Medical & Surgical Urology
Open Access
ISSN: 2168-9857
ISSN: 2168-9857
Case Report - (2018) Volume 7, Issue 4
Keywords: Prothrombin complex concentrate; Anticoagulation reversal; Left ventricular assist device
Recipients of left ventricular assist system (LVAS) require long-term anticoagulation with warfarin to prevent thromboembolic complications. Management of these patients is complicated by the frequent need for procedures and concomitant risk of bleeding, which may require rapid anticoagulation reversal [1]. We discuss a successful case of the use of four factor prothrombin complex concentrate (4FPCC) for warfarin reversal in a patient with a HeartMate 3 LVAS requiring robotic assisted laparoscopic prostatectomy.
A 66-year-old male with a history of hypertension, chronic kidney disease, non-ischemic cardiomyopathy (left ventricular ejection fraction 20%) and end-stage heart failure underwent HeartMate 3 LVAS implantation as destination therapy. Active prostate cancer was felt to be a contraindication to heart transplant listing as posttransplant immunosuppression may promote unchecked tumor growth. Life-expectancy is also a consideration given the limited supply of donor hearts. He was diagnosed with clinical stage T1cN0MO Gleason score 6 (3+3) tumor with a PSA of 5.02; final pathologic stage was pT2Nx. Definitive cancer treatment was recommended to allow for heart transplant. Therefore, he underwent a laparoscopic radical robotic prostatectomy with bladder neck suspension. As thromboprophylaxis for mechanical circulatory support, he was on warfarin with a target international normalized ratio (INR) of 2-3 (reference range 0.9-1.1) and aspirin 325 mg daily which was continued without interruption. The INR the morning of the procedure was 3.2. He received 29 units/kg of 4F-PCC (total dose 2302 units; weight 79.1 kg) to achieve a goal INR ≤ 1.4, per surgeon’s recommendation. One-hour post 4F-PCC infusion, the INR was 1.4, and surgery commenced approximately 1.5 hours after the 4F-PCC dose. The surgery lasted 3.5 hours. There were no complications or need for blood transfusions. An INR checked immediately prior to extubation was 1.5 (approximately 5 hours post 4F-PCC dose). The INR was back within the target range of 2.0-3.0 by 23 hours post 4FPCC administration, avoiding the need for an intravenous (IV) anticoagulation bridge (Figure 1).
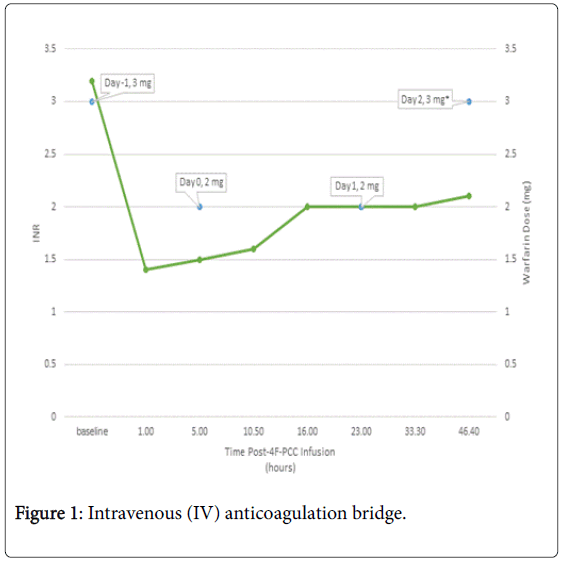
Figure 1: Intravenous (IV) anticoagulation bridge.
Minor bleeding was observed within the first 72 hours at the surgical site without hematuria. No intervention or transfusion was required. The patient was discharged 48 hours post-procedure with an INR of 2.1. Follow-up at 30-days revealed no major bleeding events. Mild hematuria was reported 5 days post-operatively, though acceptable per urology given the high bleeding risk associated with the procedure, and did not require blood transfusion or interruption in anticoagulation. No pump-thrombosis, elevations in lactate dehydrogenase or free hemoglobin, or thrombotic events were observed (Table 1).
| LDH Value (ref. 135-225 U/L) | |
|---|---|
| Pre-4F-PCC | 205/237 |
| 22 h post-4F-PCC | 190 |
| 46 h post-4F-PCC | 215 |
| 8 days post-4F-PCC | 241 |
| 35 days post-4F-PCC | 204 |
Table 1: LDH values post 4F-PCC dose.
Since the approval of 4F-PCC, use in the LVAS population has continued to increase, with most data supporting use in heart transplantation. In a retrospective analysis, 32 patients who received 4F-PCC for warfarin reversal prior to hear transplant had a decreased time to chest closure and required less blood products, without any observed thromboembolic complications or increased rate of death compared with 42 patients who did not receive 4F-PCC [2].
Data for the use of 4F-PCC in LVAS patients for both urgent and elective procedures are limited, with no reports of prostatectomy procedures. There is one case report of robotic assisted laparoscopic radical prostatectomy in an LVAS patient in which warfarin was held for two days prior to surgery and the patient was started on heparin 5000 units subcutaneous every six hours; aspirin was continued. The patient’s INR was 2.0 at time of surgery. In this case, there was difficulty maintaining hemostasis during dissection due to continued blood oozing from surgical planes extending the operative time (total operative time was 400 minutes and estimated blood loss was 300 mL). Despite this, urologists observed no post-operative complications and the patient were discharged home on post-op day 8 [3].
The use of 4F-PCC in this population is an attractive strategy that offers more rapid INR correction, smaller volume of infusion, and predictable reversal time compared with fresh frozen plasma and/or vitamin K administration, and avoid the need for pre-operative bridging. Bleeding rates with open robotic prostatectomy procedures have been reported to be as high as 1%-3% due to the rich blood supply to the prostate and the adjacent Santorini’s plexus; this procedure is associated with significant blood loss even in patients with normal coagulation profiles [4-6]. Rozet et al. compared patients undergoing extraperitoneal robotic assisted laparoscopic prostatectomy (RALP) and extraperitoneal laparoscopy radical prostatectomy (LRP) and found the transfusion rate to be higher for the RALP group, with rates of 9.8% and 3%, respectively [7]. In our patient, warfarin was continued, however 4F-PCC administration 30 minutes prior to surgery decreased the INR from 3.2 to 1.4, while allowing for a fast rebound to 2.0 at 23 hours post 4F-PCC as the effects of factor VII in the 4F-PCC wore off to obviate the need for IV bridging. This practice has become our standard approach for LVAS patients. Previously we completed a retrospective analysis of 37 patients with LVAS to evaluate the safety and efficacy of 4F-PCC (mean dose 22 units/kg) for warfarin reversal during bleeding episodes or prior to elective or urgent procedures. In this analysis, we did not observe any confirmed or suspected pump thrombosis or arterial/ venous thrombotic events [8].
LVAS patients frequently undergo procedures and require lifelong anticoagulation, thus providers are frequently in the position of making the best peri-procedural plan for these patients. The utilization of 4F-PCC in this population can facilitate continuation of therapeutic anticoagulation without the need for peri-procedure bridging, resulting in a decreased risk of bleeding and decreased hospital length of stay. Instead of holding warfarin and bridging with low molecular weight heparin in the outpatient setting, the use of 4F-PCC immediately prior to the procedure allowed the patient to remain therapeutic on warfarin and be discharged 2 days post-operatively.
In this report, we described the use of four factor prothrombin complex concentrate (4F-PCC) for temporary warfarin reversal in a patient with a Heart Mate 3 LVAS requiring robotic assisted laparoscopic prostatectomy. This approach is attractive for both patients and providers given the possible impact on quality of life, care, shorter hospitalization, and potential cost savings.