Gynecology & Obstetrics
Open Access
ISSN: 2161-0932
ISSN: 2161-0932
Research Article - (2018) Volume 8, Issue 3
Background: Ethiopia is a country of long-standing history with its own identity. It is also a country with many useful traditional practices. On the other hand, it is a country where harmful traditional practices commonly practiced during pregnancy, labor delivery, post-natal.
Objective: The aim of this systematic review was to identify common folk practices during childbirth and reasons for committing this practice in Ethiopia, 2017.
Methodology: Systematic review was conducted using a priori protocol prepared specifically for this review. Articles were retrieved through a comprehensive search strategy. Data were extracted using critical appraisal check list.
Results: A total of 173 articles were identified, of which 10 were included in the review after full evaluation. The findings were presented under sub headings as folk practice: During pregnancy: priority for first pregnancy, not talking about it at early age, not buying items for baby until delivery, food taboos like: food items that are white in color, vegetables, fruits, meat in some circumstances and sugarcane. During Labor and Delivery: Hanging experienced women near the laboring mother, not allowing men to be involved in the delivery process, sex preference, birth by shock and dancing, applying butter on abdomen, Bush Birthing, opening belts, opening all closed items in the house hold. During postnatal period: funeraling of placenta, “Gubbifachuu”, “Arguugaa eelmachuu” milking the cows for three consecutive days, giving water and/or milk right after delivery, washing newborn, staying with clothes dressed during delivery, not initiating breastfeeding up until the cord cut off, placing the butter on the cord, not tying cord, “Ulumaa taa’uu”, not to touch the new born baby, Mingi, Lanka Mansat.
Conclusion: There is strong evidence that Ethiopian women are practicing various cultural practices during child birth process. Therefore, we recommend context specific intervention to avert maternal and newborn complications/deaths related to this folk practices.
Keywords: Ethiopia; Folk practice; Pregnancy; Childbirth; Post-natal
Antenatal care; EDHS: Ethiopia and Demographic Health Survey; EJHD: Ethiopian Journal of Health Development; EJRH: Ethiopian Journal of Reproductive Health; FMOH: Federal Ministry of Health; HEW: Health Extension Worker; HSDP: Health Sector Development Plan; MCHIP: Maternal and Child Health Integrated Program; MDG: Millennium Development Goal; MMR: Maternal Mortality Ratio; SBAS: killed Birth Attendant; SMI: Safe Motherhood Initiative; TBA: Traditional Birth Attendant; WHO: World Health Organization
Culture is socially acquired and transmitted or shared characteristics of a given group, community and nation which can affect the health of the individual in several ways [1]. Ethiopia is the tenth largest country in Africa. The country is agrarian and its economy depends on subsistence agriculture. Approximately 85 percent of the population lives in rural areas and the settled population is scattered, which makes delivery of health service difficult. It’s a diverse country with over 80 cultural and nearly 80 languages [2].
It is also a country with many useful and promotional traditional practices like breast feeding, post-natal care, social gathering such as “Eder”, “Shengo”, “Ekub”, caring for the aged person, children and religious leaders [3].
On the other hand, it is a country where harmful traditional practices such as types of food eaten and method of their preparation, child bearing practices, handling of children and aged person, and other values that hold peoples together and give them a sense of identity and distinguish them from other group [3,4]. For instance, women, especially in rural areas, work for more than 12 h in a day in the field of agricultural work, marketing, labor work and different home work during their pregnancy, breast feeding and PNC time, food taboos, herbal drug usage, abdominal massage and hardworking during pregnancy and child birth [5].
According to the World Health Organization (WHO), more than half of births in developing nations are attended by traditional birth assistance with little knowledge of anatomy and physiology. Usually they use harmful treatments during delivery. For example, in case of obstructed labor, they massage the abdomen by pressing to force the baby out, delay of delivery is believed to be a punishment for marital infidelity and put the pregnant woman at high risk of death [6].
Particularly in Ethiopia there are practice like massaging the abdomen before and during delivery, shaking a woman in prolonged labor, isolation during delivery and after delivery, suturing the vagina after delivery, drastic measures to hasten the expulsion of the placenta, inducing sneezing to force out after birth, taking bitter anti-helminthes drug during pregnancy and only 28% of delivery assisted skill birth attendant and6% delivered alone without any assistance [7].
Maternal and perinatal mortality and morbidity levels are key indicators of the public health situation in a country [8]. The Safe Motherhood Initiative (SMI) was launched 15 years ago with the aim of reducing high maternal mortality, particularly in poor countries. Maternal health care was identified as a priority. Despite this initiative, maternal mortality remains very high in low-income countries, and lack of access to maternal care facilities is a further contributing factor [9].
Ethiopia has one of the highest maternal mortality ratios (MMRs) in the world which is 412 maternal deaths per 100,000 live births in the 2016 Ethiopian Demographic Health Survey [10]. Despite an effort to expand coverage of health services, Ethiopia has struggled to improve its maternal health indicators [11]. Not surprisingly, the country’s high MMR is associated with a lack of adequate access and continued under-utilization of modern health services, and many studies also indicated as cultural barriers have been found to be a significant determinant, particularly related to facility-based delivery [12].
What are the common folk practices during childbirth and what are the reasons for undertaking such practices in Ethiopia?
Objective
The aim of this systematic review was to identify common folk practice during childbirth and reasons for undertaking these practices in Ethiopia.
Methodology
A mixed-method systematic review was conducted using a prospective protocol prepared specifically for this purpose and reported using the checklist proposed by the Meta analysis of JBI for reporting of systematic reviews.
Criteria for inclusion and exclusion of studies.
Inclusion criteria
The studies were included in the review and analyses if they met the following criteria:
Types of studies: All articles or research involving culture and maternal health care. Studies that used any design such as cohort, cross-sectional, or case control, international studies that addressed the relationship between folk practice during child birth and associated reasons, in Ethiopia ,adjusted their results for at least socioeconomic status (occupation, educational level, income, housing, or other variables), reported odds ratio (OR) or relative risk estimates and 95% confidence intervals (CIs) or data to calculate them, contained the search phrase in title or abstract, full text was available and written in English language were included in case of the quantitative.
Participants/Populations: Articles that generated the data from health care utilizers, and health care providers, patients and managers; and articles that used secondary data (like patient card review) were considered for this review.
Types of interventions: Any hospital or health institutions or community based studies that aim to assess folk practice during childbirth.
Comparison: We had no case and control group; our aim was to see the folk practice during childbirth and the justification behind in Ethiopia.
Types of outcome measures: The main outcomes of our interest are: any folk practice during childbirth and justification behind this practice.
Time and Place: Both published and unpublished report, conducted in Ethiopia were considered without time limitation.
Search strategy
A combination of search terms were employed to find relevant studies in MEDLINE, EMBASE, ECLA, POPLINE, CINAHL, LILACS, and Google scholars, Initial search was executed using a key word such as traditional practice; cultural practice; child birth; pregnancy, traditions and beliefs; culture and childbearing practice, reproduction and tradition; determinants and maternal health service Ethiopia; socio-cultural barriers and maternal health Ethiopia; gender norms Ethiopia; family influence and maternal services. In the case of studies discussing more than one outcome, each outcome was considered independently. To find unpublished studies, we contacted relevant researchers in the field.
Study selection and quality assessment
The title and abstract of each article was screened for inclusion by four independent reviewers. Full text articles were reviewed by two independent reviewers using pre-sated inclusion criteria.
The quality of the qualitative studies was assessed using an adaptation of the Critical Appraisal Skills Programme (CASP) qualityassessment tool (http://www.casp-uk.net) and assessment included the following domains: aims, methodology, design, recruitment, data collection, data analysis, reflexivity, ethical considerations, findings, and research (Table 1). The quality of the quantitative studies was assessed using an adaptation of the STROBE https://www.strobe.
| Source | Setting/Region | Study design | Sample Size | Main Findings |
|---|---|---|---|---|
| 2007 | Ethiopia: Benishangul Gumuz | Cross sectional: qualitative | 57 | Food prohibition during pregnancy, Abdominal massage Son preference at birth, Shaking a woman in prolonged labor, Isolation during delivery and after delivery Suturing the vagina after delivery Inducing sneezing to force out after birth |
| 2017 | Ethiopia: Oromia | Mixed method design | 1598 | Abdominal massage, cutting cord, Son preference at birth, Burying of placenta, Distance and availability of the service, Sex Preference, Birth positions |
| 2014 | Ethiopia: SNNP | Cross sectional: qualitative | In depth | Preference of traditional medicine, Placental care, Abdominal massage |
| 2012 | Ethiopia: Afar | Cross sectional: quantitative | 295 | Food prohibition during pregnancy |
| 2012 | Ethiopia: Oromia | Cross sectional: quantitative | 295 | Food prohibition during pregnancy |
| 2014 | Ethiopia: Amhara | Cross sectional: qualitative | 2FGD KII |
Immediately bathing then dry the newborn, Lanka mansat, pre-lacteal feeding |
| 2013 | Ethiopia: SNNP | Mixed: cross sectional | Q=909, 3FGD 3 IDI |
Burying of placenta, Applying butter on the abdomen |
| 2015 | Ethiopia Southwest: Oromia | Cross sectional | 312 | Cultural malpracticesduring pregnancy: food taboos, abdominal massage , home delivery, cutting cord by uncleanblade, avoiding, colostrum, washing baby immediately after delivery |
| 2012 | Ethiopia: Afar | Cross sectional: qualitative | 21- In depth 6 FGD |
Effect of Cultural practices on positive health seeking behaviour practices |
| 2016 | Ethiopia: South Gondar | Cross sectional: quantitative | 355 | Not tying cord after delivery, Abdominal massage during pregnancy, Food prohibition during their pregnancy. |
Table 1: Description of studies included in the analysis.
Data extraction and management
Data was extracted using a standardized form including the following domains: study setting, sample characteristics, objectives, design, data collection and analysis methods, and conclusion. Themes, findings, and participant quotations was extracted from qualitative studies. Data source, outcome measures, and results were extracted from quantitative studies. We designed a form to extract data. It was extracted using the agreed form and the discrepancies were resolved through discussion.
Data analysis
Quantitative: As it is not possible to present prevalence estimates due to high heterogeneity in the quantitative studies, including inconsistent identification criteria and operational definitions. Therefore, descriptions of study characteristics, outcome measures, and key findings were presented.
Qualitative: A thematic synthesis approach was used to analyze and synthesize the qualitative data. A spreadsheet was created of all qualitative data extracted from the studies’ findings sections, and thematic analysis methods was used.
Description of studies
We identified 173 articles. After removing duplicates and citations reported on other outcome measures which were 97. Seventy-six were considered for further evaluation. Out of this, 76 articles were considered for full-text evaluation, sixty six of these studies were excluded and 10 studies were included in the final report (Figure 1).
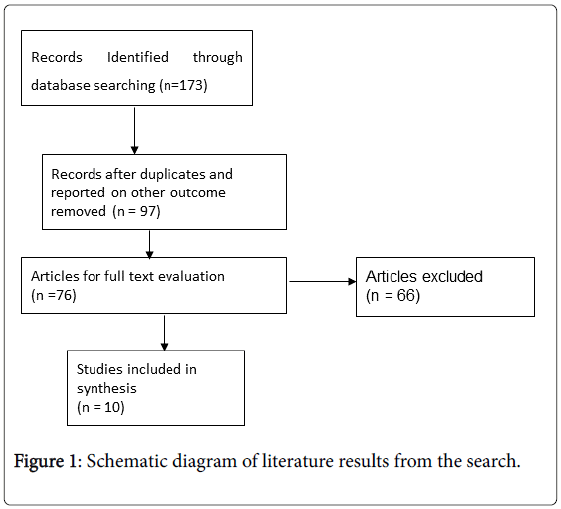
Figure 1: Schematic diagram of literature results from the search.
Key findings
The key findings were presented under three sub headings as during pregnancy, labor-delivery and post-natal.
During pregnancy
Culture is generally considered as a blessing and a positive life event. During pregnancy there are diverse cultures to be practiced in different part of Ethiopia which may have positive or negative implications like going to parents' home at eighth month to prepare for the birth if the pregnancy is the first, not talking about it until the woman starts to show, believing if talking about abortion might be there, not purchasing items for the baby until it is born and gender is known otherwise considered as bad luck [1,13].
Food taboos are common and the best and most nourishing portions of the food are served to the men. Pregnant and lactating women are restricted from certain food staffs like: food items that are white in color (such as milk, fatty meat, porridge, potato, and banana), vegetables, fruits, meat of hunted animals, eggs, meat of animals slaughtered by their husband's clan, and sugarcane. They believe that these food items which are white in color were surfaced on the body of the baby and cause labour difficulties, also they (white in color) produce offensive uterine fluid (amniotic fluid) during delivery, the green vegetables, like green peppers are believed to causes a bad odor in both the mother and the baby, make the newborn baby bald and if women eat meat of hunted animals they will get sick, their body (arms and legs) will be injured, there might be abortion, obstructed labour [1,6,12,14-16].
Abdominal massage
This is also common in attempt to facilitate labour, to correct malposition of the foetus, uterine massage during 2nd stage of labour and kneading and squeezing women abdomen with intention of inducing labour [3,14,16,17].
During labor and delivery
Hanging experienced women around the laboring mother and pretending as if they are also in labor and encouraging the woman in labor to push, not allowing men to be involved in the delivery process, gathering the women outside the home to pray, way of broadcasting the arrival and sex preference (five times to announce a boy; seven times to announce a girl), inducing birth by shock (firing shots from the woman's room)when the labors prolonged, dancing to induce labour, tying of the cord to her leg to prevent the cord and placenta from slipping back into the uterus, applying butter on abdomen : to relief her from pain during contraction and to accelerate delivery process ,pressing jar down on the abdomen until all the remains placenta are discharged, Bush Birthing “Hidhaa buufachuu”(opening belts)“Waantoota qadaaddii/kiddooqaban/waantootahidhamanii mana keessajiranmarabubuqqisuuyknhiikuu” - opening all tied/closed items in the house hold [1,3,4,6,15-18].
Cultural practices during postnatal period
Funeral of placenta “Obbaatii Marsachuu”: thinking as the placenta is the main part of the neonate without which the neonate exists, ifthisprocess is not under taken the newborn not stay with his family when grew up. “Gubbifachuu”: tyingpieces of sheet on head immediately following the delivery of the newborn by the father of newborn which show his wife delivered. ”Arguugaa eelmachuu” milking of the cows for three consecutive days by the father of newborn, “Eerbee Fannisuu“ flagging of flag at indoor which is sign of boring male neonate, Giving water and milk: Right after delivery providing water if the born neonate is male and milk for female, Washing newborn right after delivery, staying with clothes dressed during delivery, not washing bodies and initiating breast feeding up until the cord cutoff, placing the butter on the cord right after delivery and for 3 to 4 days, nottying cord, rests in the house for 49 days after the birth, not allowing the husband to see his wife from birth up to the next twelve days, not to touch the new born baby except the mother for the first month, Mingi (killing the child right after birth or later in life), Lanka Mansat (applying mild pressure inside the baby’s mouth on the soft palate using index finger which is made wet using a mixture of warm water and a local herb called ‘ersho’ or honey) [1,6,15,16,18].
The intention of this review was to identify common folk practice during birth. The findings evidently suggest that diversity in folk practices during birth which are different in terms of their manifestation, content, time and duration. These difference probably reflected by the diverging underlying explanations cited .For example, believing some food items as if they cause labour difficulties, produce offensive amniotic fluid during delivery, bad odor in both the mother and the baby, hanging experienced mother around the laboring mother, pretending as if she also in labor to encourage her to push, dancing and shooting the fireto induce labour, thinking as if applying butter on abdomen relief contraction pain making the muscle relaxed [1,6,15,18].
Folk practices during birth are usually undertaken in the belief that these practices have a protective effect on birth process and future. This may due to unavailable mechanism for disconfirmation of traditional beliefs that they engaged in these rituals as skepticism when they encountered pain or complication actually or later on in life.
From a Western medical outlook, some rituals may indeed have beneficial health effects, such as ensuring adequate rest, privacy, support and nutrition. However, there is a lack of evidence linking folk practices during birth. From a psycho-socio-cultural viewpoint, folk practices may serve multiple functions and they may also be seen as a sign of respect for certain religions or traditions, and in some cases, as a status symbol.
Finally, an individual may have multiple cultural and/or religious identities, as well as personal, idiosyncratic beliefs, leading to further variations of practice. Therefore, physicians, nurses, midwives and other allied healthcare professionals need to have awareness of and knowledge about these practices that can avoid causing undue distress to those receiving care about their wishes regarding folk practices and negotiate a mutually agreeable care plan, which may extend beyond the hospital stay.
There are several limitations to this review. These are limited to English literature. There may be pertinent information that is published in other languages. Not all cultural groups are uniformly represented due to the accessibility of studies, reflecting the need for additional research. It is very likely that cultures not described in this review also have folk practices that have not yet been described in the English-language. It is key to reiterate the care against over generalization of cultural practices of given culture based on accessible information, which is derived from studies conducted in particular regions at a particular point in time lead to substantial inconsistency in practice.
Ethiopia has much common cultural malpractice during prenatal delivery and postnatal periods.
Pregnancy in Ethiopia culture is generally considered a blessing and a positive life event. For women, pregnancy is a time in which their status remains uncertain until they are able to give birth to their first baby and prove that they are fertile. It is well recognized that Pregnancy is viewed as a critical period in the life of women and is usually subjected to a number cultural practices as a way of safeguarding their lives.
Ethiopian, women are helped through pregnancy by their mothers and other female family members, friends and neighbors.
Scientific literature provides strong evidence of cultural practices during a period of pregnancy delivery and after delivery like food taboo, cord cutting by unsterile material, not to tie cord, abdominal massage, bush birthing practice, Barring of placenta around the home, immediate bathing and drying, avoid exposure to wind, and sun, mingi and lankamansat.