Medical & Surgical Urology
Open Access
ISSN: 2168-9857
ISSN: 2168-9857
Review Article - (2018) Volume 7, Issue 4
Introduction: Management of lower caliceal stones is challenging. Recent advances in technology have led to the implementation of micro percutaneous nephrolithotomy (microperc) as well as retrograde intrarenal surgery (RIRS) in the management of lower caliceal kidney stones.
Objective: Review of studies evaluating the role of RIRS and microperc techniques for the treatment of lower caliceal kidney stones.
Evidence acquisition: A systematic literature review was performed in September 2017 using the PubMed, Scopus, and Web of Science databases to identify relevant studies.
Conclusion: Microperc and RIRS, both are valid options for the treatment of small lower caliceal stones in adult patients. The stone clearance rates in both microperc and RIRS are comparably high and the complication rates are comparably low. Microperc is associated with more post-operative pain and more fall in the haemoglobin level while RIRS is associated with more intraoperative DJ insertion.
Keywords: Kidney stones; Microperc; Retrograde intrarenal surgery; Lower caliceal
Kidney stones are becoming increasingly prevalent, the cause of which is still unclear [1,2]. Multiple factors can contribute to the treatment choice and success. Therefore, the European Association of Urology (EAU) guidelines recommend different treatment options for renal stones with different sizes and different locations.
According to the EAU guidelines, endourological management (percutaneous nephrolithotomy [PNL] and retrograde intrarenal surgery [RIRS]) is the recommended treatment for stones larger than 2 cm in diameter while shockwave lithotripsy (SWL) is the first option for smaller kidney stones [3]. The choice of the treatment is also affected by other factors including stone location and pelvicalyceal anatomy [4,5].
Natural history of caliceal stones
Natural history of small, non-obstructing asymptomatic lower pole stones is not well defined, and the risk of size progression is unpredictable. There is no agreed protocol on the intervention timing, method, or follow up. The EAU guidelines recommended to actively treat caliceal stones associated with stone growth, collecting system obstruction, infection, and acute and/or chronic pain [3].
Several studies have investigated the risk of stone progression, development of symptoms, or the need for intervention in lower pole stones. Glowacki et al. estimated the risk of development of symptoms or the need for intervention to be around 10% per year; with a cumulative 5-year event probability of 48.5% [6]. Another study reported that 77% of patients with silent caliceal stones experienced progression in stone size, with 26% requiring surgical intervention [7].
Treatment of non-symptomatic caliceal stones is still a debate. Although some have recommended prophylactic treatment for these stones to prevent stone progression and complications, conflicting data have been reported [8-10]. Other authors recommend active treatment based on the data from studying the natural history of small residual stone fragments after SWL or URS [11]. On the other side, excellent stone free rates and pain reliefs have been reported after removal of small symptomatic caliceal stones by SWL, PNL or URS [10-12].
Treatment of lower caliceal stones
The management of symptomatic lower caliceal calculi is still being considered as a problematic issue. All treatment modalities, such as SWL, RIRS, and PNL ranging from noninvasive to invasive, can be used according to the stone size and anatomic factors [4,5].
Extracorpral shock wave lithroripsy (SWL)
Because of its noninvasive nature, SWL was accepted as a first-line treatment modality for patients with lower caliceal renal calculi up to 1 cm in diameter. Studies have shown, however, that success rates of SWL are influenced by patient- and stone related factors including stone size, location, and composition, pelvicaliceal system anatomy, and skin-to-stone distance (SSD) [13,14].
The stone clearance rate after SWL seems to be lower for stones in the inferior calyx than for other intrarenal locations. The stone clearance rate after Shockwave lithotripsy for the lower pole stones is very variable and widely ranges from 25% to 85% [15-18], therefore, endoscopic procedures (PNL and RIRS) are recommended for stones >10 mm and a valid option for smaller size stones [3].
Retrograde intra renal surgery (RIRS)
RIRS for lower caliceal stones is an acceptable alternative therapeutic method to standard PNL. With the development of new generation flexible ureteroscopes with greater deflection and control, there has been an increased use of ureteroscopy and laser lithotripsy for renal stones [19]. Significant advancement in the technology of manufacturing flexible ureteroscopies as well as holmium laser fibers has resulted in high treatment success rate and limited morbidity.
The flexibility of the new generations of ureteroscopes allowed access to lower calices. The development of small diameter laser fiber and retrieval baskets helped with scope maneuverability. Also, the standard use of access sheath helped with the insertion of the scope while maintaining low intrarenal pressure [20].
Fabrizio et al. [21] evaluated the role of RIRS in the management of kidney stones in patients whom SWL or PNL was contraindicated or previously failed. The authors reported a stone free rate of 77% after single session of flexible ureteroscopy and a further 12% with a single asymptomatic stone fragment less than 3 mm. Grasso et al. [22] published their own results on evaluation of the role of ureteroscopy in management of lower caliceal stones. They reported a stone free rate of 76%. When stratified by stone size, the stone-free rates were 82% and 71% for patients with stones 1 to 10 mm and 11 to 20 mm, respectively.
The stone free rate for RIRS has been reported to be above 90% in management of kidney stones and as high as 85% for lower caliceal stones. Despite of the high success rate of RIRS, there seems to be some limitations in management of lower caliceal stones. Resorlu et al reported that 7% of the lower caliceal stones were found to be inaccessible among 1000 cases of their ureteroscopy series. On further evaluation, stone length and different anatomical variables of the lower calix can affect stone clearance rate [23].
Certain maneuvers were described to improve the success rate of RIRS in the management of lower pole stones. Schuster et al. [24] published their experience in management of lower caliceal stones using a novel technique. They used a nitinol basket or a grasper to displace the stones from the lower calix into more accessible calix.
Stone clearance rate was better in the displacement group in comparison to the in situ group (79% and 61% respectively). Further subgroup analysis revealed that in treatment a group for calculi 1 cm or less, complete success was obtained in 77% of in situ group versus 89% in the displacement groups. For stones larger than 1 cm complete success was achieved in 29% in the in situ versus all 100% in the displacement group.
When compared to standard PNL, RIRS is a safer approach for management of small kidney stones. Development of the new generations of flexible ureteroscopy with smaller diameter, better deflection and improved optics, has led to reduction in the risk of major procedure related complications. Furthermore, RIRS has been proven safe in patients at high risk, such as pregnant women, obese patients, or those with coagulopathy or in whom PNL may be contraindicated [22].
Minimally invasive percutaneous procedures (miniperc and ultraminiperc)
To reduce the disadvantages of conventional PNL, a ‘mini-perc’ technique was first developed. Jackman et al. [25] defined the ‘miniperc’ as a percutaneous nephrolithotomy achieved through a sheath too small to accommodate a standard rigid nephroscope. While standard nephroscopes have shaft calibers of 24-30Fr, so-called ‘miniperc’ instruments have smaller dimensions ranging 12-20Fr.
Both standard PNL and miniperc are multistep procedures that require initial ultrasound or fluoroscopic access, guide wire placement in the system, removal of the initial puncture needle over the guide wire, serial or single-step dilation of the tract with resultant tract bleeding during the maneuvers and finally the placing of a sheath over the tract dilators.
These individual maneuvers are time consuming and often have disadvantages, such as increased fluoroscopic time and radiation, tract bleeding and inadvertent complications, including caliceal or infundibular tearing and pelvic perforation [26].
Janak et al. invented an innovative PNL technique, which is termed as ultramini- PNL (UMP). The essential element of the novel UMP is using a 6 Fr Mini nephroscope through an 11-13 Fr metal sheath to perform holmium: YAG laser lithotripsy.
Dilation is achieved in one step with much less fluoroscopy time, and the cross-section of the puncture channel is only approximately 30% of that required with the conventional miniperc (reference to 18 Fr size) [27].
This miniaturization is the main reason why no blood transfusion and why no nephrostomy tube routinely placed in their group of patients. In UMP the stones may not to be smashed to dust, it is enough to be disintegrated to a size less than 3 mm then, like the mini- PNL, small fragmented stones (≤ 3 mm) will pass around the endoscope and wash out through the sheath, The authors claimed that UMP would be an alternative to SWL and flexible ureteroscopy as it provides the ability to gain direct access to the desired calyx and accomplish a higher immediately stone-free rate (88.9% in the study) [27].
Micro percutaneous nephrolithotomy (microperc)
Microperc was defined as modified PNL in which renal access and PNL are performed in a single step through the all-seeing needle with a 4.85 Fr tract size. The highly advanced telescope for the procedure consists of micro-optics of less than 1 mm diameter with a resolution of up to 10,000 pixels. The telescope with the light lead is inserted in the outer sheath of the puncture needle. The puncture needle has an outer circumference of 1.6 mm (4.85 Fr).
The telescope is made of fiberoptics which gives it the advantage of being highly flexible. After obtaining the puncture, the sharp inner part of the needle is removed and a three-way connector is attached to the outer sheath of the needle with the telescope inserted through the central port, irrigation from one side port and laser fiber through the third side port. The optics is relayed through a multi-joint mounting arm with attached camera and light cable (Figures 1 and 2).
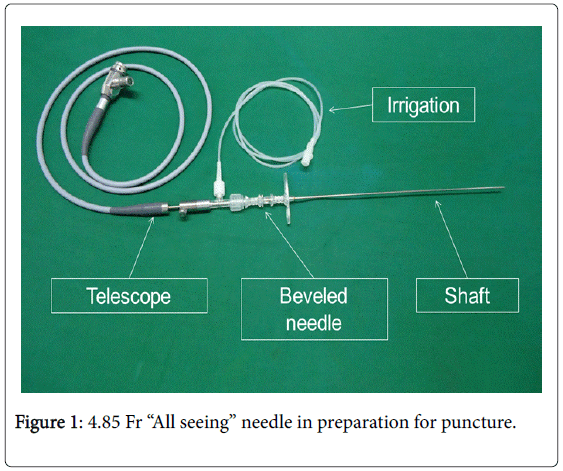
Figure 1: 4.85 Fr “All seeing” needle in preparation for puncture.
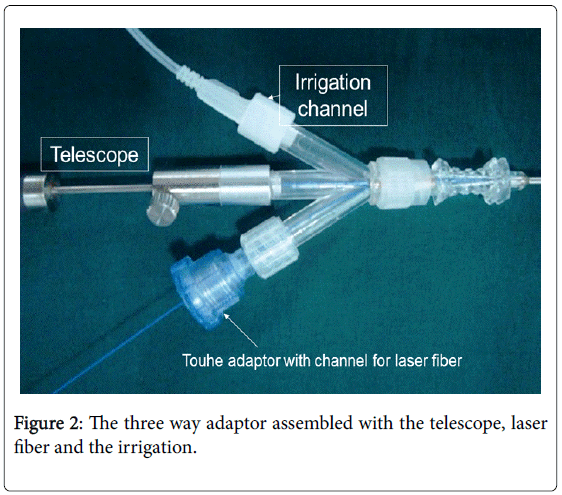
Figure 2: The three way adaptor assembled with the telescope, laser fiber and the irrigation.
Microperc is different from standard PNL and mini PNL. Microperc is done through the smallest possible tract diameter which is limited to the puncture needle diameter. This miniaturization can reduce the risk of bleeding which is a recognized complication of PNL. The downside of having no working sheath is that microperc does not allow retrieval of any stone fragments. Still, the use of laser with the aim of stone dusting can eliminate the need for fragment retrieval [28,29].
The first study on “All seeing needle” needle was done by Desai et al. [28]. The authors evaluated the use of the needle in 10 patients with small kidney stones less than 15 mm. The success rate was reported to be 89%. The growing interest in the use of microperc has led to several evaluation studies, some of them were small case series [30-33]. Larger series was reported by Hatipoglu et al. [34]. The authors evaluated the procedure in four centers.
Microperc versus retrograde intrarenal surgery
Several authors evaluated microperc in a more comprehensive way and evaluated the technique against RIRS [35-37]. Sabnis et al. evaluated the role of microperc and RIRS in management of kidney stones <15 mm in diameter in a randomized prospective trial [35]. The authors found that microperc and RIRS both have similar stone free and complication rates (97% versus 94% SFR respectively). Moreover, microperc group was associated with higher level hemoglobin loss (0.96 versus 0.56 g/dl in RIRS group, p=<0.001), increased pain (4.8 versus 3.8 VAS in RIRS, p=0.003), and greater analgesic requirements, whereas RIRS was associated with a higher rate of DJ stenting (20% versus 62.8% in microperc group).
Tepeler et al. [37] performed a retrospective study comparing microperc and RIRS in lower pole stones less than or equal to 2 cm. They included 68 patients in the microperc and 59 patients in RIRS group. They found that microperc SFR was higher and the operative time was shorter than for RIRS (88.2% and 46.2 min versus 74.5% and 80.1 min respectively). The complication rate was 2.9% in microperc group and 13.5% in RIRS group and all the complications were mild.
As mentioned earlier, there is no facility to retrieve the stone fragments in microperc. The small fragments generated by laser fragmentation are flushed out with the irrigation fluid. This can lead to obstruction of the collecting system especially in the presence of relatively large fragments causing colic episodes and even steinstrasse. In a series by Armagan et al. [36] two patients developed renal colic or steinstrasse, the latter required DJ insertion. Similarly, Silay et al. [32] reported two cases of renal colic, Hatipoglu et al. [34] reported eight cases of renal colic and five cases of steinstrasse and Tepeler et al. reported 6 patients developed renal colic [36].
Intraoperative conversion to miniperc may be necessary in cases where vision is impaired due to bleeding and in cases where stones migrate to a different calix. In a series by Armagan et al. [36] conversion to miniperc was required in 3/30 patients (10%), in a series by Piskin et al. [33] it was required in 2/9 patients and in a series by Hatipoglu et al. [34] it was required in 12/140 patients (8.57%). In a study by Sabnis et al. [35] it was required in 2/70 patients (2.8%, one patient in each group). In Tepeler et al. [37] conversion to miniperc was done in 6 patients in each study group. The reason for conversion was inadequate vision in microperc and inability to reach the stone using the deflection in RIRS.
The post-operative hospital stay is variable between studies based on individual center policy. Sabnis et al. [35] reported a hospital stay of 57 hours in the microperc group versus 49 hours in RIRS group while in Tepeler et al. [36,37] the hospitalization time was 33.8 hours in the micropec group versus 23 hours in the RIRS group.
Cost effectiveness is an important variable especially in developing countries. Bagcioglu et al. [38] compared flexible ureteroscopy and microperc in terms of costeffectiveness by analyzing 111 procedures. According to their results, the mean total cost of microperc was less than RIRS, driven by the costs of additional required treatments and the ancillary equipment of RIRS eg. DJ stents, guide wires, ureteral access sheaths, and basket catheters. Currently the life expectancy of a flexible ureteroscope is around 21 cases per repair [39] Microperc has the advantage of reusable puncture needle which makes it a more sensible option when it comes to the cost. So far there is no assessment of the durability of microperc instruments.
Microperc would be of interest in select cases of renal stone disease. For microperc to be an appealing alternative to SWL or flexible ureteroscopy it must be fully effective in 1 step with acceptable morbidity (Table 1).
| Study | Patients | Age | Stone size | Hospital stay | Success rate | Haemoglobin drop | Complications |
|---|---|---|---|---|---|---|---|
| Sabnis et al. [35] | Microperc=(n=35) RIRS (n=35) |
Microperc=38.6 ± 14.6 RIRS=43.7 ± 12.1 |
Microperc=1.10 ± 0.23 RIRS=1.04 ± 0.25 |
Microperc=57 ± 22 RIRS=49 ± 18 |
Microperc=97.1% RIRS=94.3% |
Microperc=0.96 ± 0.41 RIRS=0.56 ± 0.31 |
Conversion to miniperc=1 each |
| in MP and RIRS | |||||||
| Intraop complication | |||||||
| Clavien grade 2-pelvic perforation=1 in MP | |||||||
| Postoperative Complication | |||||||
| Clavien grade 1 | |||||||
| Mild hematuria-5 in microperc | |||||||
| Fever 3 in microperc | |||||||
| 4 in RIRS | |||||||
| Tepeler et al. [36] | Microperc (n=21) | 37.3 ± 20.1 (7–69) | 17.8 ± 5.9 (9–29) mm | 37.5 ± 14.4 h | 85.70% | 0.8 ± 0.6 (0.1-2.3) | Complications (n, %) 2 (9.5%) |
| Clavien grade II 1 | |||||||
| Urinary tract infection | |||||||
| Clavien grade IIIa 1 | |||||||
| Renal colic necessitating | |||||||
| Double-J stent insertion | |||||||
| Post-operative renal colic = 2 | |||||||
| Intravasation requiring drain placement=1 | |||||||
| Armagan et al. [37] | RIRS (n=59) and microperc (n=68) | RIRS=49.3 ± 15.3 Microperc=43.6 ± 18. |
RIRS=14.4 ± 3.1 Microperc=13.7 ± 4.2 |
RIRS=23.0 ± 58.1 h Microperc=33.8 ± 17.2 h |
RIRS=44/59-74.5 Microperc=60/68-88.2 |
RIRS=0.68 ± 0.51 Microperc=1.29 ± 0.88 s |
Intractable renal colic (Clavien grade IIIa) |
| RIRS=6 | |||||||
| Microprc=1 | |||||||
| Acute pyelonephritis (Clavien grade I) | |||||||
| RIRS=2 | |||||||
| Microperc=1 | |||||||
| Silay et al. [32] | Microperc (n=19) | 7.5 ± 4.4 years | 14.8 ± 6.8 mm | 1.8 ± 0.8 days | 89.50% | 0.1 ± 0.3 | Post-operative renal colic = 2 |
| Intravasation requiring drain | |||||||
| placement=1 | |||||||
| Hatipoglu et al. [34] | Microperc (n=140) | 28.7 ± 20.6 (1-69) years | 15.1 ± 5.15 (6-32) mm | 1.76 ± 0.65 (1–4) days | 82.14% | 0.87 ± 0.84 (0–4.1) | Overall-20 (14.28%) |
| Clavien grade I | |||||||
| Renal colic-7 | |||||||
| Clavien grade II | |||||||
| Urinary tract infection-3 | |||||||
| Blood transfusion-1 | |||||||
| Clavien grade III-a | |||||||
| Renal colic necessitating D-J stent insertion-1 | |||||||
| Steinstrasse requiring D-J stent insertion-2 | |||||||
| Clavien grade III-b | |||||||
| Steinstrasse requiring D-J stent insertion | |||||||
| (pediatric patients)-3 | |||||||
| Extravasation requiring drain placement-3 |
Table 1: Review of the published studies on the role of microperc in the management of lower caliceal stones.
Microperc and RIRS, both are valid options for the treatment of small lower caliceal stones in adult patients. The stone clearance rates in both microperc and RIRS are comparably high and the complication rates are comparably low. Microperc is associated with more postoperative pain and more fall in the haemoglobin level while RIRS is associated with more intraoperative DJ insertion.