of all larynx anomalies and occurring more frequently in male newborns (2:1) [10]. Other significant upper airway MFs are vocal cord paralysis and subglotic stenosis.
Congenital pulmonary anomalies, on the other hand, occur at a frequency of 2% [11]. Among the most common of them are pulmonary sequestration, congenital cystic adenomatoid formation, congenital lobar emphysema and bronchogenic cysts, being relatively common the simultaneous presence of many of such diseases [12,13]. Secondary pulmonary hypoplasia due to congenital diaphragmatic hernia and cystic adenomatoid formation also contribute to the high newborn morbi-mortality [11].
Regarding congenital cardiac MFs, the ones of valves and septum, together, are observed in 6:1.000 LBIs [14,15]; on the other hand, valve defects, which have a prevalence of 1,5% in the general population, may remain undetected until adult life [16]. Such anomalies confer high morbidity and lead death causes by congenital defects [17].
Finally, of the esophageal anomalies, the most common and significant is esophageal atresia with or without tracheoesophageal fistulae (interruption of the continuity of the esophagus at the proximal portion, most frequently with a fistula communicating the trachea with the esophagus around the region of the carinae), with an incidence of 1:3500 LBIs [18]. This disease in general is accompanied by other congenital defects such as, most frequently, the VACTERL sequence (vertebral, anorectal, cardiac and tracheoesophageal MFs and MFs of the radius bone and limbs) [19]. Other congenital MFs of the esophagus that are worth mentioning are esophageal stenosis (most common at the distal esophagus), duplicated esophageal cysts (gastro-intestinal tract duplication with a prevalence of 1:4500 LBIs, characterized by well developed non-striated muscle cover and normally consisting of a communication to the alimentary tract; in esophageal duplications, there is a para-esophageal cyst connected or embedded to the muscle wall [20,21]) and MFs of communicating viscerae, which includes esophageal lung and communicating pulmonary sequestration [22].
Due to the significance of the thorax as a whole and of its component systems specifically, it is easy to realize the need for a more thorough investigation of congenital MFs associated with this portion of the body. In spite of the rare frequency with which these MFs occur, their corresponding morbi-mortality rates are considerable, which propels us to comprehend them and their triggering factors, in deeper details, essentially with the purpose to facilitate early diagnostics and consequently to improve prognostic evaluation. With that in mind, the present study was developed, in which a survey on the ECLAMC database was performed looking for the incidence of such defects in LBIs of ISCMPA.
This is a retrospective case-control study of congenital MFs (designed and performed according to Silveira et al.[23]), organized from an operational regulation which grants an even newborn evaluation, with secondary base data obtained from ISCMPA maternity through ECLAMC database survey forms. The ECLAMC is acknowledged by World Health Organization (WHO) and by International Clearinghouse for Birth Defects Surveillance and Research (ICBDSR) for its role in prevention and investigation of congenital defects and related risk factors.
Case was defined as the newborn with any morphologic anomaly observed at birth. All LBI cases were paired to a control, which was considered as the first LBI with no MFs and of the same sex, born at the same hospital immediately after the newborn bearing a MF. Newborns born outside ISCMPA or weighing less than 500g were excluded from the study.
The databank of the present study includes, for the identification of congenital MFs, all births between January 2004 and December 2006. A number of 259 newborns presenting one or more observable MFs were selected and, consequently, 259 normal newborns were considered as their controls, in a total of 518 LBI. One important observation is that data from October 2005 and 72 random control cases were lost. To correct for this, each MF group was paired to all control cases and the number of births of October 2005 was excluded from calculations.
The assessed variables include weight at birth, gestational age, maternal and paternal age, maternal disease during pregnancy (chronic or acute), parents consanguinity, maternal habits during pregnancy (smoking and use of alcohol, drugs or medications), maternal and paternal academic level and sex of the newborn. Different types of MFs were assessed in the analyzed population; for our study, we selected 30 newborns with MFs in the thoracic region (single or multiple), or, more specifically, in the neck (8 occurrences), chest wall (4) and cardiac (20) and pulmonary (4) systems; they were pooled into the “thoracic MFs group”. We chose to do this pooling based on several aspects: on the related embryological origin of the grouped organs and structures; on the high frequency of observations of multiple and simultaneous MFs in the thoracic region in a certain newborn, which points to related MFs etiology and risk factors; and also on the goal of reaching sufficient sample number to allow proper statistical calculations.
Statistical analyses were performed using the Excel for Windows software, 2003 version. Continuous data were described as lower, higher and median values; categorical data, as percentage. Qui-square and Student T-test were used to compare groups. Odds ratio and 95% confidence interval were estimated. The analyses were considered significant if P < 0.05. The study was submitted to the Ethics Committee in Research (Comite de Etica em Pesquisa, CEP) of our institution and approved under the protocol number 2042/8 and statement 563/08.
According to the performed statistical tests, several variables showed significant difference between the group of malformed newborns (MG) and the control group (CG). For example, we found that the weights of the MG (lower=780g, median=2805g, higher=3840g) were significantly lower than the ones of the CG (lower=990g, median=3115, higher=4600g; P=0,007; Figure 1).
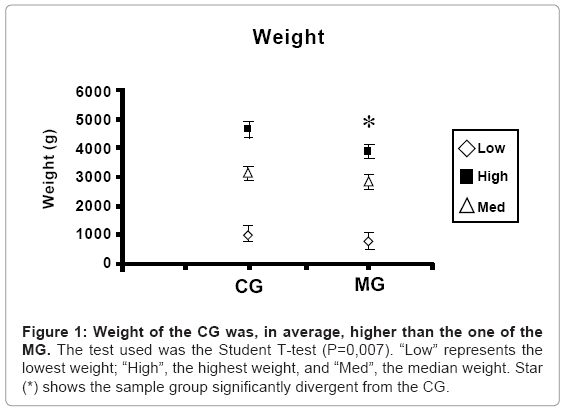
Figure 1: Weight of the CG was, in average, higher than the one of the MG. The test used was the Student T-test (P=0,007). “Low” represents the lowest weight; “High”, the highest weight, and “Med”, the median weight. Star (*) shows the sample group significantly divergent from the CG.
From the data obtained it was also possible to observe significant difference in the number of males and females born in the analyzed groups. In the MG, for example, 40% of the newborns were male, while 60% of them were female; on the other hand, 51% of the newborns of the CG were male and 48% female (P=0,02; Figure 2).
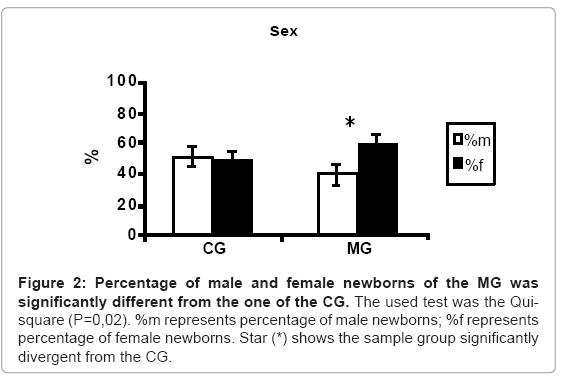
Figure 2: Percentage of male and female newborns of the MG was significantly different from the one of the CG. The used test was the Quisquare (P=0,02). %m represents percentage of male newborns; %f represents percentage of female newborns. Star (*) shows the sample group significantly divergent from the CG.
Gestational age (GA), measured in weeks, also diverged significantly between both groups, being, in general, higher to the CG (lower=20, median=39 and higher=43 weeks) compared to the MG (lower=28, median=37 and higher=41; P=0,002; Figure 3).
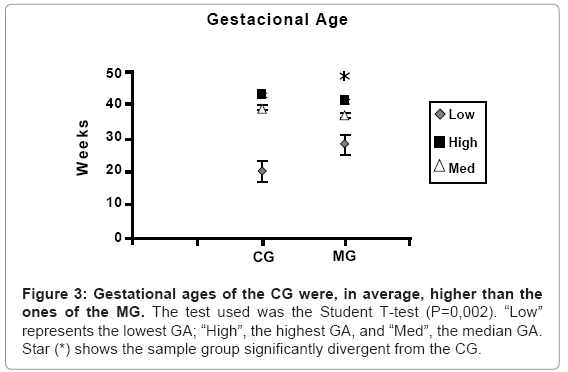
Figure 3: Gestational ages of the CG were, in average, higher than the ones of the MG. The test used was the Student T-test (P=0,002). “Low” represents the lowest GA; “High”, the highest GA, and “Med”, the media
Similarly, paternal age (PA), in years, showed significant variation. It was, in general, lower to the CG (lower=16, median=28, higher=61) than to the MG (lower=20, median=32, higher=80; P=0,042; Figure 4).
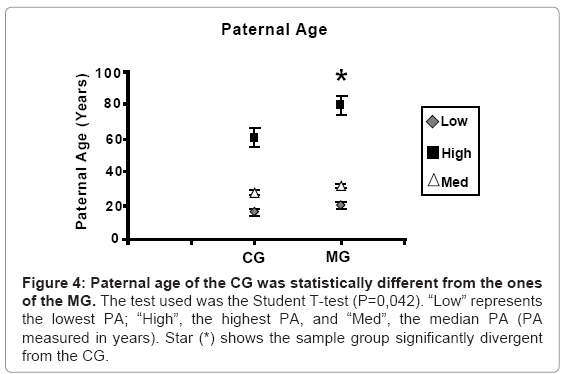
Figure 4: Paternal age of the CG was statistically different from the ones of the MG. The test used was the Student T-test (P=0,042). “Low” represents the lowest PA; “High”, the highest PA, and “Med”, the median PA (PA measured in years). Star (*) shows the sample group significantly divergent from the CG.
Other variables that presented significant difference between the studied groups were smoking and maternal chronic disease during pregnancy. Regarding smoking, 26% of the mothers of the CG declared themselves as smokers, while only 3.4% of the MG mothers did so (P<<0,01; Figure 5). For maternal chronic disease, it was present in 14% of the CG mothers and in 25% of the MG ones (P = 0,004; Figure 6).
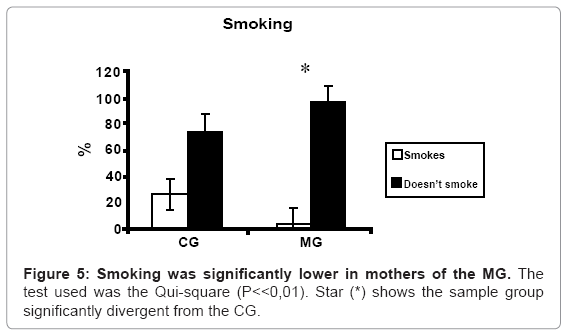
Figure 5: Smoking was significantly lower in mothers of the MG. The test used was the Qui-square (P<<0,01). Star (*) shows the sample group significantly divergent from the CG.
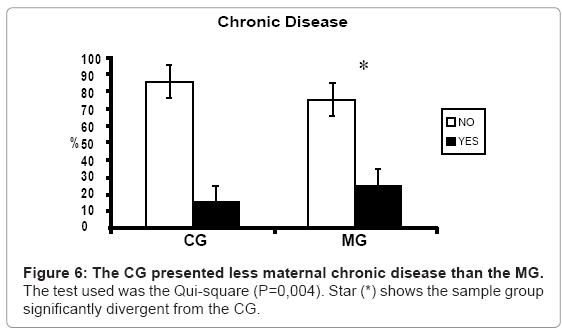
Figure 6: The CG presented less maternal chronic disease than the MG. The test used was the Qui-square (P=0,004). Star (*) shows the sample group significantly divergent from the CG.
Our research showed that, from the 259 malformed newborns found, 30 of them presented thoracic MFs, which included cardiac (20 occurrences), pulmonary (4), chest wall (4) and neck (8) subtypes of MFs, some of them occurring simultaneously in the same newborn. The MFs of the cardiac and chest wall subtypes are formed by pooling even more specific MFs, while MFs of the pulmonary and neck subtypes are not - since, in the latter case, detailed information regarding specifications for these subtypes was not available in the analyzed patient records. The specific MFs described for the subtype cardiac were: anomalies of great vessels, of cardiac chambers and of cardiac valves; the specific MFs described for the subtype chest walls were: pectus carinatum and MFs of ribs. The pooling of specific MFs into subtypes and of subtypes into the general thoracic type, was done for several reasons: i)based on the related embryological spatial, temporal and tissue origin of the grouped organs and structures [1-6]; ii)based on the high frequency of observations of multiple and simultaneous MFs in the thoracic region in a certain newborn [18,19,31], which points to related MFs etiology and risk factors (discussed below); iii)and also based on the goal of reaching sufficient sample number to allow proper statistical calculations. So, statistical analyses were performed using the pool called here “thoracic MFs group”. It is important to remark, however, that the discussion of our results is done based on the subtypes described above (cardiac, pulmonary, chest wall and neck defects) since there are no studies available analyzing a pool such as the “thoracic MFs group” as it was defined here.
From the studied variables, the analysis of the ECLAMC database showed, at first, that LBI with thoracic MFs presented significantly lower weight at birth than LBI of the CG. This observation is supported by several other works, which analyzed the subtypes of MFs and the specific MFs already mentioned. For example, similar observation was performed for newborns with chest wall defects containing mutation in the Dup6p gene [24]; one case of tracheal agenesis and another of tracheal atresia, were described in which newborns had low weight at birth [25,26]; regarding pulmonary MFs, association between bronchoplumonary dysplasia and newborns with extremely low weight at birth [27] was demonstrated; finally, data available also show correlation between extreme low weight newborns and esophageal atresia [28] and, furthermore, a higher incidence of MFs of esophagus was clearly correlated with newborns with weight lower than 2,5Kg at birth [29]. However, newborns with cardiac MFs, in general, show normal weight for their gestational age [30,31], although it is known that 80% of cases of extremely low weight newborns present patent ductus arteriosus [32]. In the case report of Durak et al. it was observed that the newborn with ribs MF presented normal weight for his gestational age [9].
Our work also shows significant difference regarding the sex of newborns between the CG and the MG: in the latter group, there was higher incidence of female LBIs. Existing data regarding this variable is not conclusive. For example, it was shown that chest wall MFs occur predominantly in males [7,8], while, in one case report, the reported chest wall MF was observed in a female LBI [9]. Concerning defects of the upper airways, sex incidence also varies depending on the specific disease; several diseases are more frequent in females (choana atresia, subglotic hemangioma) and many others occur more in males (laringomalacia) [10]. Congenital bronchopulmonary anomalies in general, congenital cystic disease and bronchopulmonary dysplasia, on the other hand, seem to affect more males [11,27,33]. At least one big study demonstrated approximately the same prevalence of cardiac defects in males and females [31] and one population study identified a similar trend for esophageal MFs such as esophageal atresia and tracheo-esophageal fistula [29].
Our analyses also demonstrated that gestational age was significantly different between the CG and the MG, being higher for the first group. This particular observation is strongly supported by other studies. Regarding upper airways MFs, there is a case report of a newborn of 28 weeks with tracheal agenesis [25], many described cases of tracheal atresia in premature newborns [34] and several works showing strong correlation between prematurity and larynx atresia or stenosis [35]. Concerning congenital lung anomalies, the associations between premature newborns and bronchopulmonary dysplasia [27] and between premature newborns and cystic adenomatoid malformation [36], are solidly demonstrated; other studies also report the occurrence of many premature newborns presenting pulmonary sequestration and cystic adenomatoid malformation, although statistical analyses regarding this variable have not yet been done [35]. Esophagus MFs are linked to prematurity as well, as it was demonstrated in the work of Forrester & Mertz, where it was observed a much higher frequency of esophageal MFs in LIBs with gestational age shorter than normal comparing to LIBs with normal gestational age [29]. In the study of Miller et al., on the other hand, it was shown that cardiac MFs occur more often in newborns of normal gestational age [31]; similar situation was described in a case report describing a newborn with ribs MF [9].
From our data, it was still possible to observe that advanced paternal age could have an influence on the generation of thoracic MFs. Accordingly, there is a case report showing that the pulmonary malformation characterized as pulmonary isomerism, which contain diaphragmatic hernia among other important MFs such as renal hipoplasia and midline defects, typical of Wolf-Hirschhorn Syndrome, could be consequence of paternal translocation defects, which could be the result of advanced paternal age [37].
Significant difference was not found between the CG and the MG regarding maternal age (data not shown). Although correlation has been demonstrated between increased maternal age and increased frequency of Down Syndrome [38], this observation does not find parallel in isolated cardiac MFs to the present time [31,39], which supports our own results. The incidence of esophageal MFs, such as esophageal atresia and tracheo-esophageal fistula in LIBs, also has not been correlated with advanced maternal age [29]. Data comparing maternal age and the generation of chest wall anomalies, upper airways and lungs have not been found.
Environmental factors were also shown to be, at least apparently, important to the appearance of thoracic MFs. For example, our analyses demonstrated that newborns of the MG had less smoker mothers than newborns of the CG. This finding, although surprising at first, is at least partly supported by previous studies. Oddsberg et al., for example, did not find any evidence that smoker mothers had increased risk of giving birth to newborns with esophageal atresia [40]. In the case report of Durak et al., the mother of the studied newborn, which showed ribs MF, was not smoker [9]. On the other hand, the work of Lagendijk et al. demonstrated that maternal smoking is a risk factor to the appearance of cardiac MFs [41]. Similarly, there is evidence that maternal smoking increases thickness of airways walls of infants exposed prior to or after birth, which could also have a correlation with increased frequency of Sudden Death Syndrome [42].
Finally, the occurrence of maternal chronic diseases during pregnancy was higher in the MG. The increased risk of appearance of cardiac MFs with presence of maternal chronic disease during pregnancy is supported by the work of Lagendijk et al. [41]. It was found no further data analyzing the correlation between maternal disease and generation of MFs in newborns of the other subtypes of MFs studied here.
None of the other analyzed variables showed significant difference between the MG and the CG.
From the results obtained and from the analyses performed in the present study, we could show that several maternal-paternaldependent variables pose potential risk to the appearance of thoracic MFs in the newborn. These analyses are, in general, merely indicative and absolutely not conclusive, due to sample number limitations. In spite of that, we believe that, from our data, valuable information could be added concerning factors that are interacting with and are deleterious to the embryo or fetus. And, considering that these factors are, very often, perfectly modifiable and that they could be managed of prevented, it is our intention to have contributed to, in the future, the reduction of the incidence of newborns with MFs in the working area of ISCMPA.