Medical & Surgical Urology
Open Access
ISSN: 2168-9857
ISSN: 2168-9857
Case Report - (2018) Volume 7, Issue 3
Keywords: Renal stone; Steinstrasse; SWL; Renal tubular acidosis
Steinstrasse, the term was coined by Egbert Schmiedt and Christian Chaussy, the German pioneers of SWL in the 1980s. It refers to complication of SWL for treatment of renal stones whereby smaller stone fragments from kidney get lodged in ureter. Most of the stone fragments are small, transient and clear spontaneously. The stone fragments, at times become static, causing partial or complete obstruction and may require intervention. Spontaneous steinstrasse is rare phenomenon. Few cases of renal tubular acidosis with spontaneous steinstrasse have been reported. Symptomatic patients require prompt treatment as it may lead to loss of renal function. We discuss a 21 year male with large spontaneous steinstrasse with bilateral renal stones, its aetiology and management.
A 21 year male presented in our Emergency department with complaints of acute onset left flank pain. Past history was insignificant. Patient was afebrile and general physical and systemic examination was grossly normal. Pain was relieved with intravenous analgesics. On evaluation, kidney, ureter and bladder ultrasound showed bilateral renal stones with left renal hydronephrosis. Further, kidney, ureter and bladder X-ray revealed bilateral radio opaque stones in renal fossa and multiple left ureteric stones appearing as steinstrasse (Figure 1). On evaluation, routine haematology was normal and serum urea and creatinine were 38 mg/dl and 2.8 mg/dl respectively.
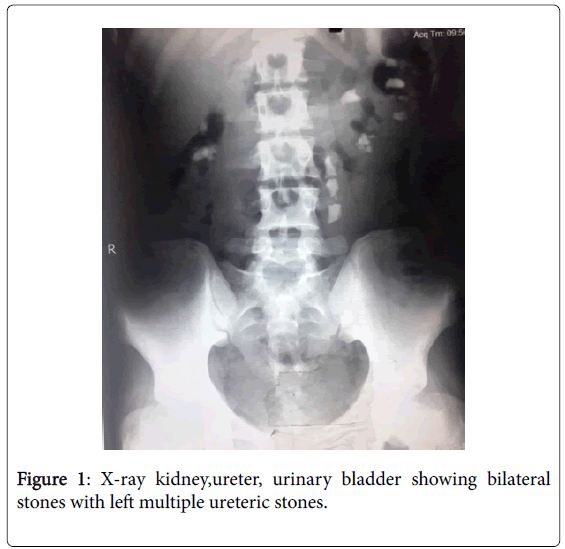
Figure 1: X-ray kidney,ureter, urinary bladder showing bilateral stones with left multiple ureteric stones.
Urine routine examination revealed 7-8 pus cells, 2-3 red blood cells and no amorphous deposits or crystals. In view of obstructive uropathy with raised creatinine, bilateral Double J stent was placed under antibiotic cover (Figure 2). Patient was pain free and discharged with a follow-up at week time. The serum urea and creatinine were 21 mg/dl and 1.1 mg/dl respectively.
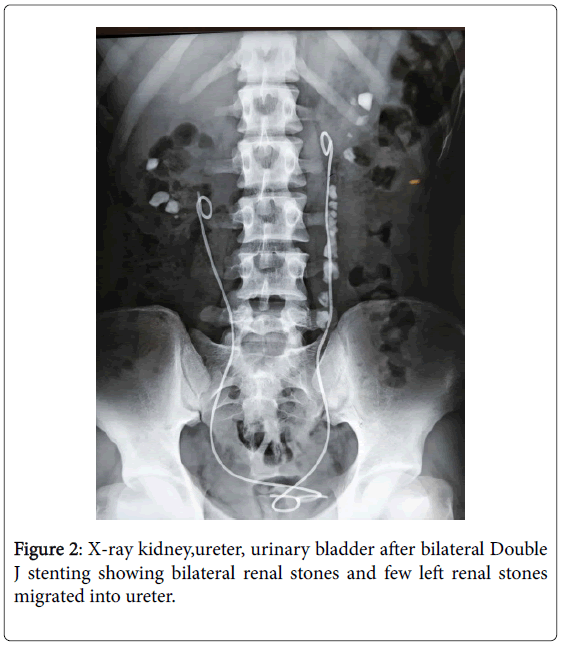
Figure 2: X-ray kidney,ureter, urinary bladder after bilateral Double J stenting showing bilateral renal stones and few left renal stones migrated into ureter.
The metabolic evaluation revealed that Urine pH was 6.5, 24 hour urinary creatinine was 1248 mg, calcium was 156 mg, citrate was 310 mg, uric acid was 480 mg and volume was 3200 ml. Serum calcium was 9.1 mg/dl, uric acid was 6.2 mg/dl and electrolytes were grossly normal. Urine culture showed no growth and differential leukocyte counts were within normal range. Intravenous pyelogram was done prior to planned surgery and it showed bilateral functioning kidneys. Patient underwent staged surgery; left ureterolithotomy via open flank approach was performed under general anaesthesia. The ureter was identified and dissected all around. Dense adhesions were present probably due to inflammation secondary to stones. Ureter was incised and all stone fragments were removed. Post-operative X-ray showed bilateral renal stone with Double J stent in situ (Figure 3).
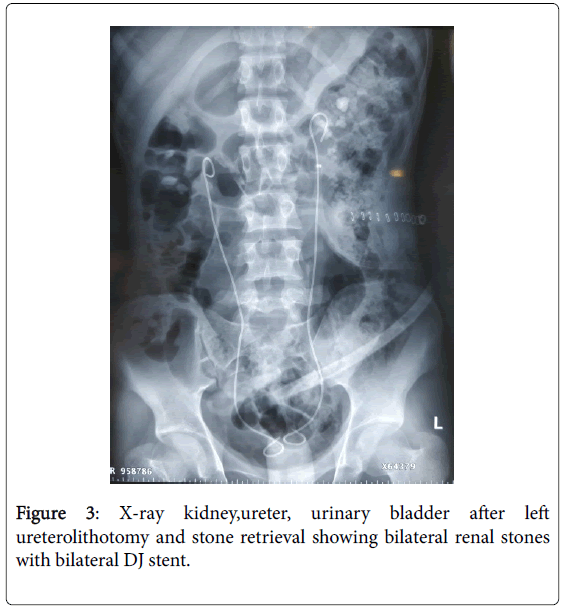
Figure 3: X-ray kidney,ureter, urinary bladder after left ureterolithotomy and stone retrieval showing bilateral renal stones with bilateral DJ stent.
2 weeks later patient was readmitted and left followed by right PCNL was done via standard approach and complete stone clearance achieved (Figure 4). Post-operative recovery was uneventful and patient was discharged on day 3.
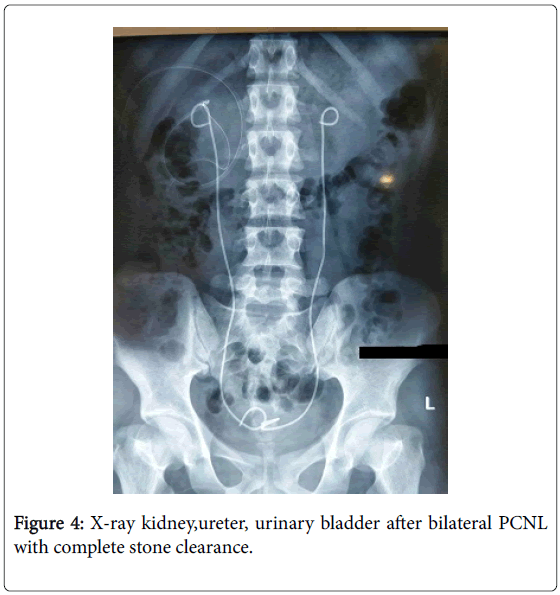
Figure 4: X-ray kidney,ureter, urinary bladder after bilateral PCNL with complete stone clearance.
Stone analysis showed 100% calcium phosphate stones. At 6 weeks, patient had unremarkable outpatient follow up and bilateral Double J stent were removed with flexible cystoscopy. 6 months follow up; patient is stone free and doing well.
Steinstrasse is aggregation of stones in the ureter seen commonly following extracorporeal SWL for renal stones. It is reported as high as in 15 % of cases after SWL in some series [1]. The clinical presentation of steinstrasse can be that of renal colic or may be silent and can lead to loss of renal function. Pandey et al. [2] reported a case of multiple ureteric stone with renal stone and non-functional kidney managed with nephroureterectomy [2]. Steinstrasse are usually small, transient and flush out instinctively. Large steinstrasse is defined as aggregation of stones occupying more than one third of ureter and is very uncommon [3]. Steinstrasse in absence of SWL is very rarely reported. Few cases of spontaneous steinstrasse in association with renal tubular acidosis and nephrocalcinosis have been reported [4,5]. The stone formation in case of renal tubular acidosis is likely due to hypercalciuria and hypocitrauria causing supersauration and stone formation. The index case was also worked up, however showed no metabolic abnormality. The reason postulated behind stone formation in the index case could be due to dietary reasons, less water intake and environmental factors. Nevertheless, metabolic work up should be done in such cases to prevent recurrence of stone formation and treat accordingly.
Patients typically present with renal colic if it’s obstructing the ureter and complaints of pain, nausea and vomiting. Initially conservative therapy in the form of medical expulsive treatment can be tried, however in case of persistent symptoms and obstruction, other options should be considered like endoscopic manipulations, percutaneous nephrostomy and rarely open surgery when burden is very high and previous therapy has failed [6,7]. In the index case, patient had massive stone burden in the ureter and after explaining the options to the patient, ureterolithotomy via open approach was performed and later percutaneous nephrolithotomy was done on bilateral kidneys one at a time.
Large spontaneous steinstrasse is rare. It can be insidious in presentation and yet have significant patient impact in terms of renal function and infection. Prompt treatment is essential to prevent permanent loss of renal function. We report this unusual case of large spontaneous steinstrasse with no metabolic abnormality and discuss the management.