Advanced Techniques in Biology & Medicine
Open Access
ISSN: 2379-1764
ISSN: 2379-1764
Research Article - (2016) Volume 4, Issue 1
Carbonic anhydrase is a key enzyme for initiating the crystal nucleation, seen as “the central dark line” in the crystal structure in calcified hard tissues such as tooth enamel, dentin and bone. Both estrogen deficiency and fluoride exposure adversely affected the synthesis of this enzyme in the calcifying hard tissues. This led to the notion that fluoride exposure might increase the risk of developing osteoporosis in postmenopausal women. Using ovariectomized rats, which represent an estrogen (Es)-deficient state, as an animal model of postmenopausal women, we examined the causal relationship between fluoride (F) exposure and risk of developing osteoporosis. Two groups of rats, an Es-deficient group and a non-Es-deficient group, were administered free drinking water containing F ions (1.0 mg/L). Two other groups, an Es-deficient group and a control-group, were administered tap water. Soft X-ray radiography demonstrated a significant increase of radiolucent areas in the calvaria of the combined Esdeficient plus F group compared to that in the other experimental groups. Electron microscopy revealed an increase of amorphous minerals in the radiolucent areas. Light microscopy demonstrated that combined effects evidently of Es-deficiency and administration of F caused deterioration of the rat tibia with a coarse pattern of trabecular architecture, suggesting that a decline in bone formation might be the primary cause of osteoporosis. Consequently, F exposure might accelerate osteoporotic changes in postmenopausal women even at a low dose.
Keywords: Fluoride exposure, Estrogen deficiency, Osteoporosis, Soft x-ray radiography, Electron microscopy, Light microscopy
Osteoporosis is a major health problem among aging people and occurs predominantly in postmenopausal women. Various risk factors have been identified that are associated with the development of osteoporosis [1-6]. Among those factors, estrogen (Es) deficiency is well known to increase the risk of postmenopausal osteoporosis. In addition, cadmium (Cd) is a well-known chemical risk factor for osteoporosis, so-called “Cd-induced osteoporosis” [7-13]. According to our previous study, both Cd exposure and Es deficiency adversely affects the crystal nucleation process, resulting in crystal structure defects. Further, the combined effects of Es deficiency and Cd exposure were responsible for greatly increasing amorphous minerals and deceasing trabecular architecture in the bone, resulting in the development of “itai-itai disease” [13]. In the case of fluoride (F) exposure, the detrimental effect of F ions on the crystal nucleation process far exceeded that of Cd ions [14,15]. This led to the assumption that F schemes for caries prevention might leave postmenopausal women exposed to a high risk of developing osteoporosis without any beneficial effects.
By the middle of the 20th century, bone fractures and pathological bone formation by F poisoning had been reported [16,17]. Statistical analyses carried out between the late 1950s and early 1990s reported the exponential increase of osteoporotic fracture after F schemes for caries prevention were adopted around the 1940s [18,19]. This tendency is not simply explained by the increase in the proportion of elderly individuals in the population, suggesting a causal relationship between water fluoridation and the risk of bone mineral loss and fractures [20-23]. However, conflicting results have been reported [24-27], leaving the matter unsettled. Furthermore, after adopting F therapy for osteoporosis, since sodium fluoride had been first thought to have profound effects on calcium metabolism of patients with several bone diseases [28], the high-dose of F ions was found to not only increase bone mass without creating new trabecular architecture–meaning mechanically inferior bone–but also induce abnormal bone mineralization [29-33]. In contrast, a low-dose of F ions was found to increase the osteoid indices [34-36], further complicating the matter.
As part of our study on mechanism of calcification, we would like to provide a plausible explanation for these matters and raise awareness that F schemes, in particular water fluoridation for caries prevention, might accelerate the development of osteoporosis in postmenopausal women by a mechanism involving crystal nucleation.
Animals
In order to obtain Es-deficient animals, 5-week-old female Sprague-Dawley rats that were ovariectomized at the age of 3 weeks, and 5-week-old female rats without ovariectomy were purchased from Tokyo Laboratory Animals Science Co., Ltd. (Tokyo, japan). The ovariectomized rats were divided into two groups: the Es-deficient group (-Es/-F) and the combination of Es-deficient with F exposure group (-Es/+F 1.0 ppm). Similarly, rats without ovariectomy were divided into two groups: the F exposure group (+Es/+F 1.0 ppm) and the control group (+Es/-F). Rats in both the F exposure and combination (-Es/+F 1.0 ppm) groups were given free drinking water containing 1.0 mg/L F ions (NaF), while the control (+Es/-F) and Es deficient (-Es/-F) rats were given tap water. Three months later, rats were anaesthetized with ether, and samples of the calvaria and tibia were excised. Samples of the calvaria were subjected to soft X-ray analysis and transmission electron microscopic (TEM) observation, and those of the tibia were examined under a light microscope. No sample was decalcified. As a supplemental data, we tried to assess simply the combined effect of Es deficient with F exposure (-Es/+F 1.0 ppm) on the bone by comparing to that of the combination of Es-deficient with Cadmium exposure (-Es/+Cd 2.0 ppm). Three to five rats from each group were examined. The animal protocol was approved by the Animal Care and Use Committee of Meikai University.
Soft x-ray analysis of the calvaria
Rat calvaria tissues were analyzed using a soft X-ray radiography device (Sofron SRO-M50, Softex Co., Ltd, Japan) in order to compare the degree of mineralization under different experimental conditions. The samples were placed on the X-ray film cassette and exposed to soft X-rays. Soft X-ray radiography was performed at 25 kV and 3 mA for 5 min. After developing the photographic papers, each image was processed using a photo scanner (GT-9800F, Seiko Epson Co., Ltd, Japan).
Transmission electron microscopy of the calvaria and light microscopy of tibia
The samples of calvaria and tibia were fixed with 2% glutaraldehyde in a 0.1 M cacodylate buffer (pH 7.4) for 1 h at 5°C, post-fixed with 1% osmium tetroxide in the same buffer for 2 h at 5°C, dehydrated by passage through a series of ascending ethanol concentrations, and embedded in Araldite 502 resin. Sections of the calvaria and tibia were cut using diamond knives in a Porter-Blum MT2-B ultramicrotome (Sorvall, USA). Thin sections of the calvaria were examined under a JEM 100CX transmission electron microscope (JEOL Ltd. Tokyo, Japan) at an accelerating voltage of 80 kV, and thick sections of trabecular architecture beneath the metaphyseal plate of the tibia were stained with 1% toluidine blue in 30% ethanol solution and analyzed by light microscopy.
Soft X-ray radiographs have revealed that the calvaria in the control group was well-mineralized compared with that in the other experimental groups, showing entirely radiopaque (Figure 1a). Although both Es deficiency and F exposure affected the calvaria structure to a certain degree as seen by the increase of radiolucent areas (Figures 1b and 1c), the combined effects of Es deficiency and F exposure remarkably altered the calvaria structure, showing an increase of radiolucent areas, resulting in the appearance of a labyrinthine pattern as shown in Figure 1d. The combined effects of Es deficiency and Cd exposure revealed a relatively small morphological change of the calvaria equivalent to that of Es deficiency (Figures 1b and 1e).
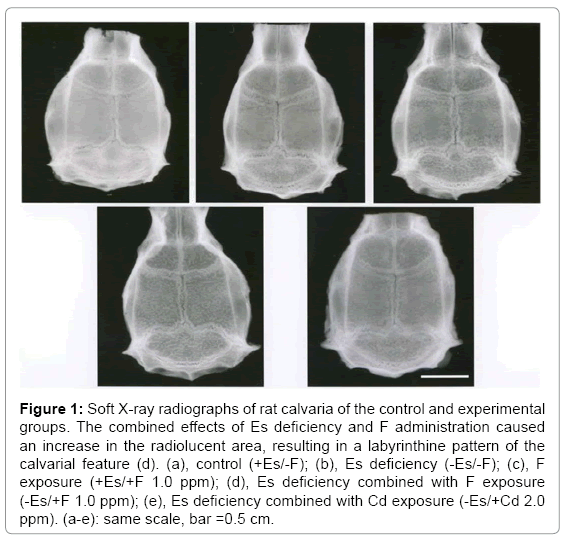
Figure 1: Soft X-ray radiographs of rat calvaria of the control and experimental groups. The combined effects of Es deficiency and F administration caused an increase in the radiolucent area, resulting in a labyrinthine pattern of the calvarial feature (d). (a), control (+Es/-F); (b), Es deficiency (-Es/-F); (c), F exposure (+Es/+F 1.0 ppm); (d), Es deficiency combined with F exposure (-Es/+F 1.0 ppm); (e), Es deficiency combined with Cd exposure (-Es/+Cd 2.0 ppm). (a-e): same scale, bar =0.5 cm.
Concerning the crystals in the calvaria of the combined group, at low magnification, electron microscopy demonstrated that the radiolucent areas of the calvaria were filled with fine needle-shaped minerals with less electron density (Figure 2c), whereas the radiopaque areas contained relatively thick and electron-dense minerals similar to those of the control (Figures 2a and 2b).
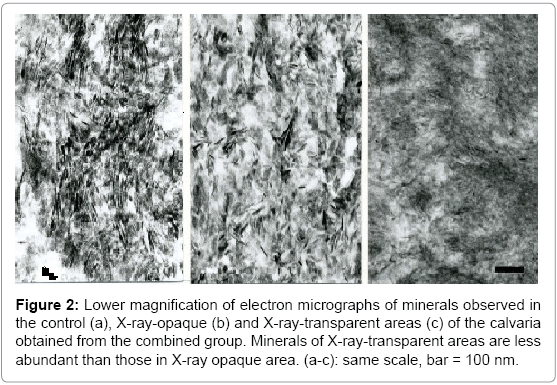
Figure 2: Lower magnification of electron micrographs of minerals observed in the control (a), X-ray-opaque (b) and X-ray-transparent areas (c) of the calvaria obtained from the combined group. Minerals of X-ray-transparent areas are less abundant than those in X-ray opaque area. (a-c): same scale, bar = 100 nm.
Higher magnification clarified crystals with proper lattice fringes in both the radiopaque areas of the combined group and the control animals (Figures 3a and 3b). However, most of these needle-shaped minerals in the radiolucent areas had ill-defined features and lacked the central dark lines (CDLs) or lattice fringes commonly observed in sound crystals, indicating that the radiolucent areas were filled with amorphous minerals (Figure 3c).
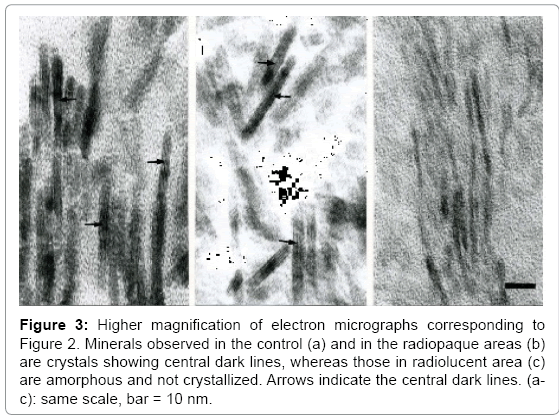
Figure 3: Higher magnification of electron micrographs corresponding to Figure 2. Minerals observed in the control (a) and in the radiopaque areas (b) are crystals showing central dark lines, whereas those in radiolucent area (c) are amorphous and not crystallized. Arrows indicate the central dark lines. (ac): same scale, bar = 10 nm.
Light microscopy demonstrated that the control rat’s trabecular architecture beneath the metaphyseal plate in the tibia was welldeveloped with a robust structure (Figure 4a). In contrast, the trabecular architecture of the experimental rats appeared thinner. In particular, it was evident that the tibia of rats with a combination of Es deficiency and F exposure (-Es/+F 1.0 ppm) had a remarkable decrease in the trabecular architecture compared to either Es deficient (-Es/-F) or F exposed (+Es/+F 1.0 ppm) rats (Figures 4b-4d). In addition, light microscopy demonstrated an alteration of the trabecular architecture with a coarse pattern and an increase of adipocytes in tibial tissues affected by the combined effects, indicative of the progress of osteoporotic change (Figure 4d). On the contrary, the combined effects of Es deficiency and Cd exposure (-Es/+Cd 2.0 ppm) on the tibia did not affect its morphological change significantly compared to the effects of Es deficiency combined with F exposure (-Es/+F 1.0 ppm) viewing from figures of 4d and 4e. There did not appear to be a significant increase in either the number of Howship lacunae in the calvaria or osteoclasts in the tibia of the combined group.
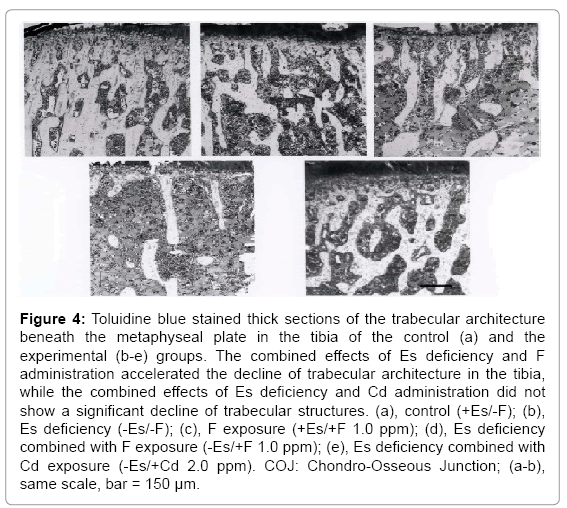
Figure 4: Toluidine blue stained thick sections of the trabecular architecture beneath the metaphyseal plate in the tibia of the control (a) and the experimental (b-e) groups. The combined effects of Es deficiency and F administration accelerated the decline of trabecular architecture in the tibia, while the combined effects of Es deficiency and Cd administration did not show a significant decline of trabecular structures. (a), control (+Es/-F); (b), Es deficiency (-Es/-F); (c), F exposure (+Es/+F 1.0 ppm); (d), Es deficiency combined with F exposure (-Es/+F 1.0 ppm); (e), Es deficiency combined with Cd exposure (-Es/+Cd 2.0 ppm). COJ: Chondro-Osseous Junction; (a-b), same scale, bar = 150 μm.
As expected, the present study has clearly shown that the combination of Es deficiency and F exposure group facilitated osteoporotic change in the bone compared to the other experimental groups. Also, it is noted that the combination of Es deficiency and F exposure adversely affected more than that of the combination of Es deficiency and Cd exposure on the bone formation, suggesting that F ions contributed to accelerate the interruption of bone formation more than Cd ions. In both the soft X-ray radiograph of the calvaria and light microscopy of the tibia (Figures 1 and 4), the osteoporotic changes observed in this study were similar to those resulting from the combined effects of Es deficiency and Cd exposure, Cd-induced osteoporosis [13]. The finding supports the epidemiological results that water fluoridation might be responsible for the increasing rate of osteoporosis in postmenopausal women [20-23]. In general, using animal models of postmenopausal osteoporosis, many researchers tend to assume that the development of osteoporosis in the ovariectomized animals is primarily due to bone mineral loss resulting from an increase in bone resorption relative to bone formation. In this study, as seen in Figures 1 and 4, soft X-ray radiography of the calvaria appeared to support the assumption of excess bone resorption by osteoclasts. Electron micrographs, however, have proven this assumption to be misconceived, because the supposed bone resorption areas were filled with amorphous minerals in the calvaria (Figures 2c and 3c). In addition, it was noted that the radiolucent areas were not created by bone absorption by osteoclasts. This finding contradict the widely accepted belief that osteoporosis is caused by excessive bone resorption by osteoclasts. From these morphological results, we speculate that a deterioration of bone formation might be the primary cause of osteoporotic change.
Although F therapy for osteoporosis has been employed based on the assumption, which could generate fluorapatite and protect against bone resorption, the complicated mechanisms and outcomes of F treatment for osteoporosis still remains unclear. The scientific justification for F therapy for osteoporosis, which induced irregular periosteal bone formation, ligament calcification, abnormal mineralization, and an increase of osteoid formation [29-36], is as follows: Concerning the high dose of F treatment, the increase of bone mineral density might be attributed to the pathological mineralization seen by an abnormal calcification and the presence of large crystals located outside the collagen fibrils [16,17,35,37]. This occurs because a high content of F ions absolutely inhibits the synthesis or activity of certain enzymes such as enolase and carbonic anhydrase [13,14,38-42]. This might be fatal to cellular metabolism and eventually lead to pathological calcification, which might be similar to the vascular calcification accompanying cellular degeneration [43]. On the other hand, the increase of osteoid caused by the relatively low dose of F treatment may be interpreted as an increase of amorphous minerals due to the failure of crystal nucleation observed in the present and the previous studies [13,14,43].
Regarding whether F ions replace OH in hydroxyapatite in tooth enamel, dentin and bone, the recent findings obtained from Raman microprobe analysis clearly clarified that the incorporation of F ions into the lattice structure of apatite crystal never occurs in calcified hard tissues [15]. This is because F ions are only able to incorporate into the crystal structure through the precursor-octacalcium phosphate (OCP)– mediated pathway, which differs from the CDL pathway, meaning that acid-resistant fluorapatite is never created in tooth enamel by F intake [15]. Regarding this purported phenomenon of acid resistance of fluorosed enamel, their crystals show voids in the centers similar to those of caries lesions; therefore, the acid resistance of fluorosed enamel is merely superficial [15]. The reason for this is that the central areas of sound enamel crystals are less acid resistant than the peripheral areas due to the high content of carbonate ions. Consequently, although the World Health Organization continues to support F schemes for caries prevention despite a lack of scientific proof [44], the F schemes are not able to improve the crystal quality but rather contribute adversely to affect tooth development and increases the risk of developing postmenopausal osteoporosis.
The exposure to fluoride ions causes the crystal structure defect by interrupting the crystal nucleation process. Further, the combined effect of Es-deficiency and F intake affected adversely the crystal nucleation process, resulting in an increase of amorphous minerals in the bone. Eventually, fluoride exposure increases the bone fragility in postmenopausal women, instead of improving the bone quality.
This study was supported in part by Grant for Supporting Project for Strategic Research from the Japanese Ministry of Education, Culture, Sports, Science and Technology [S0801032, 15K11034].