Biochemistry & Pharmacology: Open Access
Open Access
ISSN: 2167-0501
ISSN: 2167-0501
Review Article - (2014) Volume 3, Issue 5
Smoking harms nearly every organ of the body and diminishes a person’s overall health. Millions and millions of peoples have health problems due to habit of smoking. It is now a burden worldwide because smoking addiction of teenagers increasing immensely. Globally, smoking is not only a leading cause of cancer as well as various heart diseases. Smoke contains several carcinogenic pyrolytic products like Polycyclic Aroma0tic Hydrocarbons (PCAH), acrolein etc. are irreversibly binds to DNA, causes genetic mutation and cancer. Various methods exist which allow a smoker to see the impact of their tobacco use, and the immediate effects of quitting. Using biochemical feedback methods include breath carbon monoxide (CO) monitoring, cotinine (metabolite of nicotine) can allow tobacco-users to be identified and assessed, and the use of monitoring throughout an effort to quit can increase motivation to quit. Pharmacologic smoking cessation aids like Nicotine Replacement Therapy (NRT), bupropion, varenicline, cytisine etc. are recommended for all smokers trying to quit. Varenicline appears to be more effective than other available pharmacologic smoking cessation aids. Offering the choice of pharmacologic therapy in addition to supportive counseling, which is now available in the market, should help family physicians achieve greater success assisting their patients with smoking cessation. Family physicians should share the evidence with patients and encourage them to use pharmacologic therapy and counseling to improve the likelihood of success.
<Keywords: Quit smoking, Carcinogenic, Biochemical feedback, Pharmacological feedback
One and all are familiar with “Smoking is injurious to health” and it is a common quote found almost everywhere. Knowing the injurious effects of smoking, don’t be the fool to try it. One more quotation “A cigarette is a pipe with a fire at one end and a fool at the other". Cigarette smoking is addictive and harmful.
Global scenario of tobacco smoking is very pathetic and is a single greatest cause of preventable death [1]. In 2000, smoking was practiced by 1.22 billion people, predicted to rise to 1.45 billion people in 2010 and 1.5 to 1.9 billion by 2025 [2]. It is now a burden worldwide because smoking addiction of teenagers increasing enormously [3]. Rates of smoking have leveled off or declined in the developed world [4] but in developing world, tobacco consumption is rising by 3.4% per year as of 2002 [5].The WHO in 2007 projected 58.8 million deaths to occur globally, from which 5.4 million are tobacco-accredited [6].
It is common believe among teenagers and adults that there are no effects of smoking on their health until they reach middle age [7]. In fact, the latest research shows that the average smoker tries their first cigarette at age 12 and may be a regular smoker by age 14 [8]. On literature survey, it has been found that 90% youths become new regular smokers and failed to quit smoking [9].
Cigarette smoking is a leading cause of cellular damage and alters biochemical functions. Most commonly affecting organs are heart, liver and lungs, etc. (Figure 1). Smoke contains several carcinogenic pyrolytic products that bind to DNA and cause genetic mutations, resulting cancer. Particularly potent carcinogens are Polycyclic Aromatic Hydrocarbons (PCAH), which are toxicated to mutagenic epoxides. Benzopyrene is a member of PCAH, first carcinogenic compound of tobacco smoke causes cancer by irreversibly binds to cellular DNA [10]. body for first time smoking of cigarette but it’s rapidly produce serious medical conditions and health consequences, cited briefly in Table 1. Following immediate effects with various behavioral problems become manifest on cigarette smokers:
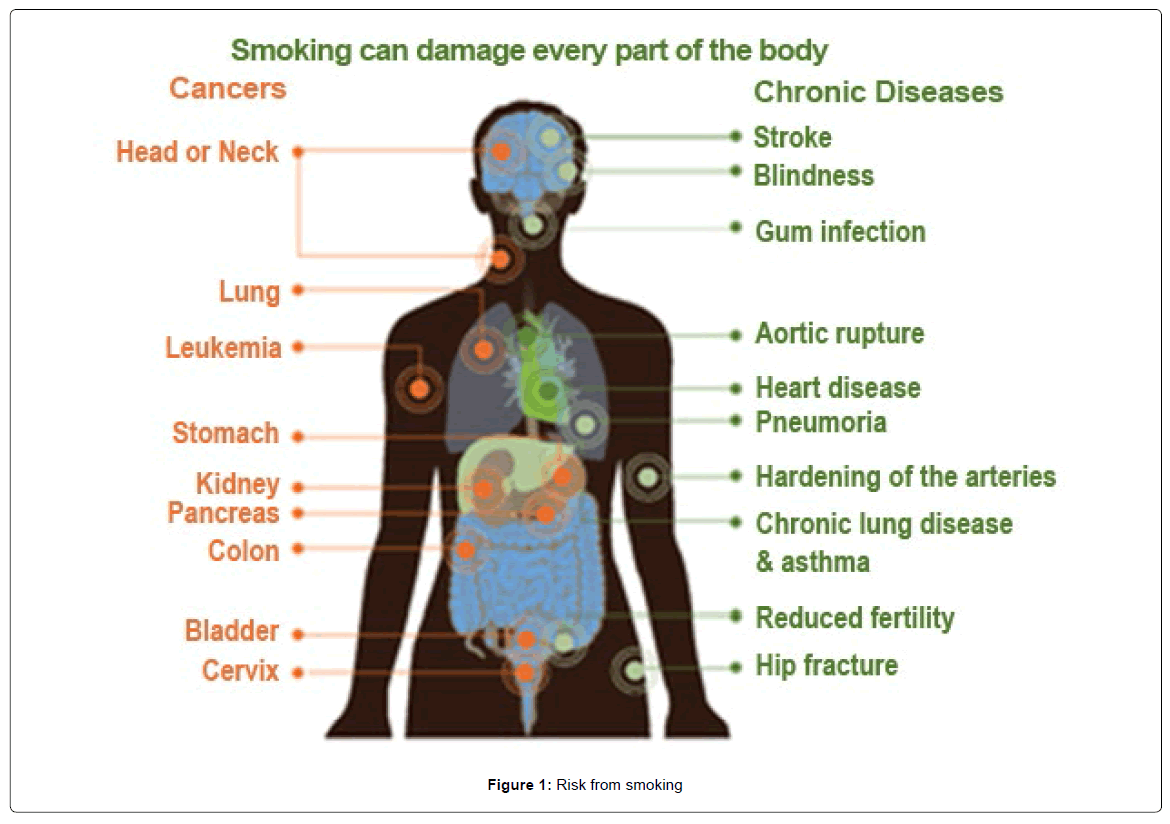
Figure 1: Risk from smoking
| Organ/ System on the body | Major effects |
|---|---|
| Brain | Smoking increases the risk of stroke by at least 50%, which can cause brain damage and death. |
| Heart | Smoking damages the heart and blood circulation, increasing the risk of conditions such as coronary heart disease, heart attack, stroke, peripheral vascular disease and cerebrovascular disease |
| Lungs | Smoking can cause fatal diseases such as pneumonia, emphysema and lung cancer. Smoking causes 84% of deaths from lung cancer and 83% of deaths from chronic obstructive lung disease. |
| Stomach | Smokers have an increased chance of getting stomach cancer or ulcers. |
| Skin | Smoking reduces the amount of oxygen supply to the skin, causes premature ages of skin and makes it three times more likely facial wrinkling, particularly around the eyes and mouth, gives yellow-grey complexion, hollow cheeks and dull. |
| Mouth and throat | Smoking causes bad breath, stained teeth, gum disease and damage sense of taste. More than 93% of oropharangeal cancers (cancer in part of the throat) are caused by smoking. |
| Bones | Smoking can cause the bones to become weak and brittle. Women are more likely to suffer from brittle bones (osteoporosis) than non-smokers. |
| Reproduction and fertility | Smoking can cause male impotence, as it damages the blood vessels that supply blood to the genital organ. It can also damage sperm, reduce sperm count and cause testicular cancer. One study found that the fertility of smoking women was 72% that of non-smokers. |
| Respiratory System | Lung diseases caused by smoking include COPD, which includes emphysema and chronic bronchitis. |
| Cardiovascular System | Smoking damages blood vessels and can make them thicken and grow narrower resulting stroke and coronary heart disease as a leading cause of death in the globe. |
Table 1: Effects of smoking on the body
Studies have shown that smokers feeling better with one or two cigarette on their stress state of life [11]. The feelings of relaxation are more than non-smokers [12]. Routine smoking may continue to change brain chemistry, including decreasing dopamine receptors and thus yielding a more intense desire and risk of addiction [13].
Effects on the Respiratory System
Regular smoker become an asthmatic patients due to bronchospasm which makes airways smaller and leads to wheezing. An asthmatic that starts smoking can severely worsen his/her condition [14]. This effect may develop due to decrease production of mucus in lunges, as an important trapping and clearing agent of chemical and toxic substances. Small “finger like” hairs, called cilia, coat the lung's airways and move rhythmically to clear this mucus from the lungs. Combined with coughing, is also an effective method of clearing the lungs of harmful substances. Tobacco smoke paralyzes these cilia, allowing mucus to collect in the lungs of the smoker [15]. Cigarette smoke also promotes goblet cell growth resulting in an increase in mucus [16]. More mucus is made with each breath of irritating tobacco and the smoker cannot easily clear the increased mucus. The combination of bronchospasm andincreased cilia production result in airway obstruction and decreased lung function, leading to poor breathing performance.
Effects on the Cardiovascular System
Blood pressure means systolic over diastolic pressure, is a measure of tension upon the walls of arteries by blood. It has been reported that nicotine consumption increases blood pressure [16]. Older male smokers have been found to have higher systolic blood pressure than non-smokers [17]. The higher pressure can also cause organ damage where blood is filtered, such as in the kidneys [18]. Smoking causes blood vessel constriction and transient reduction in blood supply followed by increased risk of stroke or heart attack due to either by decreasing the nitric oxide (NO) or increasing the endothelin-1 (ET- 1) [19]. Nicotine consumption increases a resting heart rate, as soon as 30 minutes after puffing; and the higher the nicotine consumption (through deep inhalation or increased number of cigarettes) the higher the heart rate [20]. Nicotine damages the blood vessel walls, which allow plaques to form at a faster rate than they would in a non-smoker, resulting atherosclerosis [21]. In addition, a recent study in Japan showed a measurable decrease in the elasticity of the coronary arteries of nonsmokers after just 30 minutes of exposure to second hand smoke [14]. Smoking is also one of the main causes to damage blood vessel with clot formation, resulting thrombosis due to elevated levels of thrombin, an enzyme that causes the blood to clot, immediately after smoking [22].
Current view that HDL (High Density Lipoprotein) is beneficial whereas LDL (Low Density Lipoprotein) can be harmful to the body due its impairing blood flow effect to heart, brain and other organs. Nicotine increases the amount of LDL in the blood vessels and decreases the amount of HDL. These silent effects begin immediately and greatly increase the risk for heart disease and stroke [23].
Effects on the Gastrointestinal System
The gastrointestinal system includes the mouth, esophagus, stomach, small and large intestines, and the anus, are all easily affected by tobacco smoke. Most common symptoms of heartburn and acid regurgitation from the stomach due to decrease base secretion and defective counteract digestive mechanism. The base smoker’s bodies secrete is less neutralizing than nonsmokers and thus allows digestive acids a longer period of time to irritate the esophagus [24]. These immediate changes in base secretion and esophagus/stomach communication cause painful heartburn and result in an increased risk of long term inflammation and dysfunction of the esophagus and stomach [25] , resulting peptic ulcer [26] . Mucus is produced in the stomach to provide a protective barrier between stomach acid and cells of the stomach.Mucous production in the stomach is inhibited by smoking [27]. Smoking also decreases blood flow to the inner layer of the esophagus, stomach and small intestine [23].
To maintain good health need proper digestion and absorption of macro and micro-nutrients in the body. Any abnormality in metabolic processes may be a cause of serious health problem. Smoking interferes with the absorption of a number of micronutrients, especially vitamins C, E, and folic acid that can result in deficiencies of these vitamins [28]. A deficiency in Vitamin C can lead to scurvy which is a disease characterized by weakness, depression, inflamed gums, poor wound healing, and uncontrolled bleeding [29]. Vitamin E deficiency may cause blood breakdown, eye disease, and irreversible nerve problems of the hands, feet, and spinal cord [28]. Folic acid deficiency may result in long-lasting anemia, diarrhea, and tongue swelling [28].
Reactive oxygen species are generated through various metabolic processes and destroyed by antioxidants, including vitamins A, C, and E, otherwise they are likely contributing to the development of cancer, heart disease, and cataracts [30]. Oxidants also speed up blood vessel damage due to atherosclerosis [31]. This increase in antioxidant consumption reduces the levels of antioxidants such as alpha-tocopherol, the active form of vitamin [32]. But this scenario is completely changed after smoking due to decrease level antioxidant in blood and resulting immediate cell, gene, and blood vessel damage [33]. Smoking immediately causes oxidant stress in blood while the antioxidant potential is reduced because of this stress [34].
Effects on the Renal System
Smoking is a well-known cause for many diseases and it was recently proven to play an important role in renal disease. Studies showed that cigarette smoking is a one of the risk factor for development and progression of chronic renal disease in community [35].
Effect on the reproductive system
Approximately 85% male smokers are impotence and suffer erectile dysfunction [36]. Smoking causes impotence because it promotes arterial narrowing [37]. Smoking is not only harmful to male, it also affects potentially in female infertility. Possible mechanisms include tubal changes, defective folliculogenesis, decrease ovulation, low embryo transport, less endometrial receptivity, decrease uterine blood flow and the uterine myometrium [38].
Effect on oral cavity
Smoking causes a variety of cancers including cancers of the oral cavity (lip, tongue, mouth, and throat), esophagus, larynx, and lung [39].Smokers not only have significantly greater loss of tooth but also face in the staining of teeth and bed breath [40].
• Breath carbon monoxide (CO) monitoring:Carbon monoxide concentration in breath has been shown to be directly correlated with the CO concentration in blood of smoker. Within hours of quitting, CO concentrations show a noticeable decrease [51].
• Cotinine: A metabolite of nicotine, cotinine is present in smokers and can be used as a reliable biomarker to determine smoking status [52].
• Lipid profile: The lipid profiles include serum total cholesterol, triglycerides; LDL, VLDL and HDL are raised in smokers which may lead to higher incidence of cardiovascular disease [53].
• Salivary parameters:Salivary globulin and C - reactive protein are important parameters for the study of periodontal
• Breath carbon monoxide (CO) monitoring:Carbon monoxide concentration in breath has been shown to be directly correlated with the CO concentration in blood of smoker. Within hours of quitting, CO concentrations show a noticeable decrease [51].
• Cotinine: A metabolite of nicotine, cotinine is present in smokers and can be used as a reliable biomarker to determine smoking status [52].
• Lipid profile: The lipid profiles include serum total cholesterol, triglycerides; LDL, VLDL and HDL are raised in smokers which may lead to higher incidence of cardiovascular disease [53].
• Salivary parameters:Salivary globulin and C - reactive protein are important parameters for the study of periodontal health and smoking status [54].
Pharmacological feedback
Pharmacologic smoking cessation aids are recommended for all smokers trying to quit, unless contraindicated. The screening data indicates some useful medicines are now in the market as pharmacologic smoking cessation aids [55].
• Nicotine replacement therapy (NRT):Nicotine gum, patches, and inhalers, are effective therapeutic aids in smoking cessation [56]. A systematic review and meta-analysis, which reviewed randomized trials of NRT compared with placebo or no treatment, showed increased the chances of stopping smoking by 50 to 70% [57]. All nicotine products may cause side effects include: Headaches, Nausea and other digestive problems
• Bupropion: Bupropion (Zyban) was launched as a smoking cessation aid in 1997 in the United States and has been approved in more than 50 countries [58,59]. In a systematic review and meta-analysis of 31 bupropion trials in which bupropion was the sole agent used for cessation, with 6 months follow-up or longer, the reviewers found the possibility of cessation almost doubled with bupropion therapy [60]. Bupropion alone or in combination with the nicotine patch has been found to significantly increase long-term cessation rates compared with the patch alone [61]. Bupropion blocks the reuptake of dopamine and norepinephrine, which is thought to be the mechanism behind its effect on smoking cessation [62]. The side effects occur when taking bupropion like anxiety , irregular heartbeats,dry mouth, irritability , restlessness , headache , skin rush, confusion etc.
• Varenicline: Varenicline (Champix) was introduced in Canada in April 2007 [63]. Varenicline is the first partial agonist of the α4β2 nicotinic acetylcholine receptor to be developed. The dependency effects of nicotine are thought to be mediated at these receptors [64]. Cochrane review of 15 studies found that varenicline was significantly superior to bupropion at one year but that varenicline and nicotine patches produced the same level of abstinence at 24 weeks [65]. Nausea occurs commonly in people taking varenicline. Other less common side effects include headache, difficulty sleeping, and abnormal dreams. Rare side effects reported by people taking varenicline compared to placebo include change in taste, vomiting, abdominal pain, flatulence, and constipation.
• Cytisine: Cytisine (Tabex) is a plant extract that was the first medication approved as an aid to smoking cessation, and has very few side effects in small doses [66]. The clinical studies showed a good tolerance to the drug and grave adverse effects were not observed. The following adverse effects are rather often observed at the beginning of Tabex treatment: changes in both taste and appetite, dryness in the mouth, headache, irritability, nausea, constipation, tachycardia, light elevation of the arterial pressure.
• Moclobemide: 3 months continuous moclobemid medication had a much higher successful quit rate those in the placebo group [67]. This medication may initially cause dizziness, nervousness, mild headache, trouble sleeping and nausea as your body adjusts to the medication. Other side effects reported include sweating, loss of appetite, dry mouth, anxiety or blurred vision.
• Clonidine: It may have approximately doubles abstinence rates, but it can cause high blood pressure and side effects include dry mouth and sedation [68]. The principle adverse effects of clonidine are dry mouth, dizziness, hypotension and drowsiness Dizziness, lightheadedness
• Nortriptyline: It is a second-generation tricyclic antidepressant, has similar success rates to bupropion but has side effects including include dry mouth, sedation, constipation, and increased appetite, mild blurred vision, tinnitus, often euphoria and mania [67]. Drowsiness, dizziness, dry mouth, blurred vision, constipation, weight gain, or trouble urinating may occur.
Smoking is addictive and harmful to every organ of the body. It is now a cause of cancer and death from cancer. This worldwide burden is now a big challenge “how to quit smoking” and improves person’s overall health. Offering the choice of pharmacologic therapy in addition to supportive counseling, which is now available in the market, should help family physicians achieve greater success assisting their patients with smoking cessation. Family physicians should share the evidence with patients and encourage them to use pharmacologic therapy and counseling to improve the likelihood of success