Biochemistry & Pharmacology: Open Access
Open Access
ISSN: 2167-0501
ISSN: 2167-0501
Research Article - (2014) Volume 3, Issue 3
Rheumatoid Arthritis (RA) is an autoimmune disease characterized by chronic synovial inflammation and disability.
The most widely used Disease-Modifying Antirheumatic Drug (DMARD) is methotrexate and it continues to be the gold
standard. However, the use of high-dose methotrexate is associated with severe adverse effects. Iguratimod, which is
currently used in clinics in China and Japan, is a novel oral DMARD for the treatment of RA. In this study, the effect
of combination of methotrexate and iguratimod on murine Collagen-Induced Arthritis (CIA) and its mechanism was
determined. Oral administration of iguratimod (3 mg/kg, 10 mg/kg) combined with methotrexate (1 mg/kg) potently
blocked CIA development and delayed its progression, which was stronger than iguratimod or methotrexate used alone.
Furthermore, infiltration of inflammatory cells into the synovium was remarkably inhibited by combination therapy and
importantly, no bone erosion and joint destructions were observed in combination therapy group. In addition, combined
administration of these two DMARDs suppressed production of cytokines (IL-17, IFN-γ, IL-6 and TNF-α) and antibodies
(IgG and IgG2b) in serum, as well as humoral and cellular responses in CIA mice. Consistent with its effects in vivo,
iguratimod combined with methotrexate significantly suppressed T and B cells responses in vitro. Taken together, our
findings suggest that combination treatment with iguratimod and methotrexate should be an intriguing and preferable
therapeutic strategy for treating RA.
Keywords: Iguratimod; Methotrexate; Rheumatoid arthritis; Collagen-induced arthritis; Combination therapy
Rheumatoid Arthritis (RA) is a chronic systemic autoimmune disease with unclear etiology [1-4]. It is characterized by severe persistent synovitis that leads to the destruction of cartilage and bone, autoantibody production, and systemic inflammation [5,6]. Various cytokines, chemokines, effector cells, such as T- and B-lymphocytes, monocytes/ macrophages, dendritic cells, Fibroblast - Like Synoviocytes (FLSs) and osteoclasts are involved in RA [7-11]. The therapeutic strategy of RA has undergone revolutionary changes [12,13]. Current drug therapies include two principal approaches: conventional Non- Steroidal Anti-Inflammatory Drugs (NSAIDs) and Disease-Modifying Antirheumatic Drugs (DMARDs) [14-16]. NSAIDs are only effective for controlling the symptoms of RA, such as pain, inflammatory, and stiffness, and the long-term disease progression can not be prevented by them [17]. However, unlike NSAIDs, DMARDs can not only improve symptoms but also interfere with the disease process [18,19]. DMARDs include methotrexate, sulfasalazine, hydroxychloroquine, and leflunomide. Recently, biological agents were introduced [17]. These biological-response modifiers include infliximab (inhibitor of TNF-α), anakinra (inhibitor of IL-1), abatacept (costimulation blocker), rituximab (anti-CD20 monoclonal antibody) and so on. However, its widespread use was limited by the high cost.
Methotrexate, a folic acid antagonist, has been the most widely used small molecular DMARD in the treatment of RA. It has been demonstrated effectiveness, high tolerability and low cost [17,20]. Methotrexate acts mainly on inhibiting the proliferation of rapidly dividing lymphocytes and other inflammatory cells [21]. Furthermore, methotrexate may diminish synovial collagenase gene expression [22], reduce toxic oxygen metabolites [23] and increase extracellular adenosine levels [24,25]. However, use of methotrexate has been limited by some toxicity problems, such as hepatitis, cirrhosis, cytopenias and interstitial pneumonitis [26]. Because the adverse effects are dose dependent, methotrextate usually started in combination with other DMARDs in current management of RA. Iguratimod is an immunomodulatory compound and has been developed as a DMARD [27]. Our previous research had identified its unique antiarthritic mechanism which is different from the classical DMARDs. Iguratimod could block the IL-17 pathway in FLSs and then effectively treat CIA [28]. In the present study, we examined the effect of combination of iguratimod and methotrexate in a murine CIA model, and elucidated the possible mechanism.
Mice
Male DBA/1 mice were purchased from the Shanghai Experimental Animal Center, the Chinese Academy of Sciences. Mice used in CIA model were 7-8 weeks of age. Animal welfare and experimental procedures were carried out strictly in accordance with the Guide for the Care and Use of Laboratory Animals (National Institutes of Health, the United States) and the related ethical regulations of our university. All efforts were made to minimize animals’ suffering and to reduce the number of animals used.
Chemicals and reagents
Iguratimod was provided by Simcere Pharmaceutical (Nanjing, China) with purity more than 99%. Methotrexate, concanavalin A (Con A), lipopolysaccharide (LPS) and 3-(4, 5-dimethyl-2-thiazyl)-2, 5-diphenyl-2H-tetrazolium bromide (MTT) were purchased from Sigma-Aldrich (St. Louis, MO). Bovine type II collagen (CII) was purchased from Chondrex (Seattle, WA). ELISA kits for IL-17 and IFN-γ were purchased from Dakewe Biotech Co. Ltd (Shenzhen, China). Cytometric Bead Array (CBA) cytokine assay kit was purchased from BD Biosciences (San Jose, CA). All other chemicals were purchased from Sigma-Aldrich (St. Louis, MO).
Induction and assessment of CIA and drugs administration
Male DBA/1 mice (eight mice per group) were immunized on day 0 with an intradermal injection at the base of the tail of 100 μg bovine type II collagen (CII; Chondrex) emulsified in complete Freund’s adjuvant (Chondrex). On day 21, mice were boosted by injection of 100 μg CII dissolved in incomplete Freund’s adjuvant (Sigma). Mice were examined daily and scored for arthritis severity, with each paw assigned a clinical score as follows: 0, normal; 1, erythema and mild swelling confined to the ankle joint and toes; 2, erythema and mild swelling extending from the ankle to the midfoot; 3, erythema and severe swelling extending from the ankle to the metatarsal joints; 4, enclosing deformity with joint swelling. Hind paw thickness was measured with electronic plethysmometer (Paw Volume Meter).
For treatment, iguratimod and methotrexate were administered i.g. beginning on the day after the booster injection (day 22). The mice were randomly divided into 7 groups: Group 1, normal DBA/1J mice; Group 2, CIA mice with vehicle; Group 3, CIA mice with iguratimod, 3 mg/kg once a day; Group 4, CIA mice with iguratimod, 10 mg/kg once a day; Group 5, CIA mice with methotrexate, 1 mg/kg once every two days; Group 6, CIA mice with iguratimod plus methotrexate, iguratimod 3 mg/kg once a day, methotrexate 1 mg/kg once every two days; Group 7, CIA mice with iguratimod plus methotrexate, iguratimod 10 mg/kg once a day, methotrexate 1 mg/kg once every two days.
Radiographic assessment
At the end of the experiments, the mice were anesthetized and radiographs of the hind paws were obtained with a lumina XR system (Caliper IVIS Spectrum). Radiographic scoring criteria of each paw were assessed on the following scale: 0 = no bone damage, 1 = joint erosion and 2 = bone erosion and osteophyte formation.
Histopathology
Paws for histological analysis were removed from mice and immediately fixed in 4% paraformaldehyde. The paws were decalcified in EDTA, embedded in paraffin, sectioned, and stained with H&E. The sections were scored to assess joints inflammation on a scale of 0-4 under blinded conditions, according to the degree of hyperplasia in the synovial lining, mononuclear cell infiltration, and pannus formation. The maximum possible score per mouse was 8.
Quantitative real-time PCR
Total RNA was extracted from cells using Trizol Reagent (Invitrogen, Carlsbad, CA). One microgram of RNA was reversely transcribed to cDNA. The mRNA expression was determined by real-time PCR using iQ SYBR Green Supermix (Bio Rad). Mouse Actb gene was used as endogenous control for sample normalization. Results were presented as fold increases relative to the expression of mouse Actb. The primer sequences used in PCR were as follows: Actb, 5’- TGCTGTCCCTGTATGCCTCT and 3’-TTTGATGTCACGCACGATTT; Cxcl1, 5’- CTTGCCTTGACCCTGAAGCTC and 3’- AGCAGTCTGTCTTCTTTCTCCGT; Cxcl2, 5’- CCCCCTGGTTCAGAAAATCA and 3’- GCTCCTCCTTTCCAGGTCAGT; Ccl2, 5’- CCCAATGAGTAGGCTGGAGA and 3’- AAGGCATCACAGTCCGAGTC; Il6, 5’- ACACATGTTCTCTGGGAAATCGT and 3’- AAGTGCATCATCGTTGTTCATACA; Rankl, 5’- AGCACGAAAAACTGGTCGGG and 3’- AAGGGTTGGACACCTGAATGC; and Mmp3, 5’- ACTCTACCACTCAGCCAAGG and 3’- TCCAGAGAGTTAGACTTGGTGG.
Cytokine measurement
Serum were obtained from mice at the indicated time points and immediately centrifuged at 1500 g for 15 min. Samples were stored at -70°C until ready for used. Cytokine levels were measured using Cytometric Bead Array (CBA) cytokine assay kit (BD) and the amount of IFN-γ and IL-17 were determined using Quick EIA™ ELISA kits from Dakewe Biotechnology Company (Shenzhen, China).
Isolation of T cells and B cells
Mouse T lymphocytes were isolated from lymph nodes of C57/BL6 mice and B lymphocytes were isolated from spleens of C57BL/6 mice. All cells were purified using magnetic beads (Miltenyi Biotec, Auburn, CA) with more than 95% purity. For antigen-specific lymphocyte responses, T cells were isolated from lymph nodes and B cells were isolated from spleens of CIA mice. The cells were incubated in RPMI 1640 medium supplemented with 10% fetal bovine serum (FBS), 100 U/ml penicillin, and 100 μg/ml streptomycin under a humidified 5% (v/v) CO2 atmosphere at 37°C.
Cell proliferation assay
Cells were cultured in 96-well plates at a density of 3×105 cells/well in RPMI 1640 medium (0.2 ml). Then the cells were treated with drugs and stimulated with 5 μg/ml of Con A for 24 h at 37oC in 5% CO2/air. Then cell growth was evaluated with modified MTT assay. MTT (4 mg/ ml in PBS, 20 μl per well) was added to each well. After 4 h of additional incubation, remove the culture media, 200 μl DMSO was added to dissolve the crystals. The absorption values at 570 nm were determined.
Measurement of cell apoptosis and CD23 expression with flow cytometry
Cell apoptosis was determined by Annexin V-FITC (fluorescein isothiocyanate) /PI (propidium iodide) staining. Samples were analyzed by FACS Calibur flow cytometer (Becton Dickinson, San Jose, CA). Annexin V+/PI- and Annexin V+/PI+ were considered as apoptotic cells in the early and late phase, respectively. Spleen cells (3×105) were stimulated with 1 μg/ml LPS with the addition of drugs simultaneously. The surface expression of CD23 was assessed after 24 h of culture. At the end of the culture period, the harvested cells were washed twice with buffer. Cells were stained with CD23 and B220 for 30 min at 4°C in the dark. Cells were then washed with buffer to remove the excess stains and analyzed in a FACS Calibur flow cytometer using Cell Quest software.
Statistics
Data are expressed as means ± SEM. Statistical analyses were performed using one-way analysis of variance (ANOVA) followed by Student’s two-tailed t-test. P<0.05 was considered significant.
Effects of the combination therapy with iguratimod and methotrexate on the development of CIA
According to our previous results, treatment with 30 mg/kg iguratimod resulted in a dramatic decrease in the arthritic scores and iguratimod at 10 mg/kg yielded a medium decrease in arthritic scores. In addition, treatment with 10 mg/kg methotrexate showed excellent antirheumatic properties, but with some adverse events. In this case, we chose 1 mg/kg methotrexate which could be well tolerated and 3 mg/kg plus 10 mg/kg iguratimod which showed mild antiarthritic properties for combined therapy. CIA was induced with type II collagen (CII) in CFA on day 0, then a booster injection with CII in IFA on day 21 in male DBA/1J mice. As shown in Figure 1, CIA developed rapidly in vehicle-treated mice, and the incidence of arthritis achieved to 100% on day 25 post-immunization (Figures 1A and 1B). These CIA mice developed severe swelling, erythema and joint rigidity of the paws (Figures 1D and 1E). Treatment with iguratimod (3 mg/kg, 10 mg/kg) or methotrexate (1 mg/kg) only exhibited very weak inhibitory effects on the arthritic scores. In mice combined treated with iguratimod (3 mg/kg) and methotrexate (1 mg/kg), the onset of arthritis was delayed and the severity of CIA was attenuated compared with the vehicle mice. Furthermore, combination therapy with iguratimod (10 mg/kg) and methotrexate (1 mg/kg) showed excellent antirheumatic activities with reduction of scores in comparison with the vehicle group. Hind paw swelling was measured and the results correlated with that of the clinical scores (Figures 1D-1F). The body weights of each group were recorded every day (Figure 1C), and expressed as a change in weight from arthritis induction (day 21). In this study, we did not observe any adverse events, such as loss of appetite, lack of movement and weight loss, indicating that both iguratimod and methotrexate were well tolerated at our tested doses.
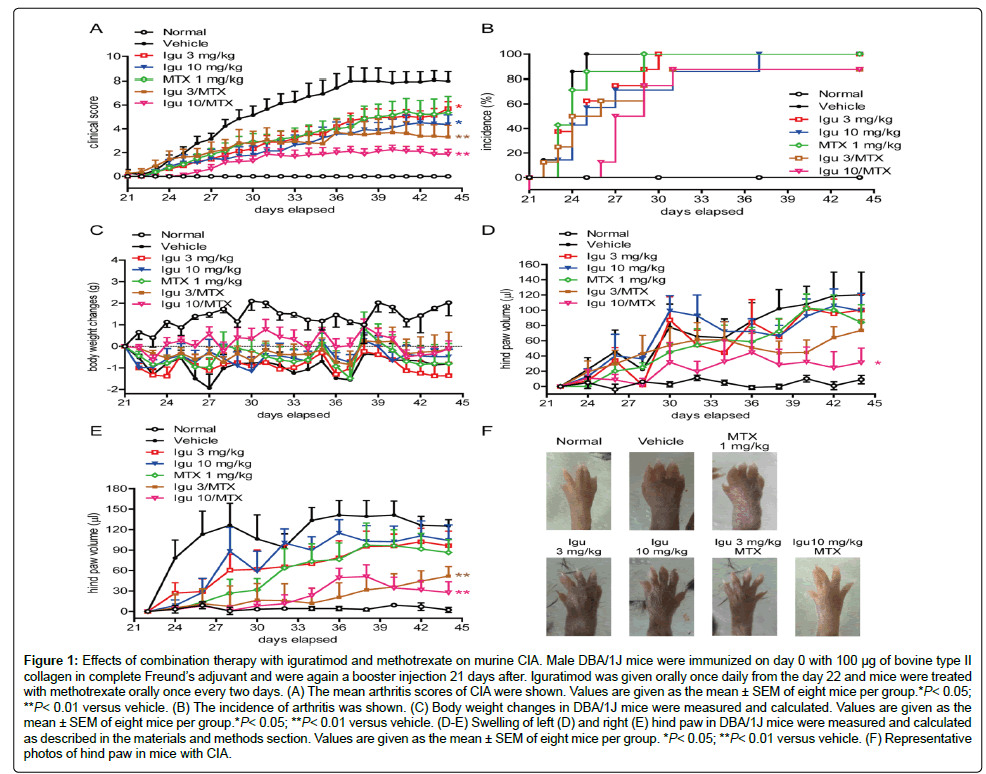
Figure 1: Effects of combination therapy with iguratimod and methotrexate on murine CIA. Male DBA/1J mice were immunized on day 0 with 100 μg of bovine type II collagen in complete Freund’s adjuvant and were again a booster injection 21 days after. Iguratimod was given orally once daily from the day 22 and mice were treated with methotrexate orally once every two days. (A) The mean arthritis scores of CIA were shown. Values are given as the mean ± SEM of eight mice per group.*P< 0.05; **P< 0.01 versus vehicle. (B) The incidence of arthritis was shown. (C) Body weight changes in DBA/1J mice were measured and calculated. Values are given as the mean ± SEM of eight mice per group.*P< 0.05; **P< 0.01 versus vehicle. (D-E) Swelling of left (D) and right (E) hind paw in DBA/1J mice were measured and calculated as described in the materials and methods section. Values are given as the mean ± SEM of eight mice per group. *P< 0.05; **P< 0.01 versus vehicle. (F) Representative photos of hind paw in mice with CIA.
Effects of combination therapy on bone erosion in mice with CIA
In the radiographic evaluation of fore and hind paws, bone erosion, articular destruction and joint displacement were detected in vehicletreated mice on day 44 (Figure 2A). However, oral administration of iguratimod and methotrexate displayed markedly protection against bone erosions and joint destructions as compared to vehicle group. Furthermore, no bone erosion was observed in mice treated with high dose of iguratimod (10 mg/kg) plus methotrexate. To confirm the protective effects, histological analysis was also carried out on the inflamed hind paws. The assessment revealed synovial hyperplasia, joint destruction and inflammatory cell infiltration of vehicle-treated mice (Figure 2B). In accordance with the effects on disease incidence and severity, combination therapy with iguratimod and methotrexate showed remarkable improvement in joint damage and inflammation as compared with those of the vehicle group. As shown in Figure 2B, cartilage and bone damage as well as inflammatory responses were significantly inhibited by the treatment of high dose iguratimod plus methotrexate.
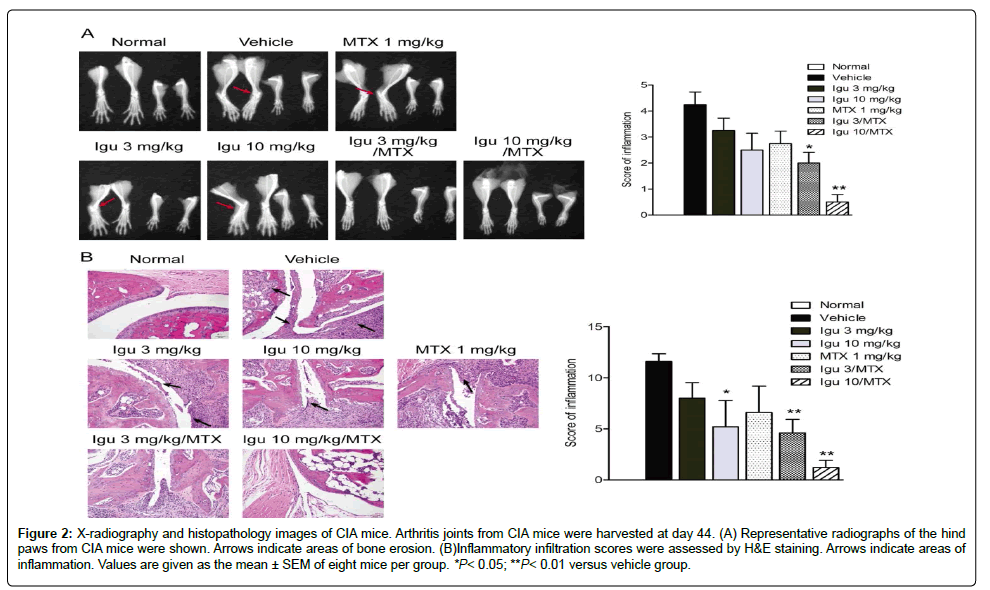
Figure 2: X-radiography and histopathology images of CIA mice. Arthritis joints from CIA mice were harvested at day 44. (A) Representative radiographs of the hind paws from CIA mice were shown. Arrows indicate areas of bone erosion. (B)Inflammatory infiltration scores were assessed by H&E staining. Arrows indicate areas of inflammation. Values are given as the mean ± SEM of eight mice per group. *P< 0.05; **P< 0.01 versus vehicle group.
Effects of combination therapy on local joint inflammation
The immunomodulatory effects of combination with methotrexate and iguratimod on proinflammatory cytokines, chemokines and tissue factors were further analyzed in inflamed paws. To evaluate whether the combination treatment suppressed the effector mechanisms of inflammation in CIA, the gene expression of various proinflammatory mediators was examined on day 44 by using quantitative real-time PCR. It was observed that combination therapy significantly decreased the mRNA levels of three major chemokines Cxcl1, Cxcl2, and Ccl2 compared to vehicle group in CIA. Also, growth factors associated with tissue destruction/remodeling were down-regulated by iguratimod or methotrexate treatment. The expressions of Rankl and Mmp3 were significantly reduced in the joints from combination therapy group (Figure 3).
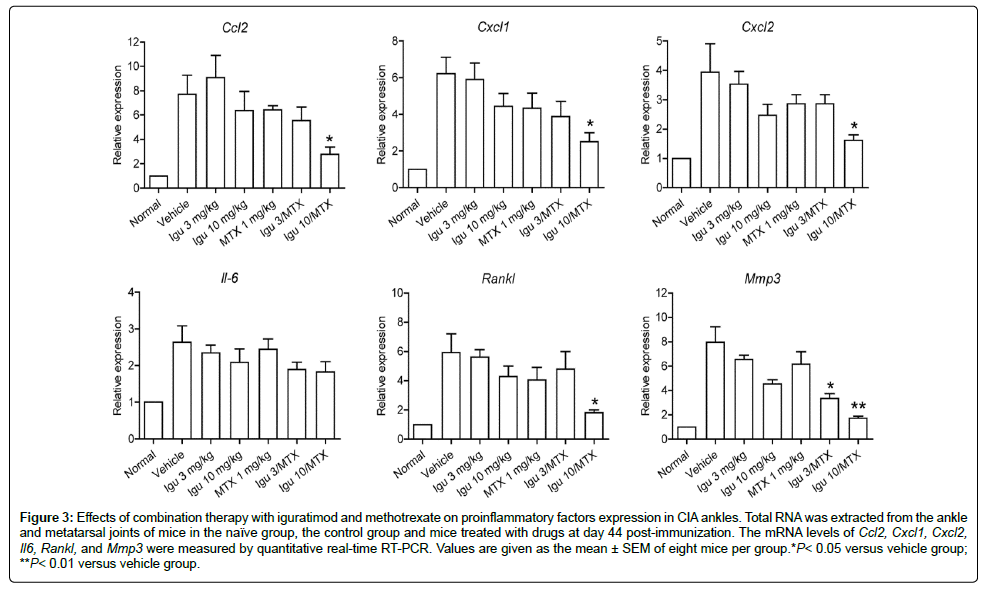
Figure 3: Effects of combination therapy with iguratimod and methotrexate on proinflammatory factors expression in CIA ankles. Total RNA was extracted from the ankle and metatarsal joints of mice in the naïve group, the control group and mice treated with drugs at day 44 post-immunization. The mRNA levels of Ccl2, Cxcl1, Cxcl2, Il6, Rankl, and Mmp3 were measured by quantitative real-time RT-PCR. Values are given as the mean ± SEM of eight mice per group.*P< 0.05 versus vehicle group; **P< 0.01 versus vehicle group.
Effects of combination therapy on serum pro-inflammatory factors levels in CIA mice
To investigate the mechanism by which combination therapy controls CIA development and progression, we examined the levels of pro-inflammatory cytokines in CIA mice. As shown in Figure 4A, IL-17 production was significantly inhibited by the combination of iguratimod and methotrexate. Meanwhile, combination therapy showed mild inhibition against IFN-γ, TNF-α, and IL-6 levels. No difference was observed in the serum IL-10 between vehicle and combined treatment group. Not only decreased T cell response but also decreased B cell activity could play a role in the efficacy of DMARDs treatment. Therefore, antigen-specific B cell responses were examined. We measured the serum levels of total IgG or isotype-specific IgG2b anti-CII antibodies after treatment with different DMARDs. As shown in Figure 4B, treatment with methotrexate resulted in decreased levels of IgG and IgG2b antibodies. Furthermore, serum concentrations of IgG and IgG2b antibodies were significantly reduced by combination treatment of high dose iguratimod (10 mg/kg) plus methotrexate (Figure 4B).
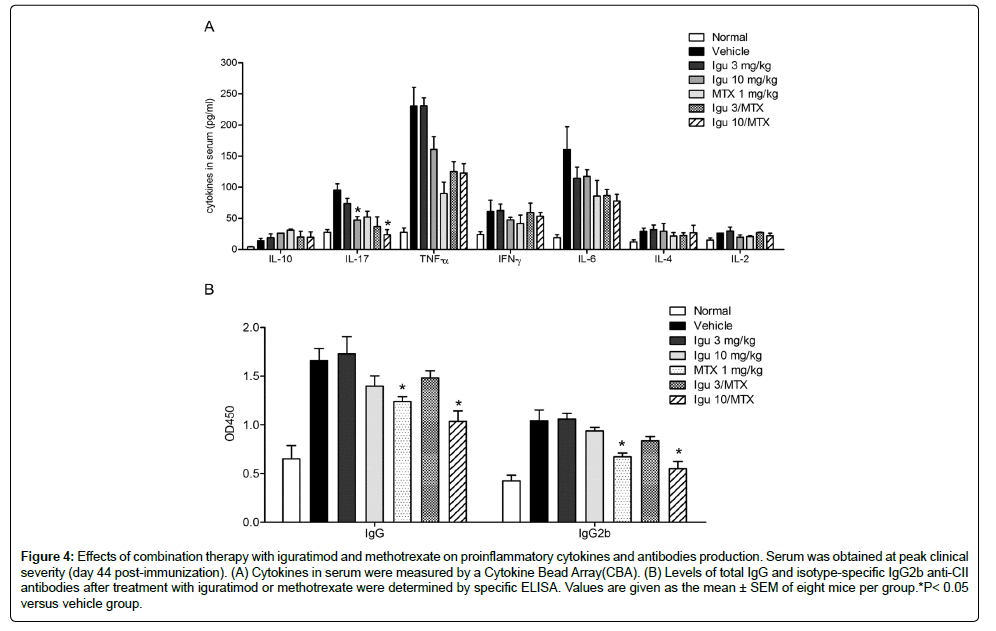
Figure 4: Effects of combination therapy with iguratimod and methotrexate on proinflammatory cytokines and antibodies production. Serum was obtained at peak clinical severity (day 44 post-immunization). (A) Cytokines in serum were measured by a Cytokine Bead Array(CBA). (B) Levels of total IgG and isotype-specific IgG2b anti-CII antibodies after treatment with iguratimod or methotrexate were determined by specific ELISA. Values are given as the mean ± SEM of eight mice per group.*P< 0.05 versus vehicle group.
Effects of combination therapy on antigen-specific responses in CIA mice
Moreover, we evaluated antigen-specific responses of peripheral T cells isolated from CIA mice. As shown in Figure 5A and 5B, vehicle-, b iguratimod-, and methotrexate- treated mice exhibited comparable levels of serum cytokines, including IFN-γ and IL-17. However, combined treatment with iguratimod plus methotrexate resulted in significant reduction in the levels of IFN-γ and IL-17. Similar results were showed in antigen-specific T cell proliferation and B cell proliferation (Figure: 5 C and D). No significant difference was observed in CII-specific T cell proliferation or LPS-induced B cell proliferation between vehicle-, iguratimod-, and methotrexate-treated mice. However, combination with iguratimod and methotrexate markedly inhibited cell proliferation induced by denatured CII or LPS.
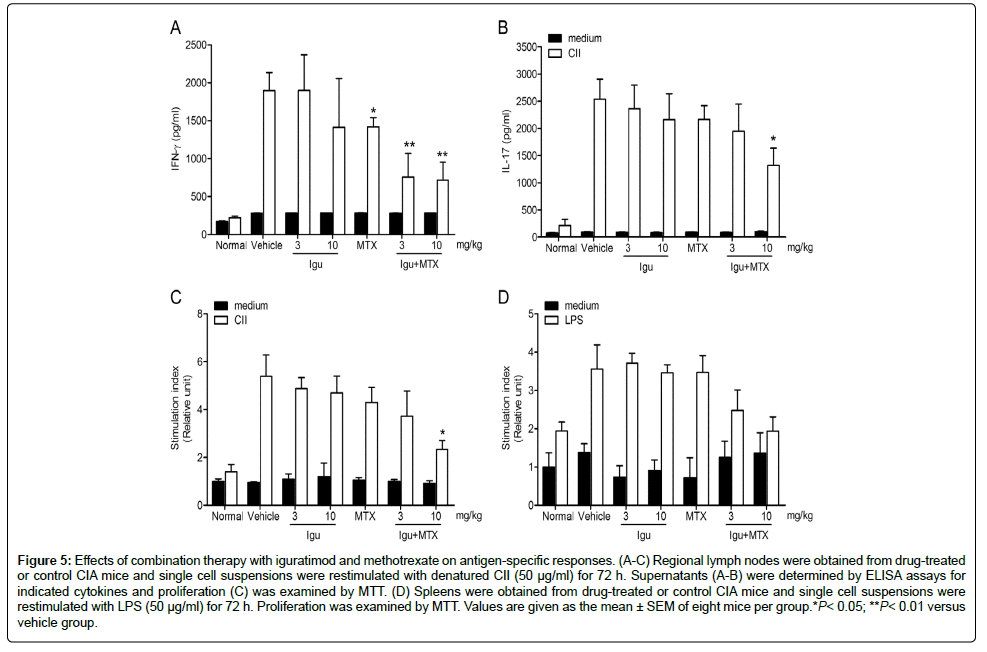
Figure 5: Effects of combination therapy with iguratimod and methotrexate on antigen-specific responses. (A-C) Regional lymph nodes were obtained from drug-treated or control CIA mice and single cell suspensions were restimulated with denatured CII (50 μg/ml) for 72 h. Supernatants (A-B) were determined by ELISA assays for indicated cytokines and proliferation (C) was examined by MTT. (D) Spleens were obtained from drug-treated or control CIA mice and single cell suspensions were restimulated with LPS (50 μg/ml) for 72 h. Proliferation was examined by MTT. Values are given as the mean ± SEM of eight mice per group.*P< 0.05; **P< 0.01 versus vehicle group.
Effects of combination therapy on T cell responses
To examine the immunosuppressive potential in vitro, we evaluated the effects of combination therapy on the Con A-induced proliferation of T cells. MTT assay showed that iguratimod slightly inhibited T cell proliferation induced by Con A. The similar result was also seen in T cells treated with methotrexate. However, iguratimod in combination with methotrexate efficiently inhibited T cell proliferation induced by Con A. Subsequently, we determined whether the combination treatment could induce apoptosis of lymphocytes. We incubated T cells with iguratimod, methotrexate or iguratimod plus methotrexate in the presence of Con A for 24 h. Iguratimod did not influence the apoptotic cell counts relative to the untreated cells. However, cell apoptosis was detected when methotrexate was used. As shown in Figure 6B, combined incubation with iguratimod and methotrexate resulted in significant apoptosis of 40% at 0.1 μM and 55% at 3 μM, respectively.
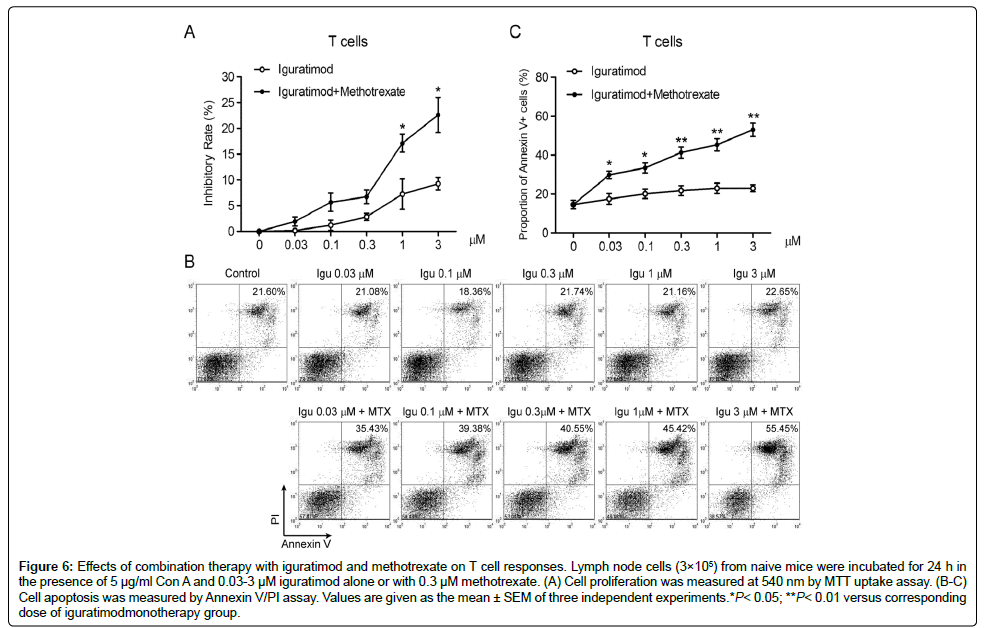
Figure 6: Effects of combination therapy with iguratimod and methotrexate on T cell responses. Lymph node cells (3×105) from naive mice were incubated for 24 h in the presence of 5 μg/ml Con A and 0.03-3 μM iguratimod alone or with 0.3 μM methotrexate. (A) Cell proliferation was measured at 540 nm by MTT uptake assay. (B-C) Cell apoptosis was measured by Annexin V/PI assay. Values are given as the mean ± SEM of three independent experiments.*P< 0.05; **P< 0.01 versus corresponding dose of iguratimodmonotherapy group.
Effects of combination therapy on B cell responses
Given the reduction of antibodies on CIA mice, it seems likely that these drugs could regulate B cell activation or function. To explore this possibility, purified splenic B cells were stimulated with LPS in the presence of iguratimod, methotrexate or iguratimod plus methotrexate for 24 h, and then the proliferative response was assessed. As shown in Figure 7A, proliferation of LPS-stimulated B cells was inhibited by iguratimod in a dose-dependent manner. And the addition of methotrexate increased the inhibitory rate. Inhibition of B cell activation was also demonstrated by B cell activation marker CD23. Combination with iguratimod and methotrexate showed significant reduction of CD23 expression in the anti-B220-labeled B cells (Figures 7B and 7C). And culture supernatants from iguratimod plus methotrexate showed lower IgG and IgM levels compared with those from iguratimod (Figures 7D and 7E).
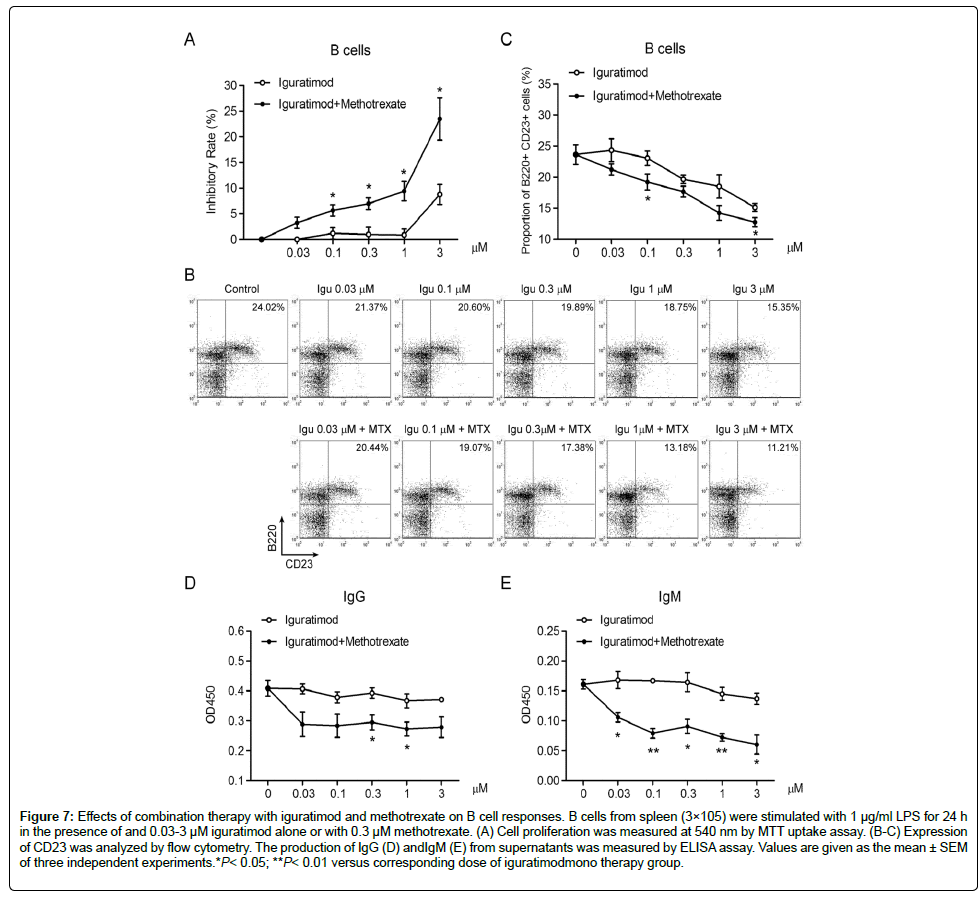
Figure 7: Effects of combination therapy with iguratimod and methotrexate on B cell responses. B cells from spleen (3×105) were stimulated with 1 μg/ml LPS for 24 h in the presence of and 0.03-3 μM iguratimod alone or with 0.3 μM methotrexate. (A) Cell proliferation was measured at 540 nm by MTT uptake assay. (B-C) Expression of CD23 was analyzed by flow cytometry. The production of IgG (D) andIgM (E) from supernatants was measured by ELISA assay. Values are given as the mean ± SEM of three independent experiments.*P< 0.05; **P< 0.01 versus corresponding dose of iguratimodmono therapy group.
Methotrexate, originally developed for leukemia therapy, has become to be the cornerstone of DMARD in the management of RA worldwide [29,30]. In RA, it is the first one to be chosen due to its excellent efficacy, tolerability, safety and cost [31]. However, for its dose-dependent adverse effects, methotrexate could be prescribed in combination with other synthetic or biological agents [32,33]. CIA has been widely used in preclinical studies as an animal model of RA, for evaluation of antiarthritic drugs [34]. In this study, the therapeutic effect of combination of iguratimod and methotrexate on CIA mice was investigated. It was indicated that the inflammation of joints, elevation of serum cytokines and antibodies levels, and bone destruction were all relieved through combination therapy. Evaluation of CIA in the present study has been performed on paw swelling, clinical scores, body weight, histopathology and X-radiography. Here we compared antiarthritic effects of iguratimod or methotrexate alone in CIA with combined iguratimod and methotrexate. Combination therapy was more efficacious to not only decrease clinical scores of disease but also reduce paw swelling than monotherapy. Histological and radiological analysis of joints further support that combination of iguratimod and methotrexate has strong anti-inflammatory effects as well as protective effects on joint tissue damage. The infiltration of inflammatory cells into the synovium plays a pivotal role in the progress of RA [1,35]. These cells release cytokines, chemokines, tissue factors, and metalloproteinases to lead to bone and cartilage destruction [36]. The gene expression of various proinflammatory mediators in inflamed paws was significantly reduced by combined iguratimod and methotrexate. Thus, in the present study of an animal model of RA, the combination therapy with iguratimod and methotrexate exerted stronger antiarthritis effect than the monotherapy. There has been a randomized, double-blind, placebo-controlled trial reported, iguratimod was orally administered at doses of 50 mg/day and methotrexate was orally administered at doses of 8 mg/week for combination treatment [37]. Corresponding doses in mice were about 6.9 mg/kg/day and 1.2 mg/kg/week, respectively. In this case, the dosages of iguratimod and methotrexate we selected in our experiments were correlated to clinical studies. And the positive results and possible mechanism could be supportive for clinical trials. It is believed that the pathogenesis of RA is closely related to dysregulation of T and B lymphocytes [36,38] and CIA is trigged by immune responses to type II collagen (CII). Therefore, pro-inflammatory cytokines and antibodies levels in serum of CIA mice were investigated. Efficacy in decreasing IL-17, IFN-γ, TNF-α, IL-6, IgG, and IgG2b productions was stronger in use of combined iguratimod and methotrexate than with use of iguratimod or methotrexate alone. Then CII and LPS were used to induce immune responses ex vivo. Iguratimod plus methotrexate treatment resulted in significant reduction in the levels of cell proliferation induced by denatured CII or LPS. Furthermore, CII induced elevations in IFN-γ and IL-17 levels were also suppressed in the combination treated CIA mice. Consequently, we employed in vitro models through T cell activation using Con A and B cell activation using LPS, respectively. It was found that monotherapy only slightly inhibited Con A induced proliferation but combination therapy showed stronger inhibitory effect than monotherapy group. Similar results were observed in Con A-induced apoptosis of T cells. Antibody response is of central importance because B cell-deficient mice do not develop the disease. In our study, proliferation and activation of LPS-stimulated B cells was significantly inhibited by iguratimod in a dose-dependent manner. And the addition of methotrexate remarkably enhanced the inhibitory effect on B cells. Taken together, the present study shows that combination treatment of iguratimod and methotrexate is superior to monotherapy in murine CIA, which can be expected to exert additive effects in alleviating the symptoms of RA. The mechanism of action was due to the inhibitory effects of iguratimod on fibroblast-like synoviocytes plus with the suppressive functions of methotrexate on T cells and B cells.
These findings collectively suggest that combination therapy of iguratimod with methotrexate may be preferable of therapeutic value for the treatment of human RA.
The authors declare that they have no competing interests.
We thank Simcere Pharmaceutical Company (Nanjing, China) for providing iguratimod. This work was supported by National Natural Science Foundation of China (Nos. 81273528, 81101563, and 91229109), Jiangsu Province Clinical Science and Technology Project (Clinical Research Center, BL2012008), and Ph.D. Programs Foundation of Ministry of Education of China (No. 20110091110016).