Advanced Techniques in Biology & Medicine
Open Access
ISSN: 2379-1764
ISSN: 2379-1764
Research Article - (2016) Volume 4, Issue 1
Introduction: Biliary stricture can occur following surgeries of the biliary tract and can cause biliary congestion and cholangitis. Recently, fully covered self-expandable metal stent (FCSEMS) has been utilized for postoperative hilar and anastomotic strictures that have conventionally been considered difficult to treat. On the other hand, there is no solid evidence regarding optimal metal stent placement period.
Method: Retrospective review of patients treated for postoperative benign biliary stricture using a FCSEMS at our hospital between 2013 and 2015.
Results: We performed a total of 14 metal stent placements for 12 patients with postoperative benign biliary stricture. In all the patients, the metal stents were placed endoscopically and removed safely after the placement. The mean duration of stent placement was 47.9 days (28-144), and there was no retrograde cholangitis observed during metal stent placement. Following metal stent removal, the stricture improved in 9 patients. Recurrence developed in 3 patients, recurring bile duct stones in 2 patients, and cholangitis in 1 patient. Adverse events included post-ERCP pancreatitis in 2 patients, which was alleviated by stent removal the following day and conservative treatment in 1 patient, and conservative treatment only in the other patient. Distal stent migration was observed in 2 patients.
Conclusion: The present results suggest that stricture improvement can be expected in a shorter period by metal stent placement in patients with refractory postoperative biliary stricture. In patients with bile duct stones, lithectomy can be safely and effectively performed following metal stent expansion; however, further studies are required.
Keywords: Benign biliary stricture, BBS, Fully covered selfexpanding metal stent
Although rare, biliary stricture can occur following laparoscopic cholecystectomy and other surgeries of the biliary tract, and can cause biliary congestion, abdominal pain, and cholangitis. If left untreated, this condition can progress into secondary biliary cirrhosis, and therefore adequate management is important. Endoscopic placement of multiple plastic stents is considered effective for improve the stricture, and has thus gained widespread popularity [1,2]. However, plastic stents need to be replaced every 3 months, and multiple stents need to be placed in a single operation, complicating the procedure. Therefore, we often encounter patients whose cases are difficult to treat. Metal stents are durable and may be implanted for long periods without requiring replacement, and the expansion with 1 stent generates results equal or superior to multiple plastic stents. The recently developed fully covered self-expandable metal stent (FCSEMS) has been utilized for benign biliary stricture as it can be endoscopically removed safely, and the effectiveness of which has been reported [3-7]. However, there is no solid evidence regarding optimal metal stent placement period in the treatment of benign biliary stricture. On the other hand, advancements of metal stents have enabled stricture improvement in hilar and anastomotic strictures that have conventionally been considered difficult to treat by selecting the most suitable stent for the condition. This study is aimed to evaluate the usefulness of FCSEMS placement in patients with postoperative hilar and anastomotic strictures.
Patients
We retrospectively examined patients treated for postoperative benign biliary stricture using a metal stent at our hospital between 2013 and 2015. At our institution, metal stents are used for postoperative biliary stricture in the following cases: (1) patients a) with a history of biliary surgery, which has a clear causal relationship with the site of biliary stricture, or b) in whom malignant biliary stricture has not been histologically detected; (2) patients who developed cholangitis or abdominal pain due to biliary stricture that required frequent endoscopic or percutaneous biliary drainage, which decreased their quality of life; (3) patients with biliojejunal anastomotic stricture that was refractory to balloon dilatation. Informed consent was obtained from all patients prior to the endoscopic procedure.
Details of endoscopic procedures
The endoscopic procedures were performed in all patients under deep sedation. We used TJF-260V (Olympus Medical Systems, Japan) for duodenoscopy and either the prototype SIF-Y-0004 or SIF-Y-0015 (Olympus Medical Systems, Japan) for endoscopy for postoperative intestinal reconstruction cases. A practitioner well experienced in endoscopic retrograde cholangiopancreatography (ERCP)-related surgeries (>300 operations/year) was responsible for all cases. In all the cases, extractable metal stents (FCSEMS) were employed. In patients with duodenal papilla, metal stent placement was performed under wire guidance following an adequate endoscopic sphincterotomy (ES). In the event that ES had already been made, an additional incision was made to avoid post-ERCP pancreatitis and to widen openings judged insufficient to match the metal stent diameter. The placed stent would ultimately be removed in all cases using forceps or a snare via the forceps channel by holding the lower end of the stent.
Follow-up and definitions
As a general rule, metal stents were removed approximately 1 month after placement. Cholangiography was initially performed upon stent removal to assess any immediate improvement of the stricture after the treatment. Approximately 6 months after stent removal, follow-up observation was performed by CT or MRI to assess the status of the stricture site. Furthermore, evaluations were performed during the 6 months following surgery to determine whether or not there is any abnormality in liver function, or if a recurrence such as cholangitis requires endoscopic treatment.
Clinical success was determined when a comparison of images of the bile duct taken prior to the placement and upon removal of the metal stent showed that 1) the stricture has disappeared or improved, 2) no symptoms appear after stent removal, 3) there are no abnormal liver function findings, and 4) additional endoscopic treatment is not required. Furthermore, relapse was defined as the need for additional endoscopic treatment for the appearance of symptoms and abnormal liver function. Complications including pancreatitis following ERCP and stent migration were recorded separately.
In the present study, we performed a total of 14 metal stent placements for 12 patients with postoperative benign biliary stricture. In all the patients, the metal stents were placed endoscopically and removed safely after the placement. The surgical procedure that caused biliary stricture was hepatectomy in 1 patient, laparoscopic cholecystectomy in 6 patients, laparotomic cholecystectomy in 2 patients, pancreaticoduodenectomy in 2 patients, and extrahepatic bile duct resection in 1 patient. The stricture site was the left hepatic duct in 1 patient, the right hepatic duct in 2 patients, the superior bile duct in 6 patients, and the site of biliojejunal anastomosis in 3 patients. The mean duration of stent placement was 47.9 days (28-144), and there was no retrograde cholangitis observed during metal stent placement. Among these patients, bile duct stones were observed in 4 patients. In all these patients, the stones could be removed following biliary expansion with the metal stent (Figure 1).
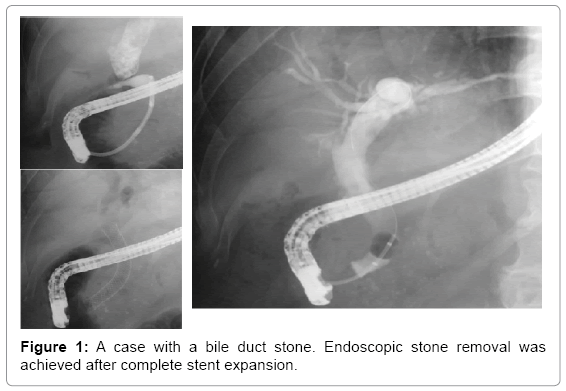
Figure 1: A case with a bile duct stone. Endoscopic stone removal was achieved after complete stent expansion.
Adverse events included post-ERCP pancreatitis in 2 patients, which was alleviated by stent removal the following day and conservative treatment in 1 patient, and conservative treatment only in the other patient. Distal stent migration was observed in 2 patients.
Following metal stent removal, the stricture improved, together with an improvement in the symptoms and abnormal liver function in 9 patients. Recurrence developed in 3 patients, recurring bile duct stones in 2 patients, and cholangitis in 1 patient. Among these patients, 1 patient underwent treatment with a metal stent for a total of 3 times. After the initial metal stent placement, the bile duct stone was removed followed by the metal stent. Five months later, the patient developed recurrent bile duct stones and recurrent stricture. Repeat surgery was performed to remove the bile duct stones, and a metal stent was placed in the stricture site; however, pancreatitis developed, and the stent was removed the following day. Four months later, a recurrent bile duct stone developed again, and following lithotomy a Nagi™ stent (Taewoong Medical Co., Ltd., Gyeonggi-do, Korea) was placed in the upper bile duct in the form of an inside stent. Six months later, distal migration of the Nagi™ stent occurred; however, cholangiographic images showed improvement of the stricture (Figure 2).
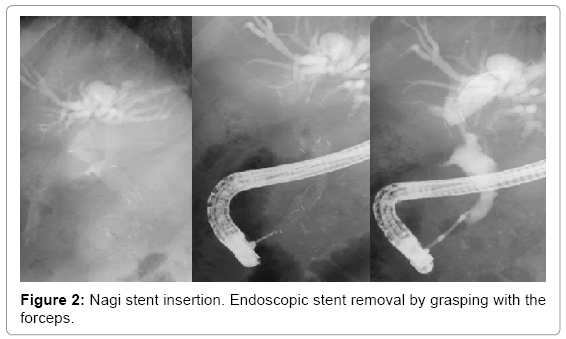
Figure 2: Nagi stent insertion. Endoscopic stent removal by grasping with the forceps.
Benign biliary stricture can lead to biliary congestion and bile duct infection, and can cause secondary biliary cirrhosis, which requires aggressive treatment, if left untreated.
In the treatment of bile duct stones and cholangitis, minimally invasive laparoscopic cholecystectomy has been established. However, misperception of the anatomical positional relationship when observing by laparoscopy has increased the incidence of bile duct injury during surgery and postoperative stricture [8,9]. Of benign biliary strictures, postoperative biliary stricture has abundant fibrous tissue in the stricture site. This, along with bile duct flexure and deviation, complicates treatment in some cases, whereas other cases are refractory to treatment (Table 1).
| M/F | Age | Operation | Bile duct stone | Location of stricture | Bismuth classification | Metal stents | Duration of FCSEMS insertion, day | Residual stricture on stent removal | Endoscopic lithotripsy | Adverse event | Outcome | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | M | 48 | LAP-CCY | - | Bs | II | Niti-S 6 × 120 mm ×2 | 119 | - | Success | ||
| 2 | F | 43 | CCY | - | Bs | I | HANARO stent8 × 100 mm | 35 | - | Distal migration | Success | |
| 3 | F | 55 | LAP-CCY | - | Br | I | Wallflex10 × 80 mm | 35 | + | Success | ||
| 4 | M | 64 | CCY | + | Bs | I | Wallflex10 × 80 mm | 34 | - | Available | Stone recurrence | |
| Supremo-1212 x 80 mm | 1 | - | Pancreatitis | |||||||||
| Nagi stent 16 × 30 mm | 182 | - | Available | Distal migration | ||||||||
| 5 | F | 67 | Liver lobectomy | + | Br | IIIa | Niti-S8 × 120 mm | 38 | - | Available | Stone recurrence | |
| 6 | F | 13 | Choledochojejunostomy | - | Biliary-enteric anastomotic site | - | Wallflex10 × 60 mm | 65 | - | Success | ||
| 7 | F | 54 | LAP-CCY | - | Bs | I | Wallflex10 × 80 mm | 35 | - | Pancreatitis,Abdominal pain | Success | |
| 8 | M | 77 | PD | - | Biliary-enteric anastomotic site | - | Wallflex 10 × 40 mm | - | Cholangitis recurrence | |||
| 9 | M | 78 | LAP-CCY | + | Bl | IIIb | Niti-S 6 × 120 mm + PS | 28 | - | Available | Success | |
| 10 | F | 83 | LAP-CCY | + | Bs | I | Wallflex 10 × 60 mm | 35 | - | Available | Success | |
| 11 | F | 51 | LAP-CCY | - | Bs | II | Niti-S 6 × 100 mm + PS | 54 | - | Success | ||
| 12 | F | 62 | PD | - | Biliary-enteric anastomotic site | - | Wallflex 10 × 40 mm | 49 | - | Success | ||
| LAP-CCY, Laparoscopic Cholecystectomy; CCY, Cholecystectomy (Open Surgery); PD, Pancreatoduodenectomy; PS, Plastic Stent | ||||||||||||
Table 1: Characteristics of the patients.
In the treatment of biliary stricture, good outcomes have been obtained by placing multiple plastic stents endoscopically [1,2], allowing minimally invasive endoscopic treatment to gain greater popularity than surgery. Furthermore, reports of the therapeutic outcomes of using covered metal stents to obtain better results have suggested the effectiveness of such treatment [3-7]. On the other hand, with uncovered metal stents, hyperplastic changes of the biliary epithelium can cause the stent to become embedded in the bile duct wall, making it impossible to remove, and thus the use of such stents should be avoided. The advantages of using metal stents include the ability to achieve large dilatation in a single step and the fewer times the procedures are required because metal stents can be implanted for a longer period than plastic stents. In a prospective study of benign biliary stricture caused by chronic pancreatitis, the improvement of the stricture with metal stents was comparable to that with plastic stents. However, the study suggested that patient burden was reduced because of the fewer times the patient has to undergo the procedures [10]. Furthermore, in patients with bile duct stones, once the implanted metal stent has fully expanded, the stone can be removed while the metal stent is implanted, making it a powerful therapeutic option. Of the patients with bile duct stones in our series, we were able to remove the stones entirely in all the patients. The optimal duration of covered metal stent placement varies from 3 to 12 months depending on the report, and remains controversial. Nonetheless, in the event of longterm placement, retrograde cholangitis is observed relatively often, and there are not always cases in which the metal stent could be removed. Situations recuiring surgery for metal stent removal must be absolutely avoided, and it is important that all patients must be stent-free following treatment. Although the duration of stent placement should be as short as possible, the set period of 1 month is considered short. In the event of stricture at the first branch of the hepatic duct, provided the metal stent is temporarily placed for a short time, placing plastic stents sideby- side (SBS) in the biliary duct without stricture will prevent biliary obstruction in the portion without stricture. Considering the combined use of plastic stents, if we could prove that satisfactory long-term improvements can be anticipated with metal stent placement for 3 to 6 months, management should be achieved with greater safety.
In the endoscopic management of malignant biliary stricture, various stents have been developed to date [11] following the demonstration of the effectiveness of covered metal stents [12]. Furthermore, although interventional endoscopic ultrasound is being established for the treatment of walled-off pancreatic necrosis (WOPN), metal stents that are best suited for therapeutic procedures with greater safety and effectiveness have become available [13,14]. However, results obtained by metal stenting remain limited to benign biliary stricture. At present, stenting is used for malignant biliary stricture with regard to refractory cases, and the best strategies are chosen according to the condition. We have used various types of stents, and although we have treated cases in which the present treatment was considered to be well indicated, we have also experienced errors. In the event of stent placement for biliary stricture in the hepatic portal region, although conventional metal stenting was difficult, the reported treatment methods include stent placement in the left and right hepatic ducts using a coarse-meshed uncovered stent with [15], and the SBS method with the metal stents placed parallel in the left and right hepatic ducts [16]. In cases with stricture in the hepatic portal region, we performed stent placement using the SBS method with a covered metal stent, and we were able to remove the stent safely and improve the stricture (Figure 3). In the present study, we observed post-ERCP pancreatitis in 2 out of the 12 patients. In 1 patient of these patients who developed recurrence, pancreatitis following ERCP was not observed with the 10 mm WallFlex® stent (Boston Scientific Japan) that was initially placed; however, pancreatitis developed upon the second procedure with the placement of a 12 mm SUPREMO®-12stent (Taewoong Medical). The conditions were considered to be approximately the same with the exception of stent diameter, which suggested that using a stent with a larger diameter created pressure displacing the pancreatic duct lumen, which could have been a causative factor of the pancreatitis. This could be attributed to the fact that common image findings among patients who developed pancreatitis revealed that after metal stent placement, a notch formation was found at the papilla, with incomplete stent expansion. In patients with biliary stricture and narrow extrahepatic bile duct following cholecystectomy, we believe that caution should be exercised such as using a metal stent with a relatively narrow inner diameter. To ensure metal stent expansion and avoid postoperative pancreatitis, we placed a Nagi™ stent in an entirely inside stent manner. The Nagi™ stent is generally used when performing EUS-guided drainage for WOPN and pancreatic pseudocysts [14]. For the stent characteristics, 1) it has an inner diameter of 16 mm and a short length, 2) it has a relatively weak radial force, and 3) it can be removed from the forceps channel by holding with forceps. For the case concerned, we used this type of stent considering that the bile duct before and after the stricture site was adequately expanded. Distal migration occurred as a result; however, the degree of biliary stricture improved without recurring pancreatitis. Following treatment, the stent was safely removed using forceps, and the patient progressed without recurrence.
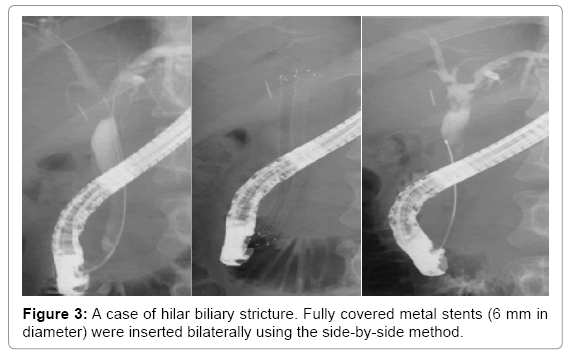
Figure 3: A case of hilar biliary stricture. Fully covered metal stents (6 mm in diameter) were inserted bilaterally using the side-by-side method.
At our institution, we treat postoperative intestine reconstruction patients using short-type single-balloon enteroscopy. This has enabled the use of a normal ERCP device [17], and a metal stent delivery system can be used similarly to duodenoscopy. Thus, an aggressive approach using a metal stent can also be effective for anastomotic stricture. The biliojejunal anastomosis area can be near the hepatic portal, and metal stent placement must be exercised with caution to prevent the stent from obstructing the intrahepatic bile duct.
Taken together, the use of various metal stents has facilitated treatment, even in patients with postoperative biliary stricture who are difficult to treat. However, the present series is a retrospective study, and the effectiveness of metal stents should be established in prospective studies of patients with postoperative biliary stricture. The methodology of the endoscopic technique also needs to be established.
In conclusion, the present results suggest that stricture improvement can be expected in a shorter period by metal stent placement in patients with refractory postoperative biliary stricture. In patients with bile duct stones, lithectomy can be safely and effectively performed following metal stent expansion; however, further studies are required.