Journal of Medical Diagnostic Methods
Open Access
ISSN: 2168-9784
ISSN: 2168-9784
Research Article - (2016) Volume 5, Issue 3
Background: Blood stream infection is a serious problem that needs immediate attention and treatment. We aim to identify the frequency of common organisms in blood culture of febrile pediatric patients so that empirical antibiotic therapy can be started timely.
Methods: This cross-sectional study was conducted in pediatric ward Civil Hospital Sukkur from 1st May 2013 to 31st October 2014. Children of both genders who are between the age of one month to 15 years admitted to the pediatric ward with a fever of > 38.0 c and with a history of fever ˃ two days and whose blood culture has been sent were included in this study. Informed consent was taken prior to enrollment. The patient’s blood culture was taken under aseptic technique. Samples were sent to microbiology lab civil hospital Sukkur. 1st culture on admission to be taken to avoid confounding with hospital-acquired the infection. The frequency of organisms grown in the culture was documented.
Results: The median age of enrolled participants was 48.5 (46.6) months, 153 (38.5%) were male and 158 (61.5%) were the female and median weight of enrolled participants was 15.9 (9.7) kg. Overall, 178 (69.3%) cases had a history of prior antibiotic use; blood cultures sent within 24 hours were 117 (45.5%) cases. Twenty-two (8.4%) cases were positive. Six were positive for Salmonella typhi cases followed by E. coli.
Conclusions: It was concluded from this study that the frequency of community acquired blood stream infection was 7.6%. Salmonella typhi, E. coli were found to be common pathogens.
Keywords: Infection; Community acquired; Blood culture; Pathogens
Bloodstream infection is a severe problem that needs immediate attention and treatment as it can lead to morbidity and mortality. Fever is often the most common reason for presentation to the hospital in developing countries. Most patients with febrile illness have selflimiting viral infections, but some have a serious bacterial infection that needs urgent and appropriate antimicrobial therapy [1] advance in blood culture technique have resulted in efficient and reliable techniques for detection of bacterial and fungal pathogens [1]. Blood stream infection is a cause of high mortality especially if caused by multidrug-resistant bacteria. Bacteriologic culture to isolate the offending pathogen and knowledge about sensitivity pattern of isolates remains the mainstay of definitive diagnosis and management of bloodstream infection. However, blood culture is time-consuming and takes at least 2 to 5 days until the identification of organism [2] one key determinant in the ultimate outcome of a patient with sepsis is an institution of early empirical and appropriate antimicrobial therapy. This is only possible with knowledge of community-acquired bacteria and their likely susceptibility to antibiotics in a given set up. There are limited reports on community-acquired bacteremia in children, particularly from developing countries. This could be due to either poor lab infrastructure or poor health seeking behavior and treatment of febrile illnesses mostly by primary care physicians without a bacteriologic diagnosis. A study done in developing countries shows 8% children had blood stream infection [3] several studies have shown that rate of isolation of pathogens from blood culture increases with the quantity of blood submitted [4]. Small study of communityacquired infections from Pakistan revealed five hundred and eight blood culture samples were positive for bacterial growth. Of these 465 (91.5%) having monomicrobial growth and 43 (8.5%) having polymicrobial growth. Among them, Klebsiella spp (24.1%) were most common amongst gram negative and staph aureus (24.1%) amongst gram positive [5]. An interesting finding in the subcontinent is the isolation of more gram negative bacteria than gram positive there is a high prevalence of enteric fever caused by Salmonella typhi and Salmonella paratyphi in Pakistan. More than 51% pediatric blood culture isolates contained S. typhi or S. paratyphi A, S. typhi alone was detected in 43% of positive blood culture. The other organisms identified were coagulase-negative Staphylococci (20%), Acinetobacter species (5.1%), E. coli (4.5%), and Pseudomona s species (11.4%) [6,7].
There are limited number of studies from Pakistan, despite the high incidence of community-acquired bacteremia and case fatality among hospitalized bacteremic children [8,9]. We aim to conduct this study to identify the frequency of common organisms in blood culture of febrile pediatric patients so that empirical antibiotic therapy can be started with bacteriology of community-acquired bacteremia. The objective of this study was to determine the frequency of community acquired blood stream infection in febrile children and to identify the commonly isolated organisms.
This cross-sectional study was conducted at pediatric ward off civil hospital Sukkur from 1st May 2013 to 31st October 2014. Children of both genders who are between the age of one month to 15 years admitted to the pediatric ward with recorded temperature of > 38.0 c and with a history of fever more than two days and whose blood culture has been sent. Neonates, post-surgical patients, patients on chemotherapy and on antibiotic therapy, children with congenital anomaly, those children who have central line for antibiotic administration over long periods, children who are referred from another hospital or health care center for further management.
Cases diagnosed with HIV and tuberculosis, and children of prolonged course of prophylactic antibiotics for any associated comorbid condition like repeated UTI were excluded. Communityacquired bacteremia was defined as bloodstream infection with the growth of pathogenic bacteria in a blood culture obtained within first 48 hours after admission in febrile children between the age of 01 months to 15 years. Children who fulfilled study criteria were enrolled in the study after taking informed consent was taken from the parents. The demographic information of patient was taken on structured proforma by the investigator.
The patient’s blood cultures were performed in microbiology lab according to standard guidelines at civil hospital Sukkur. 1st culture on admission to be taken to avoid confounding with hospital-acquired the infection. The culture was followed by the primary researcher. The frequency of organisms grown in the culture was documented.
Non-probability consecutive sampling was done. The frequency of bloodstream infection in febrile pediatrics patients is 8%, considering the bond on the error of estimation of 3% and 95% confidence interval the estimated sample size was 257. Data was analyzed using SPSS version 20 (SPSS Inc. Chicago, IL, USA). All quantitative variables like age, weight, were expressed as median (interquartile range).
Qualitative variables like gender, commonly isolated communityacquired bloodstream organisms, and history of prior antibiotics were expressed in percentages. Chi-square or Fisher exact test was used to compare categorical variables and Man-Whitney U test was used to compare median age and weight. Effect modifiers like age, gender, weight and history of prior antibiotics were stratified to see their effect on the final outcome. The study is approved by ethical review of the institute (Figures 1 and 2).
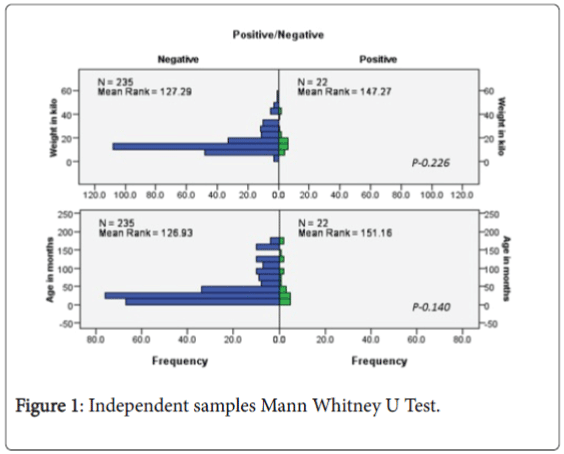
Figure 1: Independent samples Mann Whitney U Test.
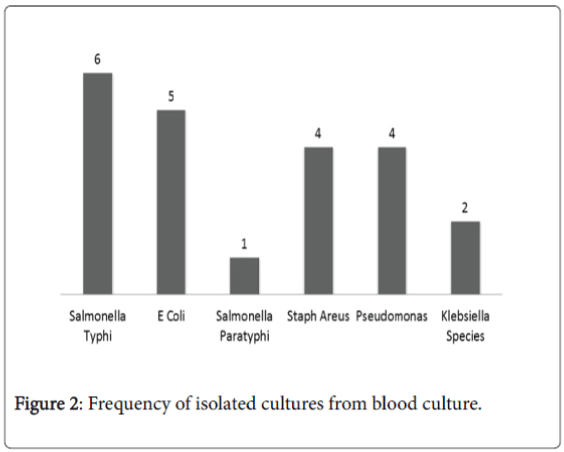
Figure 2: Frequency of isolated cultures from blood culture.
A total of 257 patients were enrolled in this study during the study period. The median age of enrolled participants was 48.5 (46.6) months, 153 (38.5%) were male and 158 (61.5%) were the female and median weight of enrolled participants was 15.9 (9.7) kg. Overall, 178 (69.3%) cases had a history of prior antibiotic use; blood cultures sent within 24 hours were 117 (45.5%) cases. Twenty-two (8.4%) cases were positive. Six were positive for Salmonella typhi cases followed by E. coli . Comparative analysis is shown in Table 1 and stratified analysis summarized in Table 2. Stratified analysis showed, of children <30 months of age, 10 (6.5%) had positive blood culture compared to 12 (11.5%) cases among children of age ≥ 30 months (p>0.120); of female children, 10 (10.1%) had positive blood culture compared to 12 (7.6%) cases among male children (p>0.079); of children weigh <13 kg, 10 (6.4%) had positive blood culture compared to 12 (11.9%) cases among children weigh ≥ 13 kg (p>0.138) and of children with no history taking antibiotics prior to culture, 17 (21.5%) has positive blood culture compare to 5 (2.8%) cases children who had history of taking antibiotics prior to blood culture.
| Negative blood culture (n=235) | Positive blood culture (n=22) | Total | |||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Age Months (Mean) | 42.6±4.7 | 61±5.5 | |||
| less than 30 months | 143 | 60.9% | 10 | 45.5% | 153 |
| More than 30 months | 92 | 39.1% | 12 | 54.5% | 104 |
| Gender | |||||
| Male | 146 | 62.1% | 12 | 54.5% | 99 |
| Female | 89 | 37.9% | 10 | 45.5% | 158 |
| Weight kg (Mean) | 10.2±10.2 | 15.1±9 | |||
| Less than 13 kg | 146 | 62.1% | 10 | 45.5% | 156 |
| More than 13 Kg | 89 | 37.9% | 12 | 54.5% | 101 |
| Blood sample taken | |||||
| Within 24 hr | 97 | 41.3% | 20 | 90.9% | 117 |
| 24-48hr | 138 | 58.7% | 2 | 9.1% | 140 |
| History of antibiotic use | 173 | 73.6% | 5 | 22.7% | 178 |
Table 1: Comparison of baseline characteristics between children with positive or negative blood culture.
| Blood culture | Age | Gender | Weight | Prior use of antibiotics | ||||
|---|---|---|---|---|---|---|---|---|
| less than 30 months | More than 30 months | Female | Male | Less than 13 kg | More than 13 Kg | No | Yes | |
| Negative | 143 | 92 | 89 | 146 | 146 | 89 | 62 | 173 |
| 93.5% | 88.5% | 89.9% | 92.4% | 93.6% | 88.1% | 78.5% | 97.2% | |
| Positive | 10 | 12 | 10 | 12 | 10 | 12 | 17 | 5 |
| 6.5% | 11.5% | 10.1% | 7.6% | 6.4% | 11.9% | 21.5% | 2.8% | |
| Total | 153 | 104 | 99 | 158 | 156 | 101 | 79 | 178 |
| p>0.120 | p>0.316 | p>0.079 | p>0.001 | |||||
Table 2: Stratified analysis by age, sex, weight and prior use of antibiotics.
Febrile illness is a leading reason for admission to hospital in Pakistan [10-12]. Despite the major contribution of infectious diseases to hospital admission, the availability of diagnostic microbiology services for bloodstream infections other than malaria is often limited by cost, infrastructure, and personnel constraints [11] consequently, health-care workers must often rely on syndrome-oriented empirical approaches to treatment and might underestimate or overestimate the likelihood of certain diseases, risking poor clinical outcomes and the promotion of antimicrobial resistance [12,13] understanding the causes and prevalence of community-acquired bloodstream infection, which is associated with high risk of death, can inform efforts to improve health outcomes in Pakistan and promote the meeting of millennium development goals for the reduction of child mortality, malaria, and tuberculosis.
Blood cultures are vital for recognizing pathogens causing severe infections and in leading appropriate antibiotic therapy. Furthermore, they remain the standard method for identifying bacteraemia in the assessment of sick patients [14] inappropriately; blood culture contamination is a common event and may lead to confusion regarding the significance of a positive blood culture. The most common contaminants are coagulase-negative staphylococcus species which are also becoming more prevalent as a primary pathogen in immunocompromised patients and in patients with indwelling intravascular devices [9,15] the uncertain clinical significance of potential contaminants leads to longer hospital stays, unnecessary antibiotic therapy, and additional laboratory testing; as a result, the cost incurred by a hospital is many times that incurred by the laboratory.
In this study 184 patients were enrolled during the study period with a median age of 48.52±46.6 months, the majority was females’ 59.8% and median weight of 15.9±9.7 kg. Overall, 118 (64.1%) cases had a history of prior antibiotic use blood cultures sent within 24 hours were 175 (95.1%) cases. Fourteen (7.6%) cases were positive. In our study Salmonella, enteric serotype typhi was the most common bacterial pathogen accounting for 4.9% of cases followed by E.coli and Pseudomonas spp. Similar findings had been reported in the systemic review where salmonella is most common pathogen isolated.
In another study from Cambodia, it was reported that salmonella is most common infection followed by E.coli [15].
We also did a stratified analysis of positive blood cultures based on age and weight. We did not found statistically significant difference across strata. Children <30 months of age, 5.4% had positive blood culture compared to 9.9% cases among children of age ≥ 30 months (p>0.191) and children weigh <13 kg, 5.7% had positive blood culture compared to 10.5% cases among children weigh ≥ 13 kg (p>0.138).
There are some important limitations to this study. We examined hospital-based cohorts to define community-acquired bloodstream infections, and thereby might have included patients with more severe illness and included only those who have access to health-care facilities.
This study presents a strong case for the importance of considering bloodstream infections in patients admitted to civil hospital Sukkur, particularly those with fever. Our findings underscore the importance of continuous re-evaluation of who's integrated management of childhood illness and other empirical treatment algorithms for febrile illness in view of changing patterns of disease. When used, empirical treatment with antimicrobial drugs should include coverage for gramnegative, especially against Salmonella, E.coli and Pseudomonas .
It was concluded from this study that the frequency of bloodstream infections was 7.6%. Salmonella typhi, E.coli , and Pseudomonas were found to be common pathogens. No relationship of positive blood culture or pathogen was found with age, weight, and gender.