Journal of Research and Development
Open Access
ISSN: 2311-3278
ISSN: 2311-3278
Research Article - (2016) Volume 4, Issue 1
Background
Evaluating national health research systems (NHRS) in six Pacific Island states - Fiji, Solomon Islands, Vanuatu, Samoa, Tonga and the Cook Islands - is a key step in determining whether their systems, infrastructure and processes are in place to effectively manage health research resources and facilitate conduct of research and its implementation.
Methods
The COHRED questionnaire used in a 2007 mapping of the Pacific Islands was utilised to survey informants from the six countries.
Results
Fiji had a more developed NHRS followed by the Cook Islands and the Solomon Islands. There was no correlation between the degree of NHRS development and population size, level of GDP or SCImago ranking for research output. All the six countries had a research structure accompanied by a satisfactory level of coordination. However, there was not always dedicated personnel assigned and there was a lack of research policies and legislation in all jurisdictions. With the exception of Fiji and the Solomon Islands, the countries had weak ethics processes and there were no monitoring and evaluation systems with the exception of Samoa.
Conclusions
The NHRS in six Pacific Island states vary from less developed in Vanuatu to more developed in Fiji. The development of the various components of a NHRS in small Island states is sensitive to political, funding and human resource pressures. There is room for improvement; nevertheless, there is no need in developing all the components of a NHRS in a resource-constrained setting as long as the various countries develop a Pacific solution that includes research collaborations and resource sharing with other Pacific and Pacific-rim countries.
<Keywords: Pacific island countries; Health research systems; Clinician researchers; Research capacity building
In 1990, the independent Commission on Health Research for Development drew attention to the disparate burden of disease in developing countries (93%) with global health research investment to address these limited to only five percent [1]. This set in motion a range of global commitments with the establishment of the Council on Health Research for Development (COHRED), tasked to support the development of health research systems capacity with a focus on lowand middle-income countries (LMIC) [2]. In 2005, the World Health Assembly adopted resolution WHA58.34, which acknowledged the critical role of research in realising global development goals and equitable health, urging member states and the global scientific community and relevant stakeholders to work towards strengthening national and global health research systems.
The Pacific region discussion on health research systems in Pacific Island countries and territories in 2007 began with a presentation on the status of health research in the Pacific based on the use of a mapping tool devised by COHRED [3]. This tool comprised 18 questions modified for the Pacific context seeking health research information through structured interviews with key informants from 15 Pacific Island countries and territories. The mapping tool investigated four key health research areas; governance, policies and priorities, communication dissemination and utilization, and routine health information systems, as well as health research stakeholders. Results suggested that health research systems in the Pacific were poorly resourced and structured. A set of 19 recommendations from the meeting proposed a range of strategies to bridge the health research systems gap including the ring-fencing of research funds by member countries (2% health budget) and international partners (5% health development aid) [4].
It was estimated that up to 85% of maternal and neonatal deaths in LMIC could have been prevented if only current research evidence was implemented [5]. The lack of utilization of research evidence, let alone the lack of evidence generation, is a result of a limited or nonfunctioning health research system, where research producers, consumers and other stakeholder partners in utilizing research to achieve national development and health equity [6-8]. Whereas there has been an increase in research capacity building (RCB) in LMIC over the last three decades, the World Health Organization (WHO) since 2005 preferred strengthening national health research system (NHRS) as a way of developing capacity from top down [9]. The concept was formed on the basis that health research could only be performed where there was a living health system. The top down approach includes amongst other values, building governance and management skills, research policy development, legislation and ethics processes and research utilization procedures [2].
The aim of this study was to map and compare the NHRS of six Pacific countries to determine whether there had been any changes in the NHRS of six of the 15 Pacific countries since the WHO mapping in 2007. Countries selected as part of the building reproductive health research and audit capacity and activity in the Pacific Islands (BRRACAP) study [10], were included (Cook Islands, Fiji, Solomon Islands, Samoa, Tonga and Vanuatu). The secondary aim of the study was to determine if there was any correlation to selected economic indicators. The study should inform whether the six countries had a NHRS that would be supportive of researchers and research.
Quantitative data was collected and analyzed utilizing similar research methodologies used to investigate the status of Pacific health research systems in 2007, based on the COHRED structured questionnaire [4]. The COHRED questionnaire was sent by email to senior representatives of the Ministries of Health and/or senior researchers of the six countries in 2012, inviting them to participate in the study. An updated version was completed in 2015 to verify health research system status.
No attempt was made to verify the accuracy of the data given so the information, as with that of the 2007 mapping, should be considered indicative. One of the authors (AE) provided additional information with a subjective score for each of the 18 questions in the governance and management section based on the scoring scheme as outlined in the 2007 mapping study [4]. The scoring scheme assigned zero (0) if the response was no or none, one (1) if there was some development, and two (2) if the area was well developed. As with the previous study, each question carried equal value and they were not ranked for importance.
Two informants who were senior or appointed representatives/ senior researchers from Samoa, Fiji and the Cook Islands completed the questionnaire. Only one informant from the Ethics Committees and Ministry of Health completed the questionnaires for Vanuatu and the Solomon Islands respectively. In the case of Tonga, the questionnaire was completed by one of the authors (AE) during an interview with five members of Tonga’s Ethics Committee.
To determine if there was a correlation between a country’s NHRS score and selected demographic measures in population size, gross national product (GDP) per capita, government expenditure on health per capita in international dollars, number of physicians per 1,000 population and a SCImago country ranking [11] for research output were used. A Pearson chi square test was used to test for association (IBM SPSS Version 23). Ethics approval was obtained from the University of Auckland Human Participants Ethics Committee.
Study results suggest that Fiji has the most developed NHRS among the Pacific Island countries assessed followed by the Cook Islands, Solomon Islands and Samoa (Table 1). All countries were more developed in the areas of research structures, health priorities, a responsible party for Monitoring and Evaluation of policy/ intervention, systems to collect/analyse/report routine health information, health care institutions, international research partners, and engaging key stakeholders. Less developed areas were those relating to research plans and policies, formulating research priorities, research legislation, stated values and aims, actual monitoring and evaluation, engagement of other ministries, other research organisations and media active in dissemination of research evidence.
| Melanesian countries | Polynesian countries | |||||
|---|---|---|---|---|---|---|
| Components of NHRS/countries | Fiji | Solomon Islands | Vanuatu | Samoa | Tonga | Cook Islands |
| Structure | National Health Research Committee (NHRC); Fiji National Research Ethics Review Committee (FNRERC) | National Health Research and Ethics Committee (NHREC). The National Health Research and Training Institute (NHTRI) Research Unit helps facilitate health research. | Vanuatu National Health Research Ethics Committee (VNHREC) | National Health Research Committee (NHRC) | Technical sub-committee chaired by the director; then to National Health Development Committee. | Research Office (RO) within the Office of the Prime Minister with research director |
| Management & coordination | Director Health Information & Research Analysis (DHIRA) | All health research proposals have to go through the NHERC. The NHERC chairman and secretary are from the Ministry of Health (MOH) and the NHTRI. | Applications to VNHREC | Director General is the Chair of the NHRC | Secretary and chair of Ethics Committee. | Applications to RO or relevant Ministry for comments and recommendations – National Research Committee (NRC)– research permit (if approved) |
| Dedicated personnel | Full time MOH research officer coordinates and facilitates health research in Fiji and serves as a secretariat to both NHRC and FNRERC | Coordinated by NHTRI which has a director who oversees administrative matters. However, at present NHTRI only has 3 staff. | None. The Health Information Systems (HIS) manager has been assigned the role of the VNHREC focal person | Yes, the MOH Research Unit is Secretariat | None | MOH has a Health Research Committee that advises the RO |
| Plan/policy | In draft for MOH approvals | In draft | We have a protocol in place but we don’t have a policy. | ToR for NHRC Draft Research Guidelines | None | None |
| Active national health priorities | Defined in MOH strategic plans for HIV/AIDS, NCDs, and risk factors, nutrition, environmental health, systems research, programme evaluation, health promotion | Maternal and child health, HIV/AIDS, TB, Malaria, clean and sustainable water supply. Millennium Development Goals (MDGs) - these are health issues that receive external funding. | Strategic Plan 2011 – 2016. 1. Reduce Child mortality 2. Improve maternal health 3. Equitable access to quality health services etc. | Health Systems Strengthening, Primary Health care, E-health, Diseases Prevention and Control, NCDs, Cancer/maternal and child health, Cervical cancer – screening, HIV Vaccination, etc | MDGs | MOH new strategic plan 2015-2019 |
| Active national health research priorities | Same as national health priorities | No | No | Yes, from the Health Sector Plan | No | Reference to the health priorities on research website |
| Research legislation | In draft | None | None | Under consideration | Ethics committee – goes to cabinet | None |
| Stated values | In draft | None | None | NHRC ToR, Guidelines | None | None |
| Stated aims | In draft | To provide quality research carried out in an ethical manner. Ensure capacity building within the field of health research. | None | Manage sound external research that benefits Samoa | None | None |
| Monitoring and evaluation (M&E) | Not done formally. With the web- portal, there is potential for monitoring and evaluation. | No | No | NHRC assesses proposals, Provide feedback to researchers, provide stance in relation to findings and review final manuscript before approval | No | Minimal, only through submission and presumed review of reports |
| Ethical review process and structure | Yes, FNRERC with regular meetings and standard procedure forms | Ethical reviews are done by NHERC. NHRC chairman or secretary along with an ethics review application form. Following review the submitting investigator will be informed of the outcome. | Corporate services under the MOH | Under review | As above Last meeting was last year | No committee for ethical review; ethical process relies on overseas Ethical Review Committees, also gets advice from the Health Research Council of NZ or HRCP as needed. |
| How use of research increased | Mainly through information brought to the MOH Executive Committee that is translated into policy action; efforts at evidence-based programme development (e.g. NCDs) | The MOH holds a yearly national health conference in which research results can be presented. All analysis is encouraged to be done within the country. | NA | Research results passed to Executive Management for implementation of recommendations | Annual recordings Annual reports | Increasing work with policy makers with research findings to provide evidence-based policy and decision making |
| How policy-makers informed of advances | New requirement for return of research reports to the MOH especially if ethics approvals are granted by the NHRC or FNRERC | Overseas meetings and the national health conference | NA | Internet and CME are available | None Visiting speakers Paid for up-to-date for clinicians | WHO, South Pacific Commission (SPC) meetings; overseas conferences; annual Cook Islands health conference; visiting consultants; MOU with NZ health provider for support; training attachments through National Human Resources Department |
| Responsible party for result dissemination | Researchers via the Health Research portal (HRP) | NHTRI has taken on the responsibility but the policy is still in draft form. | No specific mechanism – it happens by meetings or attending conferences. | NHRC puts copy of research in library | Annual reports released to public e.g. life expectancy. | RO requires 3 reports: RO, National Library, relevant ministry, different ministries with individual dissemination strategies |
| Responsible party for M&E of policy/intervention | At the discretion of the MOH Executive Committee and responsible directors | The Director of Health Policy and Planning for the Ministry of Health. | The Health Planning Unit in conjunction with the Health Sector Analyst in the M&E unit under the Prime Minister’s Office. | Strategic division (MOH) Policy and Planning Unit | DOH through the clinicians | Relevant ministry or organisation, usually in the form of a review or report |
| System to collect/analyse/report routine health information | Through Patient Information System, HRP, regular reports from other service sites, some disease based registries (e.g. cancer) | Provinces and National Health Divisions submit information and reports to the National Health Information System at the Ministry of Health’s Health Statistics Unit. | Health Information System – a routine monthly health activities and morbidity reporting from the 6 administrative provinces. Provincial morbidity reports, hospital reports, Annual HIS reports are produced on an annual basis. | Health Information System (HIS), paper info is entered electronically, community-based HIS for public funded services, Annual Health Report | Monthly report form the Islands Quarterly reports and immediate notification | Routine data through the MOH (e.g. NCDs, immunisations, water quality, etc) MOH with Statistics Unit that publishes an annual health statistics bulletin with some separate reports |
| Regulation of new health technologies, including drugs | National Drugs and Therapeutics Committee, National Equipment Committee, National Training Committee | National Drug and Therapeutics Committee regulates the introduction of new drugs. New health technologies are regulated by the Department of Planning and Policies. | NA | National Medicines and drug Policy and action Plan 2008; National Food and Nutrition Policy 2013 – 2018; National Infection Control Policy 2011 – 2016; National Tobacco Control Policy 2010 – 2015; National alcohol Policy; Food Act 2015 | Drug committee – National committee determines drug list. No approval for procedures -approved by clinicians in weekly meetings | No specific mechanism: some regulatory bodies – Public Health CODEX Committee, Cook Islands Medical and Dental Council |
| Non-health ministries with officials dealing with health | Collaboration with local universities, MoE, Department of Immigration and Ministry of I-Taukei affairs for inclusion of members into health research discussions and on the FNRERC. | No | No | NA | Certain people from finance designated to health | Minimal Statistics Office in Ministry of Finance – census, expenditure survey with some health questions |
| Institutions engaged in research for health | ||||||
| Government departments/agencies | MOH, MOE Department of Immigration, I- Taukei affairs | NHRTI, National Vector-borne Disease and Control Program | No | Composition of NHRC Membership is under review | No | MOH, Ministry of Marine Resources, National Environment Service, National Statistics and MoE, Ministry of Agriculture |
| Heath care system institutions | Divisional hospitals | NRH Honiara | Vanuatu Hospital | National Referral Hospital in Upolu and Savaii Teaching Hospital | No | Rarotonga Hospital |
| Higher education institutions/national research institutes/laboratories | College of Medicine, Nursing & Health Sciences; Fiji National University, University of the South Pacific and University of Fiji. | No | No | Collaborative working relationship | No | University of the South Pacific |
| Private non-profit organizations | Fiji Medical Association, SPC/Pacific Islands AIDS Foundation, South Pacific Applied GeoScience Commission Medical Services Pacific (MSP), IFPP (International foundation for planned parenthood), IFRC (red cross), | No | No | NA | No | Cook Islands Family Welfare Association |
| Business enterprise or industry | Tebbutt Research | No | No | Not yet | No | None |
| International research and development sponsors/partners | WHO, UNDP, UNICEF And JICA, AUSAID, EU, NIH, NHMRC (Aus, NZ), Global Fund | WHO International Center of Excellence for Malaria Research | No | WHO, Government of Samoa, SPC, | WHO, UNFPA, Japan, AUSAID | Institute of Environmental Science and research (NZ), WHO, SPC, NZ National Institute of Water and Atmospheric research, Pacific Islands Geoscience Commission, Australian Agency for International Development, Asian Development Bank |
| Media organizations active in dissemination | Health Promotion flyers and brochures through media and National Centre for Health Promotion, media releases and health warnings, one TV station, talk back radio and health talks on radio, 3 newspapers, several Fiji-based internet sites, Fiji One, Mai TV | None | No | NA | Newspapers, radio and TYV station | TV (1), national radio (1), FM radio (3), newspapers, international radio and TV, SPC media production |
| Key stakeholders | MOH, WHO, Fiji School of Medicine Also, Ministry of Immigration and Ministry of Education (MoE). | MOH and Medical Services, NHTRI | WHO, SPC, Unicef | National University of Samoa, Oceania School of Medicine, regional institutions, MOH | Funders | WHO, SPC |
| Sources for previous analysis, reports or information | MOH with strategic plan, corporate plan, annual reports; other reports in priority areas (e.g. HIV/AIDS, NCDs); National Health Research guide in 1999; Flyers and brochures with information on HR system; WHO reports, country surveys, and national demographic reports. | Demographic Health Surveys Annual National Health Reports of MHMS - contains reports from the various departments of the Ministry of Health. | NA | International journals, WHO and World Bank publications | Annual reports | MOH Statistics Bulletin, WHO Publications/updates, population census, MOH health surveys/reports |
The scoring of the various responses are presented in Table 2 and are ranked by highest total score (Fiji) to the lowest (Vanuatu). All the countries had a reasonably well-developed research structure except Tonga and Vanuatu. No country had published research policy or plans. However, while all countries had systems to collect and analyse data, we were unable to ascertain the integrity and usefulness for clinical practice. There was no statistically significant association between the NHRS scores and any of the demographic and economic variables listed in Table 3.
| Components of NHRS/countries | Fiji | Cook Islands | Solomon Islands | Samoa | Tonga | Vanuatu | Total (out of 12) |
|---|---|---|---|---|---|---|---|
| Structure | 2 | 2 | 2 | 2 | 1 | 1 | 10 |
| Coordination | 2 | 2 | 2 | 1 | 1 | 1 | 9 |
| Dedicated personnel | 2 | 2 | 2 | 1 | 0 | 0 | 7 |
| Plan/Policy | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Health priorities | 2 | 2 | 2 | 2 | 1 | 2 | 11 |
| Research priorities | 1 | 1 | 0 | 1 | 0 | 0 | 3 |
| Legislation | 1 | 0 | 0 | 1 | 1 | 0 | 3 |
| Stated values | 1 | 0 | 0 | 1 | 0 | 0 | 2 |
| Stated aims | 1 | 0 | 2 | 2 | 0 | 0 | 5 |
| M&E | 0 | 0 | 0 | 2 | 0 | 0 | 2 |
| Ethical review process/structure | 2 | 1 | 2 | 1 | 1 | 1 | 8 |
| Utilisation of research | 2 | 2 | 2 | 2 | 1 | 0 | 9 |
| Info for policy-makers | 2 | 2 | 1 | 1 | 0 | 0 | 6 |
| Dissemination | 2 | 2 | 1 | 0 | 1 | 0 | 6 |
| Responsible party for M&E of policy/intervention | 2 | 2 | 2 | 2 | 1 | 2 | 11 |
| System to collect/analyse/report routine health information | 2 | 2 | 2 | 2 | 2 | 2 | 12 |
| Regulation of new health technologies | 2 | 1 | 2 | 2 | 1 | 0 | 8 |
| Non-health ministries with officials dealing with health | 2 | 1 | 0 | 0 | 1 | 0 | 4 |
| Government departments/agencies engages in research | 2 | 2 | 2 | 1 | 0 | 0 | 7 |
| Heath care system institutions | 2 | 2 | 2 | 2 | 1 | 2 | 11 |
| Private non-profit organizations | 2 | 1 | 0 | 0 | 0 | 0 | 3 |
| Business enterprise or industry | 1 | 0 | 0 | 0 | 0 | 0 | 1 |
| International research and development sponsors/partners | 2 | 2 | 2 | 2 | 2 | 1 | 11 |
| Media organizations active in dissemination | 2 | 2 | 0 | 0 | 1 | 0 | 5 |
| Key stakeholders | 2 | 2 | 2 | 2 | 2 | 2 | 12 |
| Sources for previous analysis, reports or information | 2 | 2 | 2 | 2 | 1 | 0 | 9 |
| Total (out of 52) | 43 | 35 | 32 | 31 | 20 | 14 |
Table 2: Scores for components of NHRS governance and management.
| Fiji | Cook Islands | Solomon Islands | Samoa | Tonga | Vanuatu | |
|---|---|---|---|---|---|---|
| NHRS score | 43 | 35 | 32 | 31 | 20 | 14 |
| Ï Population (1000) in 2008 | 844 | 20 | 511 | 179 | 104 | 234 |
| †GDP per capita | 8,200 | 9,100 | 1,900 | 5,200 | 4,900 | 3,300 |
| Ï Govt expenditure on health per capita in international $ | 199 | 518 | 99 | 188 | 216 | 90 |
| Ï No. of physicians per 1,000 pop. | 0.5 | 1.1 | 0.1 | 0.3 | 0.3 | 0.1 |
| ¥ SCImago world ranking | 125 (1st ) | 214 (6th) | 184 (2nd) | 187 (4th) | 203 (5th) | 185 (3rd) |
| †https://en.wikipedia.org/wiki/List_of_Oceanian_countries_by_population (most are official estimates and current to 2016) (Last accessed 10 Jan 2016) Ï Statistical Yearbook for Asia and the Pacific 2009. http://www.unescap.org/stat/data/syb2009/ESCAP-SYB2009.pdf (Last accessed 20 Jan 2016). ¥ SCImago world ranking. http://www.scimagojr.com/countryrank.php (Last accessed 20 Jan 2016) |
||||||
Table 3: Countries with their demographic/economic variables.
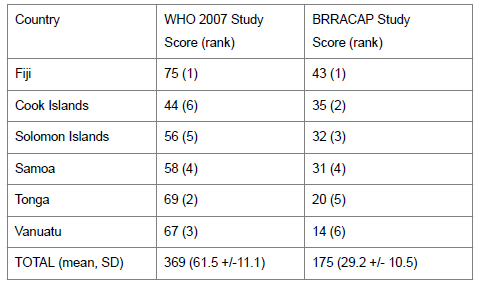
Table 4: Scores for all components of the NHRS (using COHRED components and tool) and comparisons between the WHO Study and this study for six countries. (calculation using a paired sample test, SPSS 23).
Fiji has the most developed NHRS of the six countries with Vanuatu and Tonga having the least developed systems. All six countries had research governance structures although there was a lack of health research planning, policies, research prioritisation and legislation. It would be difficult to have stated research aims and values without a legal or policy framework underpinning them. Although ethical frameworks could be strengthened in four of the countries, what was clearly lacking was the monitoring and evaluation of research. All the countries have health plans and systems for collecting and collating health data. They also had a structure for health service delivery and they had to strategically engage with stakeholders who were in the main, a funding partner of health services. The Cook Islands is the smallest and yet it had a NHRS second only to Fiji. There was no correlation between how well developed a country’s NHRS was with selected demographic and economic indicators.
Compared to the 2007 mapping by WHO [4], there have been improvements in the research governance and management in Fiji, Samoa, Solomon Islands and the Cook Islands with some of them being significant. In contrast, Tonga and Vanuatu seemed to have had a reversal in earlier gains as shown in the 2007 mapping. Factors favouring improvements in NHRS were political stability, health research leaders and a collaboration with a well-developed NHRS as in the case of the Cook Islands.
The political stability following the coupe detat of 2006 has seen major re-investment across the Fijian economy and health sectors which is the most likely reason for the improvement in the country’s health research infrastructure and systems. In contrast, the political instability in Vanuatu for the past 5 years had seen a change of health management personnel, which led to a reversal of earlier infrastructural stability. There was a period when there was no ethics committee in Vanuatu as they had been dismissed as part of the political instability. Health research structures in small Pacific states are prone to collapse, as systems are dependent on a few health personnel with the expertise, enthusiasm and research leadership skills.
Health researchers and research skills are lacking in most Island states. In the case of Tonga, the departure of a key health researcher and a lack in research leadership led to a stagnation in the monitoring and evaluation of research. The ethics committee had not met for a year and there were research projects that the ethics committee were aware of that had been conducted without ethics approval.
In addition, local research funding is either non-existent or limited [3]. In order to attract international funding to build local capacity, there needs to be a local researcher or a functioning research system [12]. Pacific countries, such as Fiji, with researchers, a tertiary medical institution and a more developed NHRS are better placed to attract these funds than the countries without these. There has been significant investment into research capacity building (RCB) in the Pacific Islands by ways of funding and in international research collaborations [3,13-15]. For example, the WHO programme, STEPwise approach to surveillance of chronic diseases, was designed to assist capacity building, but this aim was not realized in most Pacific Island states [10]. The Solomon Islands have however been successful in utilizing a well-funded malaria research programme to develop a wider research capability [16] and other research capacity initiatives [17].
There are Pacific solutions to some of the challenges. The Cook Islands is reliant on NZ institutions for ethics advice. Collaborations across borders between well developed research systems and the not so well developed may provide the capacity needed. Fiji, although lacking in areas, has shown leadership in sharing research expertise between its medical school/research institutions with other Pacific nations. Not all components of a health system need to be developed where resources are constrained. Countries however need to be aware of where the gaps lie and identify areas where they can share expertise with other Pacific countries and Pacific-rim countries such as Australia and NZ. Since all six countries have health plans, they should be encouraged to add a section entitled “health research plan”. The lack of a health research plan with research priorities jeopardizes a country’s ability to control the direction of research relevant to its priorities and may hinder its ability to attract necessary research funding [18]. The Pacific Health Research Council, which has been inactive since 2007, needs to be revived to coordinate assistance where needed. An alternative to developing a NHRS is to set up research or tertiary institutions, which can be encouraged to lead the development of a “micro-health research system” [12] which could evolve into a NHRS when the country’s research capacity improves.
A limitation of our study is that the informants may not have been aware of research developments that had not been communicated by a few policymakers. There was also the possibility that the informants may have “overplayed” their country’s capability in an area. Some of the questions may not have been well understood e.g. media organizations active in dissemination was recorded as none in the Solomon Islands and Samoa. A weakness is that there was no comparison with all the other Island states of the Pacific, especially Papua New Guinea, which has the largest population and several academic institutions.
A further research systems mapping in the Pacific should be repeated within ten years to monitor progress, considering the fragile nature of research workforce numbers. However, the use of the COHRED tool or other more extensive tools is not necessary. The experience of researchers, the end-users, maybe more relevant, in addition to research systems with components defined by Pacific countries.
The paucity of quality data along with competing social and economic priorities in Pacific Island countries and territories are barriers to prioritizing scarce resources for interventions. The lack of health research in Pacific Island countries and territories reflects a wider systemic failure to develop research capacity in the Pacific region [19,20]. Recent research investment in the Pacific has relied on overseas-based funding from the Health Research Council of New Zealand and the Wellcome Trust (United Kingdom) for the Obesity Prevention in the Community (Fiji, Tonga) and the Traffic Related Injury in the Pacific (Fiji, Republic of Palau, Samoa) research projects. With a range of Pacific-relevant solutions and cadre of Pacific researchers identified, non-sustainable research funds place research initiatives to address the specific needs in the region at risk [21]. Global investment in health research has been significant, for example the Global Fund for AIDS, TB and Malaria. The contribution of health research to the achievement of the Sustainable Development Goals is established.
Better developed NHRS in Pacific Island states are associated with political stability, research leaders and associations with other more developed NHRS. There is no need in developing all the components of a NHRS in a resource-constrained setting as long as the various countries develop a Pacific solution that includes research collaborations and resource sharing with other Pacific and Pacific-rim countries.