Gynecology & Obstetrics
Open Access
ISSN: 2161-0932
ISSN: 2161-0932
Research Article - (2017) Volume 7, Issue 10
Objective: To determine whether fetal growth restriction (FGR) fetuses have less facial expressions than appropriate-for-gestational age (AGA) counterparts with the assessment by four-dimensional high-definition live (4D HDlive) ultrasound.
Methods: 4D HDlive ultrasound examinations of fetal facial expressions were performed on singleton pregnant women between 26 and 39 weeks of gestation. The duration of the 4D HDlive recordings was 15 minutes in all cases. The frequency of seven types of previously-reported facial expressions, or blinking, mouthing, yawning, tongue expulsion, sucking, smiling and scowling, were assessed. Two observers counted the frequencies, and inter-and intra-observer reproducibility was examined. Wilcoxon rank-sum test was used for comparison of FGR and AGA group. Kruskal-Wallis test was used for intra-group significance of frequencies of seven types of fetal facial expressions. P<0.05 was considered significant.
Results: In this study, good intra- and inter-class correlation coefficients and intra- and inter-observer agreements were obtained. Thus, measurement values by only one examiner were used for further analysis. The facial expressions of 16 fetuses (FGR: n=8, AGA: n=8) were assessed. We noted a tendency for FGR fetuses to have less facial expressions than AGA counterparts. Although statistically significant inter-group difference was not detected in frequency of any facial expressions, this propensity is conspicuous in smiling (p=0.065) and mouthing (p=0.279). In AGA fetuses, the commonest facial expression was mouthing and was significantly more frequent than blinking (p=0.007), tongue expulsion (p=0.007) and sucking (p=0.002). We also noted a tendency that the frequency of facial expressions declines with fetal maturation. Although no statistically significant difference was shown, this propensity is prominent in mouthing of FGR (p=0.071).
Conclusion: 4D HDlive ultrasound provides promising modalities in novel evaluative imaging of fetal various facial expressions, and may help to elucidate functional development of central nervous system (CNS) and facial expressions both in normal and compromised fetuses.
Keywords: Fetal growth restriction (FGR); Appropriate-for- Gestational Age (AGA) fetus; Fetal facial expressions; Fourdimensional high-definition live (4D HDlive) ultrasound; Inter-class correlation coefficient; Reproducibility; Central nervous system (CNS)
Fetal facial expressions and behavioral patterns can be regarded as indicative of the fetal brain and central nervous system (CNS) development [1]. The cerebral cortex that develops from the most anterior part of the neural plate, a specialized part of the embryonic ectoderm, controls facial expressions [2].
Facial movements are controlled by the cranial nerves V and VII, which appear at around 10 and 11 weeks [3]. Innervation of wellformed facial muscles begins at 8 weeks of gestation, then by 16 weeks all the muscles used in facial expressions are formed, and finally between the gestational ages of 24 and 36 weeks, facial adipose tissue is deposited and gradually builds up [4].
The high-definition live (HDlive) system is a new surface volume rendering mode. The operator adjusts virtual light sources which give the operator the opportunity to create lighting and shadowing effects and enable obvious depth perception of the ultrasound image [5]. By those effects combined with the use of new skin-like colors, HDlive shows us a natural and anatomically realistic appearance of fetuses (Figure 1).
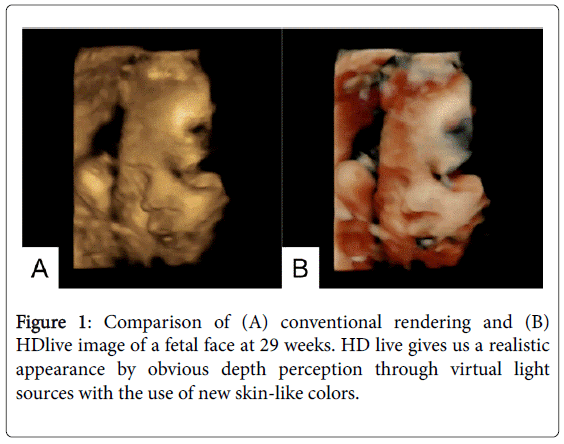
Figure 1: Comparison of (A) conventional rendering and (B) HDlive image of a fetal face at 29 weeks. HD live gives us a realistic appearance by obvious depth perception through virtual light sources with the use of new skin-like colors.
Thus HDlive greatly improves both three-dimensional (3D) and four-dimensional (4D) ultrasound images, and especially 4D HDlive might be able to present us detailed information of vicariously natural fetal facial expressions such as yawning, sucking, smiling, scowling and blinking [6].
Most of observational studies of fetal movement and fetal facial expressions have been done by investigating normal groups and some kind of high-risk groups [7]. Surprisingly, nevertheless, neurobehavioral researches on fetal growth restriction (FGR), which is considered to indicate a possible serious condition in obstetric practice, have rarely been reported.
There have been a few reports on observation of fetal facial expressions using 4D HDlive sonography [8,9]. However, previous studies on gestational age-related tendencies in the frequency of fetal facial expressions were performed solely by conventional 4D sonography and have never been done by 4D HDlive sonography.
The aim of the present study is therefore to investigate differences in facial expressions between FGR and normal fetus counterparts with the use of 4D HDlive ultrasound.
4D HDlive data were collected from singleton pregnant women between 26 and 39 weeks of gestation at our hospital between July 28, 2015 and November 30, 2016.
Subjects
The study groups were comprised of both FGR fetuses and appropriate-for-gestational age (AGA) fetuses. Each fetus underwent at least one examination, and repeated examinations were done at later days in case of unsatisfactory recordings due to malpresentation of the fetus. AGA fetus was defined as a fetus whose size is within the normal range for his or her gestational age.
FGR fetus was defined as estimated fetal body weight (EFBW) of -1.5 SD and below based on the method of The Japan Society of Ultrasonics in Medicine (JSUM), which describes measurement method (biparietal diameter; out-in, abdominal circumference; ellipse approximation, femur length; ossificated both ends), forecasting formula and reference value of EFBW [10]. This definition of FGR is adopted by Guideline for Obstetrical Practice in Japan. World Health Organization defines light for gestational age (LGA) as infants weighing less than the tenth centile for their gestation.
Especially LGA infants less than fifth centile may have poor perinatal prognosis, and mortality and morbidity are increased among infants born at term whose birth weights are at or below the third centile for their gestational age [11]. Fifth centile is equivalent to 1.64 SD in normally distributed population. Based on these, Japanese guideline uses -1.5 SD of fetal body weight reference value as diagnostic criterion and we used this definition in the present study.
Gestational age was calculated based on the first day of the last menstrual period (LMP) and confirmed by first-trimester or early second trimester sonographic measurement. In AGA group, there were four cases dated by LMP, three cases by crown-rump length (CRL), and one case by in vitro fertilization with embryo transfer (IVF-ET) (cryo- ET). All the FGR fetuses were dated by LMP.
The exclusion criteria were multiple pregnancy, fetal anomalies and oligohydramnios. This study was approved by the institutional review board of our institution. Written informed consent was obtained from all pregnant women included in the study.
4D HDlive ultrasound
4D HDlive ultrasound examinations of fetal facial expressions were performed using Voluson E10 (GE healthcare, Zipf, Austria) with RM6c transabdominal convex array transducer (4-8.5 MHz). 4D HDlive setting was standardized using a customized 4D with HDlive preset, as follows: Quality; high 1-2, Mix; 34/66, VSRI; 3-4, Light; BRT 50-60, Shadow; 100.
One ultrasonic observer performed all examinations. After twodimensional (2D) ultrasound examination, the machine was switched to 4D mode. The transducer was arranged so that sagittal sections of the fetal face including the forehead, nose, and mouth were obtained. The images were taken in the region of interest (ROI). Resultant 4D images were shown on a monitor. The duration of the 4D HDlive recordings was 15 minutes in all cases. All imaging data were stored in the hard disk of the ultrasound machine.
Study design
By viewing 15-min 4D HDlive recordings after ultrasound examinations, one examiner (Examiner A) counted the frequency of the following seven types of previously-reported facial expressions by Yan et al in each case: blinking, mouthing, yawning, tongue expulsion, sucking, smiling and scowling [12-14].
Intra-observer reproducibility was also assessed by calculating intraclass correlation coefficient of each facial expression. Another examiner (Examiner B) independently counted the frequency of each facial expression in one third of recordings which were randomly selected from all the cases, and inter-observer agreement was evaluated.
Statistical analysis
Statistical analysis was performed using SPSS 24 (IBM, Japan). To examine the significance of frequencies of each facial expression, t-test and non-parametric Wilcoxon rank-sum test were used for comparison of FGR group and AGA group and for evaluation of gestational-age related tendencies in each group. Kruskal-Wallis oneway analysis of variance by ranks test was used for intra-group significance of frequencies of seven types of fetal facial expressions. P<0.05 was determined statistically significant.
Sixteen fetuses (FGR: n=8, AGA: n=8) were examined (Tables 1A and 1B). All the AGA fetuses were confirmed as normally grown at birth and all the FGR fetuses were LGA infants at birth. The abnormal umbilical cord or placenta in the 2 fetuses of FGR group were verified at birth.
| Case | GA (weeks) | EFBW (g) and SD | Complications |
|---|---|---|---|
| 1 | 26 | 1018 (+0.1) | TPL |
| 2 | 29 | 1361 (-0.4) | TPL |
| 3 | 30 | 1476 (-0.7) | TPL, RA |
| 4 | 33 | 1879 (-0.9) | TPL |
| 5 | 35 | 2314 (-0.1) | TPL |
| 6 | 35 | 2453 (+0.3) | TPL |
| 7 | 36 | 2295 (-0.7) | TPL |
| 8 | 37 | 2485 (-0.6) | NONE |
AGA: Appropriate for gestational age; GA: Gestational age at examination; EFBW: Estimated fetal body weight; SD: Standard deviation; TPL: Threatened premature labor; RA: Rheumatoid arthritis.
Table 1A: Demographics of AGA group.
| Case | GA (weeks) | EFBW (g) and SD | AFI (cm) | MCA-PI | UA-PI | Complications |
|---|---|---|---|---|---|---|
| 9 | 28 | 586 (-3.9) | 11.04 | NM | 1.88 | PIH, TPL, lobed placenta |
| 10 | 32 | 1205 (- 3.0) | 11.86 | 1.57 | 0.88 | TPL |
| 11 | 33 | 1526 (-2.2) | 9.96 | 3.03 | 1.33 | PIH, TPL |
| 12 | 33 | 1391 (-2.9) | 10.75 | 1.38 | 0.78 | TPL |
| 13 | 33 | 1745 (-1.5) | 12.87 | NM | 1.06 | TPL |
| 14 | 36 | 1903 (-2.3) | 10.72 | 1.09 | 0.86 | Marginal cord insertion |
| 15 | 38 | 2271 (-1.9) | 10.03 | NM | 0.68 | NONE |
| 16 | 39 | 2501 (-1.5) | 9.53 | 1.79 | 0.73 | Maternal hypothyroidism |
FGR: Fetal growth restriction; GA: Gestational age at examination; EFBW: Estimated fetal body weight; SD: Standard deviation; AFI: Amniotic fluid index; MCA-PI: Middle cerebral artery pulsatility index; UA-PI: Umbilical artery pulsatility index; NM: Not measured; PIH: Pregnancy-induced hypertension; TPL: Threatened premature labor.
Table 1B: Demographics of FGR group.
Table 2 shows maternal and fetal backgrounds of the study population. There were no significant differences between AGA and FGR groups.
| AGA (n=8) | FGR (n=8) | p | |
|---|---|---|---|
| Maternal age (years) ± SD | 30.75 ± 7.51 | 30. 37 ± 5.70 | 0.383 |
| GA (weeks) ± SD | 32.91 ± 3.63 | 34.37 ± 3.53 | 0.096 |
| EFBW (g) ± SD | 1910.12 ± 563.57 | 1641.00 ± 608.84 | 0.935 |
AGA: Appropriate-for-gestational age; FGR: Fetal growth restriction; SD: Standard deviation; GA: Gestational age at examination; EFBW: Estimated fetal body weight.
Table 2: Maternal and fetal backgrounds of the study population.
Figure 2 depicts 4D HDlive ultrasound images of seven types of fetal facial expression in both groups.
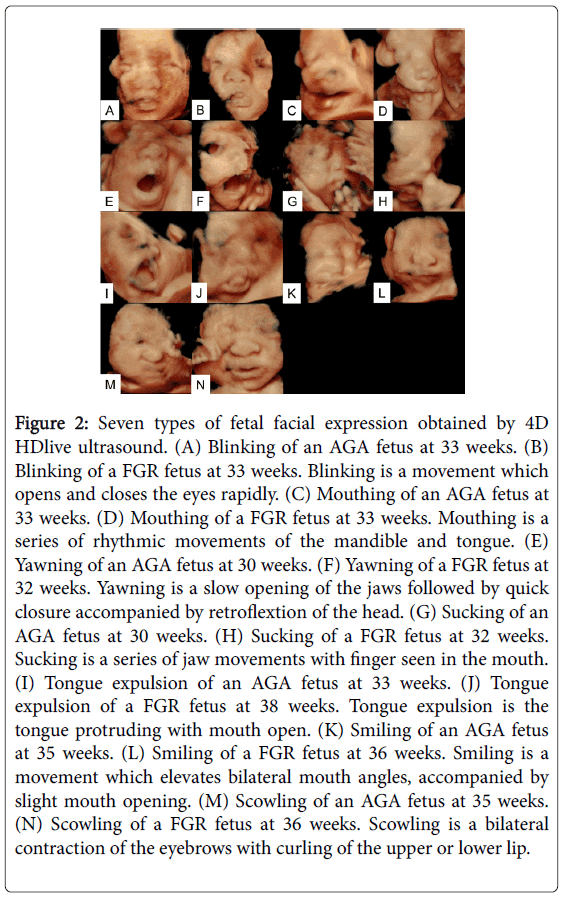
Figure 2: Seven types of fetal facial expression obtained by 4D HDlive ultrasound. (A) Blinking of an AGA fetus at 33 weeks. (B) Blinking of a FGR fetus at 33 weeks. Blinking is a movement which opens and closes the eyes rapidly. (C) Mouthing of an AGA fetus at 33 weeks. (D) Mouthing of a FGR fetus at 33 weeks. Mouthing is a series of rhythmic movements of the mandible and tongue. (E) Yawning of an AGA fetus at 30 weeks. (F) Yawning of a FGR fetus at 32 weeks. Yawning is a slow opening of the jaws followed by quick closure accompanied by retroflextion of the head. (G) Sucking of an AGA fetus at 30 weeks. (H) Sucking of a FGR fetus at 32 weeks. Sucking is a series of jaw movements with finger seen in the mouth. (I) Tongue expulsion of an AGA fetus at 33 weeks. (J) Tongue expulsion of a FGR fetus at 38 weeks. Tongue expulsion is the tongue protruding with mouth open. (K) Smiling of an AGA fetus at 35 weeks. (L) Smiling of a FGR fetus at 36 weeks. Smiling is a movement which elevates bilateral mouth angles, accompanied by slight mouth opening. (M) Scowling of an AGA fetus at 35 weeks. (N) Scowling of a FGR fetus at 36 weeks. Scowling is a bilateral contraction of the eyebrows with curling of the upper or lower lip.
In this study, good intra- and inter-class correlation coefficients not less than 0.7 were obtained except inter-class correlation coefficient of scowling, which is 0.681, and intra- and inter-observer agreements were confirmed.
Thus, measurement values by only one examiner (Examiner A) were used for further analysis.
Tables 3A and 3B; Figures 3A and 3B demonstrate the frequency of seven types of fetal facial expressions observed in each fetus. We noted a tendency for FGR group to have less facial expressions than AGA group.
| Case | GA (weeks) | Blinking | Mouthing | Yawning | T.E. | Sucking | Smiling | Scowling |
|---|---|---|---|---|---|---|---|---|
| 1 | 26 | 0 | 6 | 2 | 0 | 0 | 0 | 2 |
| 2 | 29 | 0 | 2 | 0 | 0 | 0 | 1 | 1 |
| 3 | 30 | 0 | 4 | 2 | 0 | 1 | 0 | 1 |
| 4 | 33 | 1 | 1 | 1 | 0 | 0 | 3 | 0 |
| 5 | 35 | 0 | 2 | 0 | 0 | 0 | 2 | 0 |
| 6 | 35 | 1 | 5 | 4 | 1 | 0 | 3 | 2 |
| 7 | 36 | 0 | 4 | 0 | 1 | 0 | 3 | 0 |
| 8 | 37 | 0 | 1 | 0 | 0 | 0 | 0 | 0 |
AGA: Appropriate-for-gestational age; GA: Gestational age at examination; T.E.: Tongue expulsion.
Table 3A: Frequencies of blinking, mouthing, yawning, tongue expulsion, sucking, smiling, and scowling in each AGA case during 15-minute recording.
| Case | GA (weeks) | Blinking | Mouthing | Yawning | T.E. | Sucking | Smiling | Scowling |
|---|---|---|---|---|---|---|---|---|
| 9 | 28 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 10 | 32 | 0 | 4 | 3 | 0 | 5 | 0 | 0 |
| 11 | 33 | 0 | 4 | 1 | 0 | 0 | 0 | 0 |
| 12 | 33 | 0 | 2 | 3 | 0 | 0 | 0 | 1 |
| 13 | 33 | 10 | 7 | 11 | 1 | 0 | 0 | 0 |
| 14 | 36 | 0 | 0 | 2 | 1 | 0 | 1 | 2 |
| 15 | 38 | 0 | 0 | 0 | 0 | 3 | 0 | 2 |
| 16 | 39 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
FGR: Fetal growth restriction; GA: Gestational age at examination; T.E.: Tongue expulsion.
Table 3B: Frequencies of blinking, mouthing, yawning, tongue expulsion, sucking, smiling, and scowling in each FGR case during 15-minute recording.
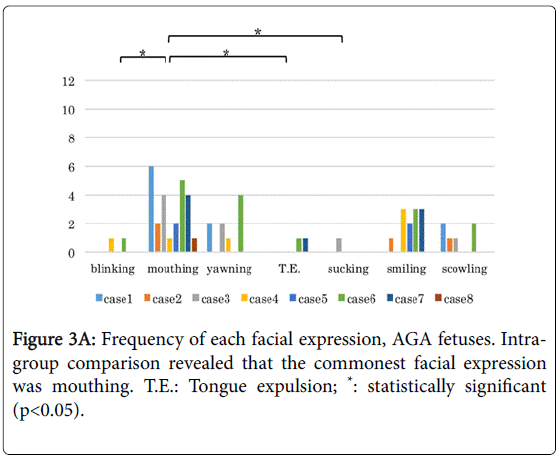
Figure 3A: Frequency of each facial expression, AGA fetuses. Intragroup comparison revealed that the commonest facial expression was mouthing. T.E.: Tongue expulsion; *: statistically significant (p<0.05).
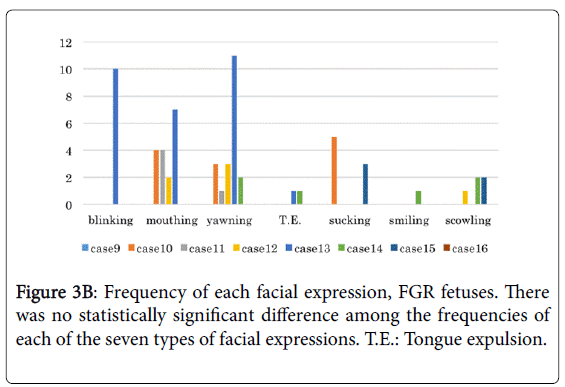
Figure 3B: Frequency of each facial expression, FGR fetuses. There was no statistically significant difference among the frequencies of each of the seven types of facial expressions. T.E.: Tongue expulsion.
Although statistically significant difference was not seen in frequency of any facial expressions, this propensity is especially demonstrated in smiling (p=0.065) and mouthing (p=0.279), as shown in Table 4. The effect size for smiling is 0.55.
| Blinking | Mouthing | Yawning | T.E. | Sucking | Smiling | Scowling | ||
|---|---|---|---|---|---|---|---|---|
| AGA | ||||||||
| median | 0 | 3 | 0.5 | 0 | 0 | 1.5 | 0.5 | |
| range | 0-1 | 1-6 | 0-4 | 0-1 | 0-1 | 0-3 | 0-2 | |
| FGR | ||||||||
| median | 0 | 1 | 1.5 | 0 | 0 | 0 | 0 | |
| range | 0-10 | 0-7 | 0-11 | 0-1 | 0-5 | 0-1 | 0-2 | |
| p | 0.798 | 0.279 | 0.505 | 1.000 | 0.645 | 0.065 | 0.798 | |
T.E.: Tongue expulsion; AGA: Appropriate-for-gestational age; FGR: Fetal growth restriction.
Table 4: Intergroup comparison of frequency of each facial expression.
In AGA group (Figure 3A), the commonest facial expression was mouthing and was significantly more frequent than blinking (p=0.007), tongue expulsion (p=0.007) and sucking (p=0.002).
In FGR group (Figure 3B), on the other hand, there was no statistically significant difference among the frequencies of each of the seven types of facial expressions.
This study shows that there seems to be a tendency that the frequency of fetal facial expressions declines with fetal maturation.
Tables 5A and 5B; Figures 4A and 4B indicate that the comparison of the cases earlier and later than 34 weeks by Wilcoxon rank-sum test in each group revealed the propensity especially in FGR group.
| Case | GA (weeks) | Blinking | Mouthing | Yawning | T.E. | Sucking | Smiling | Scowling | |
|---|---|---|---|---|---|---|---|---|---|
| <34 weeks | |||||||||
| 1 | 26 | 0 | 6 | 2 | 0 | 0 | 0 | 2 | |
| 2 | 29 | 0 | 2 | 0 | 0 | 0 | 1 | 1 | |
| 3 | 30 | 0 | 4 | 2 | 0 | 1 | 0 | 1 | |
| 4 | 33 | 1 | 1 | 1 | 0 | 0 | 3 | 0 | |
| ≥ 34 weeks | |||||||||
| 5 | 35 | 0 | 2 | 0 | 0 | 0 | 2 | 0 | |
| 6 | 35 | 1 | 5 | 4 | 1 | 0 | 3 | 2 | |
| 7 | 36 | 0 | 4 | 0 | 1 | 0 | 3 | 0 | |
| 8 | 37 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | |
| p | 1.000 | 0.886 | 0.486 | 0.343 | 0.686 | 0.486 | 0.486 | ||
AGA: Appropriate-for-gestational age; GA: Gestational age at examination; T.E.: Tongue expulsion.
Table 5A: Comparison of the cases earlier and later than 34 weeks in AGA group.
| Case | GA (weeks) | Blinking | Mouthing | Yawning | T.E. | Sucking | Smiling | Scowling | |
|---|---|---|---|---|---|---|---|---|---|
| < 34 weeks | |||||||||
| 9 | 28 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| 10 | 32 | 0 | 4 | 3 | 0 | 5 | 0 | 0 | |
| 11 | 33 | 0 | 4 | 1 | 0 | 0 | 0 | 0 | |
| 12 | 33 | 0 | 2 | 3 | 0 | 0 | 0 | 1 | |
| 13 | 33 | 10 | 7 | 11 | 1 | 0 | 0 | 0 | |
| ≥ 34 weeks | |||||||||
| 14 | 36 | 0 | 0 | 2 | 1 | 0 | 1 | 2 | |
| 15 | 38 | 0 | 0 | 0 | 0 | 3 | 0 | 2 | |
| 16 | 39 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| p | 0.786 | 0.071 | 0.250 | 0.786 | 1.000 | 0.571 | 0.250 | ||
FGR: Fetal growth restriction; GA: Gestational age at examination; T.E.: Tongue expulsion.
Table 5B: Comparison of the cases earlier and later than 34 weeks in FGR group.
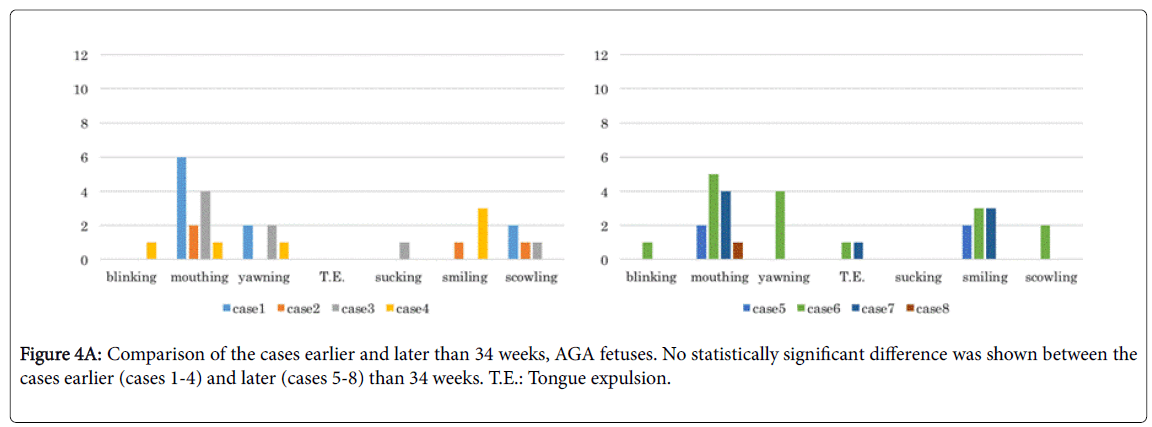
Figure 4A: Comparison of the cases earlier and later than 34 weeks, AGA fetuses. No statistically significant difference was shown between the cases earlier (cases 1-4) and later (cases 5-8) than 34 weeks. T.E.: Tongue expulsion.
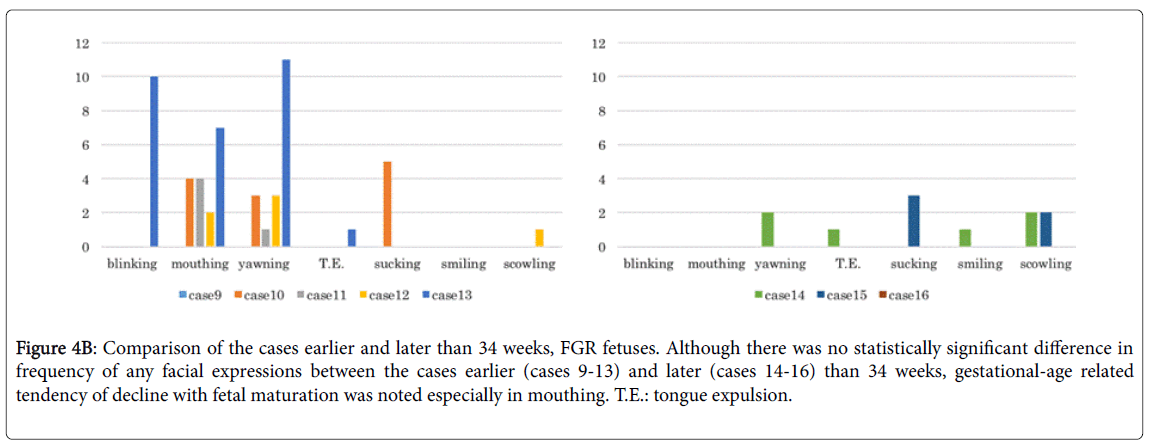
Figure 4B: Comparison of the cases earlier and later than 34 weeks, FGR fetuses. Although there was no statistically significant difference in frequency of any facial expressions between the cases earlier (cases 9-13) and later (cases 14-16) than 34 weeks, gestational-age related tendency of decline with fetal maturation was noted especially in mouthing. T.E.: tongue expulsion.
Although no statistically significant difference was shown, this propensity is prominent in mouthing of FGR (p=0.071).
Tables 6A and 6B; Figures 5A and 5B demonstrate the comparison of the cases earlier than 34 weeks between AGA group and FGR group (Table 6A and Figure 5A) and those later than 34 weeks between AGA group and FGR group (Table 6B and Figure 5B) by Wilcoxon rank-sum test.
| Case | GA (weeks) | Blinking | Mouthing | Yawning | T.E. | Sucking | Smiling | Scowling |
|---|---|---|---|---|---|---|---|---|
| AGA group | ||||||||
| 1 | 26 | 0 | 6 | 2 | 0 | 0 | 0 | 2 |
| 2 | 29 | 0 | 2 | 0 | 0 | 0 | 1 | 1 |
| 3 | 30 | 0 | 4 | 2 | 0 | 1 | 0 | 1 |
| 4 | 33 | 1 | 1 | 1 | 0 | 0 | 3 | 0 |
| FGR group | ||||||||
| 9 | 28 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 10 | 32 | 0 | 4 | 3 | 0 | 5 | 0 | 0 |
| 11 | 33 | 0 | 4 | 1 | 0 | 0 | 0 | 0 |
| 12 | 33 | 0 | 2 | 3 | 0 | 0 | 0 | 1 |
| 13 | 33 | 10 | 7 | 11 | 1 | 0 | 0 | 0 |
| p | 1.000 | 1.000 | 0.413 | 0.730 | 1.000 | 0.286 | 0.190 | |
AGA: Appropriate-for-gestational age; FGR: Fetal growth restriction; GA: Gestational age at examination; T.E.: Tongue expulsion.
Table 6A: Comparison of the cases earlier than 34 weeks between AGA group and FGR group.
| Case | GA (weeks) | Blinking | Mouthing | Yawning | T.E. | Sucking | Smiling | Scowling |
|---|---|---|---|---|---|---|---|---|
| AGA group | ||||||||
| 5 | 35 | 0 | 2 | 0 | 0 | 0 | 2 | 0 |
| 6 | 35 | 1 | 5 | 4 | 1 | 0 | 3 | 2 |
| 7 | 36 | 0 | 4 | 0 | 1 | 0 | 3 | 0 |
| 8 | 37 | 0 | 1 | 0 | 0 | 0 | 0 | 0 |
| FGR group | ||||||||
| 14 | 36 | 0 | 0 | 2 | 1 | 0 | 1 | 2 |
| 15 | 38 | 0 | 0 | 0 | 0 | 3 | 0 | 2 |
| 16 | 39 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| p | 0.629 | 0.057 | 1.000 | 0.857 | 0.629 | 0.229 | 0.400 | |
AGA: Appropriate-for-gestational age; FGR: Fetal growth restriction; GA: Gestational age at examination; T.E.: Tongue expulsion.
Table 6B: Comparison of the cases later than 34 weeks between AGA group and FGR group.
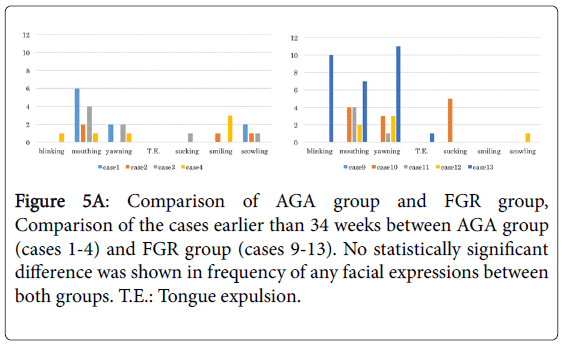
Figure 5A: Comparison of AGA group and FGR group, Comparison of the cases earlier than 34 weeks between AGA group (cases 1-4) and FGR group (cases 9-13). No statistically significant difference was shown in frequency of any facial expressions between both groups. T.E.: Tongue expulsion.
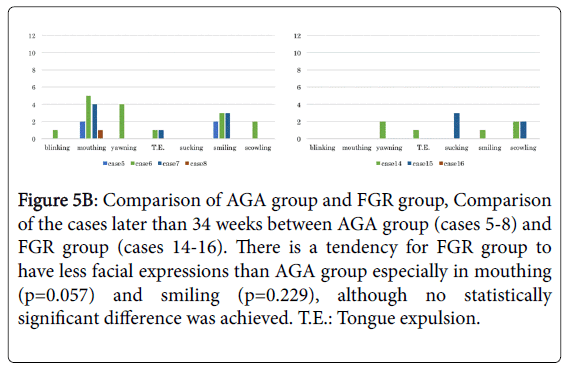
Figure 5B: Comparison of AGA group and FGR group, Comparison of the cases later than 34 weeks between AGA group (cases 5-8) and FGR group (cases 14-16). There is a tendency for FGR group to have less facial expressions than AGA group especially in mouthing (p=0.057) and smiling (p=0.229), although no statistically significant difference was achieved. T.E.: Tongue expulsion.
In cases later than 34 weeks, there is a tendency for FGR group to have less facial expressions than AGA group.
Although no statistically significant difference was achieved, this propensity is noted in mouthing (p=0.057) and smiling (p=0.229).
This study revealed differences in fetal facial expressions between AGA and FGR group using 4D HDlive ultrasound. As far as we know, there have been no reports examining facial expressions of FGR fetuses by 4D HDlive ultrasound. We herein showed two important clinical observations. First, we noted a tendency for FGR fetuses to have less facial expressions than AGA counterparts. Second, in addition to the gestational age-related tendencies of fetal facial expressions in normal fetuses examined previously by conventional 4D ultrasound, we revealed more prominent such propensity in FGR fetuses with the use of 4D HDlive ultrasound.
The first finding is important for evaluating neurological development in FGR fetuses both in the embryological aspect and in obstetric practice. As the fetus develops, fetal movements of the face, limbs and torso are correlated with the structural development of CNS [15], demonstrating that the connection between cerebral cortex and peripheral structures of the fetus are functional. In addition to simple muscle movements, cerebral cortex functions are developed to facilitate learning in the fetus prenatally [15]. Also in compromised fetuses, development progresses with gestation, although progress is at variance with that in healthy fetuses, indicating that fetal facial movements may serve as a marker for normal development [16,17]. Many observational researches regarding fetal movement and fetal facial expressions have been carried out by assessing normal group and some kind of high-risk groups of pregnancy. Although the emergence of fetal movement patterns is said to be distorted in FGR fetuses [7], neurobehavioral studies focused on FGR, which is considered to be one of high-risk groups, have scarcely ever been implemented.
There have been no more than three literatures concerning fetal neurobehavioral assessment mainly on FGR. Andonotopo et al. [18] conducted a prospective study of 50 pregnancies with FGR fetuses in the third trimester of pregnancy to find out whether the quantity of fetal facial expression and quality of body movement could be used as an additional diagnostic criterion for prenatal brain impairment in fetuses with growth restriction. A tendency of less behavioral activity such as growth restricted fetuses’ blinking less than normal counterparts was revealed, and the results of the preliminary research encouraged the further investigation with 4D ultrasound, which lead to introduce KANET for the assessment of neurological status of the fetus [19]. KANET is a combination of parameters such as isolated head anteflextion, overlapping cranial sutures, head circumference, isolated eye blinking, facial alterations, mouth opening, isolated hand and leg movements, finger movements, gestalt perception of general movements. Vladareanu et al. [20] used KANET to assess 196 singleton pregnancies between 24 and 38 weeks of gestation. In their study, fetuses getting borderline KANET score were those who were FGR with increased resistance index (RI) of middle cerebral artery (MCA). Predojevic et al. [21] used KANET to assess 5 growth restricted fetuses between 31 and 39 weeks of gestation, and concluded that KANET could recognize pathologic and borderline behavior in FGR fetuses with or without blood flow redistribution. These previous studies are based on observation by conventional 4D ultrasound. The present study focused on fetal facial expressions which are important parts of KANET, and applied novel 4D HDlive ultrasound that can show us more natural and realistic appearance of fetuses than conventional 4D ultrasound (Figures 1 and 2). Our results showed a propensity of less facial expression in FGR compared to normal counterparts, especially in smiling.
The second finding is interesting, because our current study showed that gestational age-related tendencies of fetal facial expressions in FGR group, especially mouthing, were more prominent than in AGA group (Tables 5B and 6B, Figures 4B and 5B). Previous studies of normal fetuses using conventional 4D ultrasound revealed some extent of such tendencies in the frequency of fetal facial expressions. Yigiter et al. [22] revealed that mouthing was the most frequent facial pattern between 18 and 27 weeks of gestation, while scowling was the most prominent between 28 and 36 weeks of gestation. Sato et al. [14] described that mouthing was the most common facial expression between 20 and 24 weeks of gestation. Kanenishi et al. [13] showed that mouthing was the most common facial expression between 25 and 27 weeks of gestation. Yan et al. [12] noted that mouthing was the most frequent facial expression between 28 and 34 weeks of gestation whereas the least frequent were scowling and sucking. These papers contradict each other about the frequency of facial patterns, which may have resulted from small sample size in each study, different study samples in all trimesters of pregnancy, and racial differences between Turkish (Yigiter et al. [22]) and Japanese (Sato et al. [14], Kanenishi et al. [13], and Yan et al. [12]). In the present study using 4D HDlive ultrasound, AGA fetuses between 26 and 37 weeks of gestation demonstrated that mouthing was the most frequent facial expression (Figure 3A), which is compatible with the previous reports from Japan (Sato et al. [14], Kanenishi et al. [13], and Yan et al. [12]). In contrast to AGA fetus, however, remarkable decrease in the frequency of this mouthing later than 34 weeks in FGR fetuses is the most striking finding in our current study (Tables 5B and 6B, Figures 4B and 5B). We therefore assume that in obstetric clinical situations, mouthing could be the most notable facial expression according to gestational age in FGR fetuses compared with in AGA fetuses. Although there have been a few reports on observation of fetal facial expressions using HDlive [8,9], this is the first report examining gestational age-related tendencies in the frequency of fetal facial expressions with the use of 4D HDlive ultrasound, especially in FGR fetuses.
We think that the facial expressions of FGR are related with some factors, such as PIH that leads to increasing vessel resistance with reducing blood flow into the cerebral cortex and the facial muscle, which might result in hypoactivity of the facial nerve and facial muscle compared with AGA. A tendency toward decreased frequency of facial expressions and movement patterns with increasing gestational age from the second to third trimesters has also been reported [9, 22-25]. Fetal smiles and spontaneous smiles in neonates are thought to work as a preparation of various facial expressions including social smiles, and the smiles might have the function of facilitating the development of facial muscles especially the zygomatic major muscles [26]. Suspected inhibition of neurological development in FGR compared with AGA may lead to oversuppression of facial expressions, especially in smiling, and this expectant inhibition may concern with remarkable decrease in mouthing later than 34 weeks of gestation as shown in our study.
This study has three limitations. First, small size of the study population prevents us from generalizing the obtained results. Recruiting large sample sizes is required in the future study to investigate whether the tendency demonstrated in the present study can be generalized with statistically significant difference. Second, subjective determination to evaluate fetal facial expressions obtained by 4D HDlive ultrasound might lead to inter-observer variability [13,25]. Although relatively good intra- and inter-class correlation coefficients were obtained in the present study, further investigations are required [14,27]. Third, fetal consciousness state at the ultrasound examination were not determined. Although most of the previous observational studies of fetal facial expressions using conventional 4D ultrasound had the same problem, it should be considered whether fetuses are awake or not because frequency of each of fetal facial expressions may change by fetal awakeness.
In conclusion, this preliminary study showed the tendency for FGR fetuses to have less facial expressions than AGA counterparts and, in addition to the gestational age-related tendencies of fetal facial expressions in normal fetuses examined previously by conventional 4D ultrasound, this study also revealed more prominent such propensity in FGR fetuses with the use of 4D HDlive ultrasound, especially in mouthing. The present study with novel evaluative images presented that 4D HDlive ultrasound might be a method to visualize facial expressions of fetuses related with the development of the fetal CNS in real time (Figure 2). Identifying functional characteristics of the fetus could lead to predict normal and abnormal neurological development and such information will be of great value in counseling mothers of high-risk pregnancies [7]. However, this technology does not provide specific information on which nervous centers are developed or undergoing development, and correlations of the described facial expressions and the fetal condition or even neonatal neurodevelopment are not yet clear [14]. Further researches using HDlive and 4D ultrasound are required to obtain the evidence of fetal neurobehavioral development and to evaluate normal and abnormal fetal facial expressions [9]. We believe that 4D HDlive ultrasound provides promising modalities in novel evaluative imaging of fetal various facial expressions, and may help to elucidate functional mechanism of development of CNS and facial expressions both in normal and compromised fetuses. Based on our current study, remarkable decrease in the frequency of mouthing according to gestational age seems to be the most notable finding in facial expressions of FGR fetuses compared with AGA fetuses.
We thank all the clinical staffs of Maternal Fetal Intensive Care Unit of Iwate Medical University Hospital for their help in performing examinations and the mothers who kindly agreed to take part in this study. We are grateful to Naomi Kumeda for her assistance on facial image processing.