Gynecology & Obstetrics
Open Access
ISSN: 2161-0932
ISSN: 2161-0932
Case Report - (2017) Volume 7, Issue 10
Gestational hypertensive diseases, including preeclampsia, are frequently associated to a poor prognosis when they are severe, with maternal or fetal death, and especially in low resource settings. Early recognition of severity signs can help to prevent maternal and/or fetal complications. Aside classically described signs, some others, such as vulvar edema, have been put in light through case reports and case series. Here we describe the case of a Cameroonian pregnant woman, who presented severe preeclampsia with massive vulvar edema.
Keywords: Vulvar edema; Severe preeclampsia; Intrauterine death
According to the World Health Organization in 2014, hypertensive disorders were after hemorrhage, the leading cause of maternal death, responsible of near 14% of maternal mortality [1,2]. The burden is more pronounced in low resource settings including sub-Saharan African areas, and one of the most important factors are delayed diagnosis of severity and/or management [2].
Thus, preeclampsia and eclampsia as well as other potentially dangerous pregnancy related disorders should be recognized early and managed adequately to avoid tremendously huge complications [2,3]. Otherwise, even though their severity is broadly defined by highly elevated blood pressure, proteinuria, and seizures, some other signs, such as ascites and vulvar edema, are encountered in severe preeclampsia and eclampsia [3]. Here we report the case of a Cameroonian pregnant woman, who presented severe preeclampsia with massive vulvar edema.
A 19 years old woman G1P0with a non-contributive past medical history and not followed pregnancy was referred at 32 weeks and 5 days for a voluminous vulvar edema. Two weeks prior to consultation, she noticed a progressive soft and painless vulvar tumefaction gradually hindering with daily activities without other signs. She consulted in a health center from where she was referred. On admission, she was conscious and ill looking, with a blood pressure of 160/120 mm Hg. She had pallor, signs of ascites, and no fetal heart sounds. The genital examination revealed a massive translucent vulvar edema limiting access to the vagina (Figures 1 and 2).
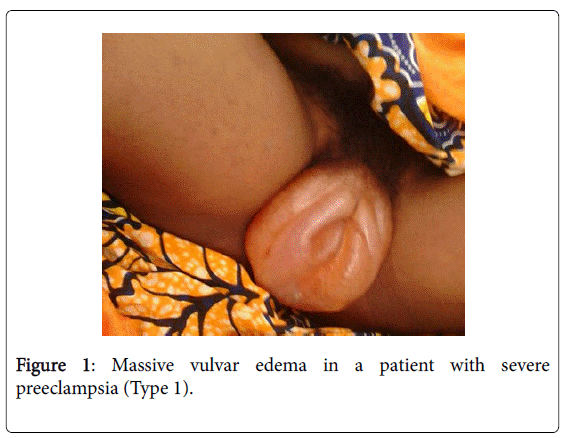
Figure 1: Massive vulvar edema in a patient with severe preeclampsia (Type 1).
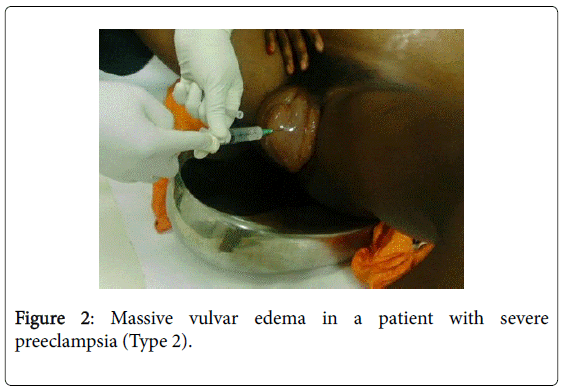
Figure 2: Massive vulvar edema in a patient with severe preeclampsia (Type 2).
She had a proteinuria (3.4 g/ 24 h) without other biological abnormalities. Abdominal ultrasound confirmed intrauterine death with massive ascites. We thought of a severe preeclampsia complicated by ascites, massive vulvar edema and fetal demise. An emergency caesarean section was done after primary care including local evacuation and aspiration of the vulvar edema. She also received IV magnesium sulfate and IV nicardipine. Surgical findings were an 1800g recently dead female fetus and 4 liters of clear ascitic fluid. The blood pressure returned to normal after 2 weeks as well as vulvar edema which regressed completely after 3 weeks.
Vulvar edema is a scarcely described sign in literature treating of gestational hypertensive disorders, but in the few reported cases, it’s found to be related to a bad prognosis [3,4]. Indeed, Morris et al. described two cases of massive antepartum vulvar edema in patients with preeclampsia which also failed to be managed with medication due to fetal distress, and thus needed a caesarean section [5]. More recently, Ngowa et al. reported a case of massive vulvar edema in a 20 years old primigravida woman with severe preeclampsia at 32 weeks gestation, which also led to a caesarian section due to acute fetal distress [4].
Possible mechanisms surrounding the presence of vulvar edema in pregnant women with hypertension, with (as in our case) or without ascites, are mainly represents by increased vascular permeability with low albumin plasma levels [5,6,7]. Indeed, hypoalbuminemia is a common manifestation in pregnancy induced hypertension and occurs mainly due to systemic small size vessel spasm, activation of rennin secreting cells with later increased secretion of angiotensin and damaged and increased permeability of vascular endothelial cells, thereby leading to a large number of other proteins and liquid leaking in tissue clearance resulting in intravascular dehydration [4,8]. As precedents observations in literature, we make the hypothesis of an association between vulvar edema with severe outcomes of gestational hypertensive disorders.
Our report aims to draw clinician’s attention on the prognostic role of vulvar edema in patients with preeclampsia. Nevertheless, a greater evaluation including a considerable sample of hypertensive pregnant women, should be done to either confirm or not, association between vulvar edema and severe outcomes.
Dr Alexandra Elanga.