Endocrinology & Metabolic Syndrome
Open Access
ISSN: 2161-1017
ISSN: 2161-1017
Research Article - (2018) Volume 7, Issue 5
Background: Adolescent Obesity is causing serious public health concern and in many countries threatening the viability of basic health care delivery. Many co-morbid conditions are seen in association with adolescent obesity. Interventions based on Yoga principles are found to have effective solutions for adolescent obesity.
Aim: To evaluate the effect of the Yoga based intervention on anthropometric and physical assessments in Adolescent Obesity
Methods: RCT (Randomized Controlled Trial) was conducted on 53 obese adolescents for 40 days. Special yoga based training Program was conducted for yoga group. Parameters like weight, Body Mass Index (BMI) parameters, pulse rate, blood pressure, MAC (Mid Upper Arm Circumferences), Ac (Abdominal Circumference), Waist Circumference (WC), HC (Hip Circumference) along with physical tests like sit ups and Flamingo balance tests were assessed before and after intervention for both yoga and control groups. Within and between groups analyses of the variables were analysed.
Result: The study showed significant reduction in weight, body mass index, Hip circumference, and total body fat percentage, subcutaneous fat throughout the body in yoga group and percentage of improvement is more in yoga group than that of control group.
Conclusion: Yoga based intervention is effective to reduced obesity in adolescent children with respect to anthropometric and physical assessments.
Keywords: Obesity; Adolescence; Yoga
Adolescent obesity
Overweight and obesity are metabolic conditions in which abnormal or excessive fat accumulation is found to impair health. In 2016, more than 1.9 billion adults aged 18 years and older were overweight. Of these over 650 million adults were obese. The worldwide prevalence of obesity nearly tripled between 1975 and 2016. The prevalence of overweight and obesity among children and adolescents aged 5-19 years has risen dramatically from just 4% in 1975 to just over 18% in 2016. The rise has occurred similarly among both boys and girls: in 2016 18% of girls and 19% of boys were overweight [1]. Obesity leads to adverse impacts on physical as well as psychological functions of the person. Energy-dense overeating, nutrient-poor foods and a sedentary lifestyle have led to an epidemic of obesity all over the world. Apart from physical problems there are issues which affect psychological well-being of an individual [2]. Children in low- and middle-income countries are more prone to inadequate pre-natal, infant and young child nutrition. At the same time, they are exposed to high-fat, high-sugar, high-salt, energy-dense, micronutrient-poor foods. These dietary patterns in conjunction with lower levels of physical activity, result in sharp increases in childhood obesity while under nutrition issues remain unsolved [3].
Assessment of obesity in adolescence
Obesity is a commonly used term with a wide range of meanings with no widely accepted diagnostic definitions or cut-off points are available for children. Mean body fat percentages and percentile curves are available for children 5 to 18 years of age [4]. Several studies have recommended BMI as the preferred measure for evaluating obesity among adolescents 2 to 19 years of age. BMI can be correlated strongly with body fat percentage as it is associated weakly with height, and it identifies the fattest individuals correctly, with acceptable accuracy at the upper end of the distribution like 85th or 95th percentile for age and gender. In 1994, the Expert Committee on Clinical Guidelines for Overweight in Adolescent Preventive Services recommended that children whose BMI exceeds 30 kg/m2 or is more than 95th percentile for age and gender should be considered obese [5].
BMI is a fairly reliable indicator of body fatness for most people. BMI does not measure boy fat directly, but research has shown that BMI correlates to direct measures of body fat. BMI can be considered an alternative for direct measures of body fat. Additionally, BMI is an inexpensive and easy-to-perform method for screening for weight categories that may lead to health problems. Measuring children’s BMI regularly is the first step to maintaining a healthy weight. BMI being an important variable, the full body sensor, composition monitor and scale is used to calculate BMI and other BMI parameters. Full Body Sensing provides a comprehensive understanding of the body composition. The BMI machine calculates the estimated values for body fat percentage, skeletal muscle percentage, resting metabolism and subcutaneous fat in different body parts like arms, trunk, and legs using the BI (Bioelectrical Impedance) Method. The monitor also calculates the BMI (Body Mass Index) and body age as well as weight. Resting metabolism is the energy required to maintain vital functions. The total amount of energy used by the body in a typical day contributes resting metabolism (60%-70%), daily activity metabolism (20%-30%) and diet-induced thermogenesis (10%). If less energy is consumed by resting metabolism that can be consumed by daily activity metabolism. Percentage of subcutaneous fat and skeletal muscles are inversely proposal to each other. Skeletal muscle is the type of muscle that can see and feel. Building skeletal muscle can help prevent rebound weight gain. The maintenance and increase of skeletal muscle is closely linked to resting metabolism rate.
Along with BMI, waist circumference in children provides a better estimate of visceral adipose tissue [6,7]. Alternative measures that account for fat distribution include abdominal circumference, hip circumference and mid arm circumference. EUROFIT tests are also one of the assessment tools in adolescent obesity to check physical fines. The measurement of physical fitness for each child helps them to develop positive attitudes towards their bodies and get information about their physical status [8]. Handgrip strength, standing broad jump, flexed arm hang, sit‐ups, sit‐and‐reach and Flamingo balance tests are few EUROFIT tests out of which sit‐ups and Flamingo balance tests are significant in adolescent obesity.
Yoga for adolescent obesity
A study consisted of 709 healthy children (with mean age=8.9 ± 1.6 years) suggest that overweight and obesity are limiting factors for fitness performance in adolescence. Interventions promoting children’s health should, ideally, begin early in life and involve measures that simultaneously improve fitness and lower fatness [9]. Yoga is widely recognized as an effective tool in maintaining a healthy lifestyle resulting as a vaccine against lifestyle related disorders [10]. According to a study of effect of aerobic & resistance exercise on physical fitness conducted on 60 adolescent obese participants in Karnataka (India), aerobic and resistance exercise in combination reduces fat significantly [11]. But only physical activity has limited scope of correcting the causes of obesity in preadolescence. Other than physical causes like lack of physical exercise, genetic and sedentary lifestyle there are few psychological causes of obesity like low selfesteem, depression, failures to cope up to demanding situations are also not uncommon. The negative experiences in school and at home leads to lower self-esteem found in childhood obesity [12]. Home, child care centre, school, and community environments can influence children's behaviours related to food intake and physical activity also which is a contributing factor of causes of obesity [13]. Along with this, increasing academic stress is also a contributing factor in causes of obesity [14]. Any form of physical activity having limited scope to manage this supportive cause of obesity can manage weight for short duration but fails to provide long termed constant impacts in preadolescence obesity. Whereas Yoga based programs have a wider impact on body, mind, habits, perception and cognition also.
In one month randomized control trial of impact of Yoga on selfesteem in 44 adolescent participants in Hardwar (India), it is noted that the level of self-esteem has significantly increased with experimental group [15]. Yoga lays great significance on strengthening inherent defensive mechanisms of human body and mind. It develops immunity and resistance in human body and helps the body and mind in attaining homeostatic balance. The strengthening of defence mechanism and harmony between mind and body prevents causes of psychosomatic disorders like obesity. The aim of yoga therefore is also the attainment of physical, mental, social and spiritual health [16]. A study conducted on Effect of yoga and physical exercise on physical, cognitive and emotional measures in 98 school children, it is observed that Physical exercise and yoga have different ways of influencing physical fitness, cognitive performance and self-esteem. Both ways showed significant improvements in tests for physical fitness [17]. But, this study has two independent groups without control group and represents geographically north part of India. The findings could be the possible effects of the two interventions, with a degree of uncertainty due to the absence of a control group. There was a need to check generalizability of the findings in a sample drawn from diverse geo-graphical and cultural backgrounds with control group. So, current study was designed to evaluate the effect of validated and feasible yoga based intervention on anthropometric and physical assessments in Adolescent Obesity.
The complete study has been approved by ethical committee of Swami Vivekananda Yoga Anusandhan Samsthana, Bangalore (Figure 1). 1400 students including both genders were screened from age of 9 year to 14 year (standard 5 to 9) in one of the reputed school in Pune city of Maharashtra state in India. Height, weight and BMI of all the students were recorded and obese participants (Figure 2) having BMI >95th percentile were included who were ready to participate in the study with written consent. Participants having any physical disability, any psychosomatic disorder, consuming any medical drugs and exposed to yoga within last 6 months were excluded from the study. All the participants are randomly divided in two groups. Yoga group (n=30) and control group (n=30). RCT (Randomized Controlled Trial) was conducted on 60 obese adolescents for 40 days. Special yoga based training Program was conducted for yoga group. Yoga intervention was consisting of specially designed and validated yoga protocol of 60 minutes duration which included set of loosening exercises, asanas, pranayamas, suryanamskara, breathing practises and meditation.
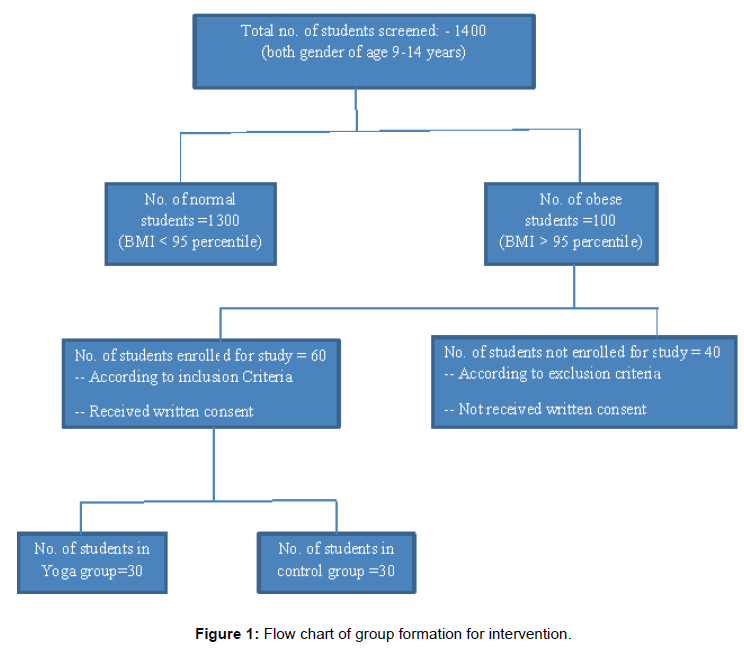
Figure 1: Flow chart of group formation for intervention.
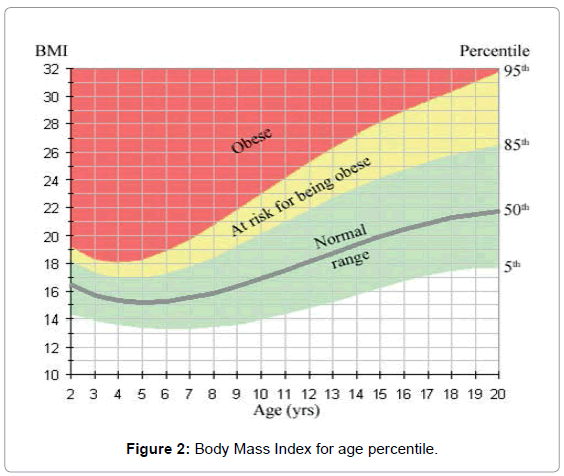
Figure 2: Body Mass Index for age percentile.
This intervention was conducted for 5 days a week for 40 days. 4 sessions of chanting, Karmayoga, Yoga counselling was also provided. Participants of Yoga group were regular in throughout the intervention and maintained 90 percent of attendance. Control group was under observation with normal routine. The diet regulation was only provided for both yoga and control group in order to acquire uniform base with respect to diet. Parameters like weight, pulse rate, blood pressure, MAC (Mid Upper Arm Circumferences), AC (Abdominal Circumference), WC (Waist Circumference), HC (Hip Circumference) along with physical tests like sit ups per minute and Flamingo balance test were assessed before and after intervention for both yoga and control groups. Body Mass Index (BMI) parameters like total body fat percentage, resting metabolism, subcutaneous fat and muscle percentage of whole body, arms, trunk and legs region also calculated using Body composition monitor Model HBF-701 before and after intervention for both yoga and control groups. In yoga group, there were 5 drop outs and from control group 2 children were absent for post parameter collection.
The data was analysed using SPSS software 20 version. Normality test was done using Shapiro Wilk test. The paired sample t test was conducted for pre & post variables which were found normally distributed for both the groups. For not normally distributed variables, Wilcoxon signed ranks test was done. Between groups analysis was done using independent sample t test for the post values of both the groups.
The baseline demographic data of age and height of the yoga and control group is described in Table 1. Results of within group analysis of Yoga group are given in Table 2. Parameters like abdominal circumference, waist circumference, hip circumference, total body fat percentage, trunk subcutaneous fat, trunk muscle percentage, legs subcutaneous fat, legs muscle percentage and situps per minute were normally distributed. Hip circumference (p=0.001), total body fat percentage (p=0.001), trunk subcutaneous fat (p=0.005) and legs subcutaneous fat (p=0.03) reduced significantly whereas abdominal circumference (p=0.376) reduced but without significance. Trunk muscle percentage (p=0.021) increased significantly. Waist circumference (p=0.553) increased but without significance. Whole body muscle percentage (p=0.076) and legs muscle percentage (p=0.187) increased but without significance. Number of situps per minute (p=0.566) is decreased but without significance.
| NO. | GROUP | YOGA | CONTROL | ||
|---|---|---|---|---|---|
| 1 | Gender | Male | Female | Male | Female |
| 13 | 17 | 14 | 16 | ||
| 2 | Average Age (years) | 11 ± 1.4 | 11 ± 1.3 | ||
| 3 | Average Height (cm) | 152.91 ± 6.97 | 152.71 ± 9.18 | ||
| 4 | Average Weight (Kg) | 63.86 ± 15.52 | 62.39 ± 14.21 | ||
| 5 | Average BMI (Kg/m2) | 27.16 ± 5.04 | 26.43 ± 3.53 | ||
Table 1: The baseline demographic data of age and height of the yoga and control group.
| No. | Variable | Mean (Pre) |
Mean (Post) |
t/z value | p value |
|---|---|---|---|---|---|
| 1 | Weight | 63.86 ± 15.52 | 63.14 ± 15.28 | 2.359a | 0.018* |
| 2 | BMI | 27.16 ± 5.04 | 26.47 ± 4.85 | 3.344a | 0.001* |
| 3 | Pulse rate | 95.5 ± 11.7 | 97.37 ± 14.48 | 0.529a | 0.597 |
| 4 | Systolic blood pressure | 125.16 ± 11.06 | 122.87 ± 13.42 | 1.037a | 0.30 |
| 5 | Diastolic blood pressure | 81 ± 6.83 | 77.26 ± 17.63 | 1.712a | 0.087 |
| 6 | Mid arm circumference | 11.23 ± 1.03 | 11.07 ± 0.93 | 0.716a | 0.474 |
| 7 | Abdominal circumference | 35.89 ± 3.69 | 35.5 ± 3.77 | 0.902b | 0.376 |
| 8 | Waist circumference | 37.65 ± 4.48 | 37.77 ± 4.81 | 0.602b | 0.553 |
| 9 | Hip circumference | 39.49 ± 4.63 | 38.21 ± 4.71 | 3.68b | 0.001* |
| 10 | Total body fat percentage | 29.83 ± 3.46 | 27.76 ± 2.72 | 4.40b | 0.001* |
| 11 | Resting metabolism | 1382.83 ± 205.34 | 1404.33 ± 263.73 | 1.33a | 0.183 |
| 12 | Subcutaneous fat (Whole body) | 25.57 ± 5.58 | 21.96 ± 4.32 | 2.57a | 0.01∞ |
| 13 | Muscle percentage (Whole body) | 27.13 ± 3.51 | 28.26 ± 2.89 | 1.77b | 0.076 |
| 14 | Subcutaneous fat (Arms) | 39.23 ± 8.58 | 34.62 ± 6.47 | 2.315a | 0.021∞ |
| 15 | Muscle percentage (Arms) | 31.01± 6.78 | 33.98 ± 5.07 | 2.032a | 0.042∞ |
| 16 | Subcutaneous fat (Trunk) | 22.21 ± 5.35 | 19.23 ± 3.29 | 3.085b | 0.005∞ |
| 17 | Muscle percentage (Trunk) | 20.58 ± 2.97 | 21.55 ± 2.20 | 2.480b | 0.021∞ |
| 18 | Subcutaneous fat (Legs) | 38.35 ± 8.27 | 34.27 ± 6.29 | 2.307b | 0.03∞ |
| 19 | Muscle percentage (Legs) | 41.94 ± 5.21 | 43.94 ± 4.65 | 1.359b | 0.187 |
| 20 | Sit ups | 32.95 ± 7.02 | 31.5 ± 9.38 | 0.582b | 0.566 |
| 21 | Flamingo Balance test | 60.70 ± 37.07 | 65.75 ± 38.48 | 1.845a | 0.065 |
aWilcox test
bPaired sample t test
*significant at 0.01
∞significant at 0.05
Table 2: Result of within group analysis of Yoga group (n= 25).
Parameters like weight, BMI, mid arm circumference, pulse rate, systolic blood pressure, diastolic blood pressure, resting metabolism, whole body subcutaneous fat, arm subcutaneous fat, arm muscle percentage and flamingo balance test were not normally distributed. Weight (p=0.018), BMI (p=0.001), whole body subcutaneous fat (p=0.01), arm subcutaneous fat (p=0.021) reduced significantly whereas systolic blood pressure (p=0.30), diastolic blood pressure (p=0.087) and mid arm circumference (p=0.474) reduced but without significance. Muscle percentage of arms (p=0.042) increased significantly whereas pulse rate (p=0.597), Flamingo balance test (p=0.065) increased but without significance.
A result of within group analysis of Control group is given in Table 3. Parameters like abdominal circumference, waist circumference, hip circumference, total body fat percentage, trunk subcutaneous fat, trunk muscle percentage, legs subcutaneous fat, legs muscle percentage and sit ups per minute were normally distributed. Number of sit ups per minute (p=0.023) decreased significantly whereas abdominal circumference (p=0.730), hip circumference (p=0.226), total body fat percentage (p=0.876), trunk subcutaneous fat (p=0.186) and legs subcutaneous fat (p=0.162) reduced but without significance. Waist circumference (p=0.244), trunk muscle percentage (p=0.427) and legs muscle percentage (p=0.270) increased but without significance.
| No. | Variable | Mean Pre value | Mean Post value | t value | p value |
|---|---|---|---|---|---|
| 1 | Weight | 62.39 ± 14.21 | 62.8 ± 14.73 | 1.646a | 0.100 |
| 2 | BMI | 26.43 ± 3.53 | 26.82 ± 3.58 | 0.108a | 0.914 |
| 3 | Pulse rate | 95.07 ± 12.7 7 | 93.85 ± 11.31 | 0.781a | 0.435 |
| 4 | Systolic blood pressure | 125.96 ± 18.54 | 119.25 ± 13.68 | 2.596a | 0.009∞ |
| 5 | Diastolic blood pressure | 83.71 ± 9.78 | 77.5 ± 8.05 | 2.90a | 0.004∞ |
| 6 | Mid arm circumference | 11.21 ± 1.37 | 11.35 ± 1.42 | 1.160a | 0.246 |
| 7 | Abdominal circumference | 35.51 ± 3.27 | 35.42 ± 3.28 | 0.348b | 0.730 |
| 8 | Waist circumference | 36.50 ± 3.01 | 36.99 ± 3.67 | 1.192b | 0.244 |
| 9 | Hip circumference | 38.84 ± 3.71 | 38.57 ± 3.93 | 1.240b | 0.226 |
| 10 | Total body fat percentage | 29.02 ± 2.65 | 28.96 ± 2.17 | 0.157b | 0.876 |
| 11 | Resting metabolism | 1369.25 ± 218.60 | 1388.33 ± 238.43 | 1.287a | 0.198 |
| 12 | Subcutaneous fat (Whole body) | 24.80 ± 5.11 | 22.75 ± 4.56 | 1.150a | 0.250 |
| 13 | Muscle percentage (Whole body) | 27.20 ± 3.06 | 28.12 ± 2.93 | 1.059a | 0.290 |
| 14 | Subcutaneous fat (Arms) | 38.90 ± 8.16 | 36.02 ± 7.03 | 0.997a | 0.319 |
| 15 | Muscle percentage (Arms) | 30.62 ± 7.27 | 33.47 ± 6.61 | 1.261a | 0.207 |
| 16 | Subcutaneous fat (Trunk) | 21.34 ± 4.32 | 20.07 ± 3.52 | 1.359b | 0.186 |
| 17 | Muscle percentage (Trunk) | 20.87 ± 2.40 | 21.2 ± 2.08 | 0.806b | 0.427 |
| 18 | Subcutaneous fat (Legs) | 38.75 ± 8.81 | 35.92 ± 7.71 | 1.439b | 0.162 |
| 19 | Muscle percentage (Legs) | 42.06 ± 4.94 | 43.78 ± 4.95 | 1.128b | 0.270 |
| 20 | Sit ups | 30.21 ± 8.74 | 26.78 ± 7.36 | 2.419b | 0.023∞ |
| 21 | Flamingo Balance test | 72.17 ± 56.41 | 91.89 ± 58.65 | 1.173a | 0.241 |
aWilcox test
bPaired sample t test
∞significant at 0.05
Table 3: Result of within group analysis of Control group (n=28).
Parameters like weight, BMI, mid arm circumference, pulse rate, systolic blood pressure, diastolic blood pressure, resting metabolism, whole body subcutaneous fat, arm subcutaneous fat, arm muscle percentage and flamingo balance test were not normally distributed Table 4.
| No. | Variable | Yoga Group (n= 25) |
Control Group (n= 28) |
t value | p value | ||
|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | ||||
| 1 | Weight | 63.86 ± 15.52 | 63.14 ± 15.28 | 62.39 ± 14.21 | 62.8 ± 14.73 | 0.517a | 0.60 |
| 2 | BMI | 27.16 ± 5.04 | 26.47 ± 4.85 | 26.43 ± 3.53 | 26.82 ± 3.58 | 0.053a | 0.95 |
| 3 | Pulse rate | 95.5 ± 11.7 | 97.37 ± 14.48 | 95.07 ± 12.7 7 | 93.85 ± 11.31 | 1.052 a | 0.29 |
| 4 | Systolic blood pressure | 125.16 ± 11.06 | 122.87 ± 13.43 | 125.96 ± 18.54 | 119.25 ± 13.68 | 0.883a | 0.37 |
| 5 | Diastolic blood pressure | 81 ± 6.83 | 76.95 ± 8.79 | 83.71 ± 9.78 | 77.5 ± 8.05 | 0.330a | 0.74 |
| 6 | Mid arm circumference | 11.23 ± 1.03 | 11.07 ± 0.93 | 11.21 ± 1.37 | 11.35 ± 1.42 | 0.027a | 0.97 |
| 7 | Abdominal circumference | 35.89 ± 3.69 | 35.5 ± 3.77 | 35.51 ± 3.27 | 35.42 ± 3.28 | 0.530b | 0.05∞ |
| 8 | Waist circumference | 37.65 ± 4.48 | 37.77 ± 4.81 | 36.50 ± 3.01 | 36.99 ± 3.67 | 0.593b | 0.79 |
| 9 | Hip circumference | 39.49 ± 4.63 | 38.21 ± 4.71 | 38.84 ± 3.71 | 38.57 ± 3.93 | 2.479b | 0.54 |
| 10 | Total body fat percentage | 29.83 ± 3.46 | 27.76 ± 2.72 | 29.02 ± 2.65 | 28.96 ± 2.17 | 3.236b | 0.92 |
| 11 | Resting metabolism | 1382.83 ± 205.34 | 1404.33 ± 263.33 | 1369.25 ± 218.60 | 1388.33 ± 238.43 | 0.579 a | 0.56 |
| 12 | Subcutaneous fat (Whole body) | 25.57 ± 5.58 | 21.96 ± 4.32 | 24.80 ± 5.11 | 22.75 ± 4.56 | 0.606 a | 0.54 |
| 13 | Muscle percentage (Whole body) | 27.13 ± 3.51 | 28.26 ± 2.89 | 27.20 ± 3.06 | 28.12 ± 2.93 | 0.036a | 0.97 |
| 14 | Subcutaneous fat (Arms) | 39.23 ± 8.58 | 34.62 ± 6.47 | 38.90 ± 8.16 | 36.02 ± 7.03 | 0.383a | 0.70 |
| 15 | Muscle percentage (Arms ) | 31.01± 6.78 | 33.98 ± 5.07 | 30.62 ± 7.27 | 33.47 ± 6.61 | 0.330a | 0.74 |
| 16 | Subcutaneous fat (Trunk) | 22.21 ± 5.35 | 19.23 ± 3.29 | 21.34 ± 4.32 | 20.07 ± 3.52 | 1.241b | 0.88 |
| 17 | Muscle percentage (Trunk) | 20.58 ± 2.97 | 21.55 ± 2.20 | 20.87 ± 2.40 | 21.2 ± 2.08 | -1.637b | 0.36 |
| 18 | Subcutaneous fat (Legs) | 38.35 ± 8.27 | 34.27 ± 6.29 | 38.75 ± 8.81 | 35.92 ± 7.71 | - 0.278b | 0.77 |
| 19 | Muscle percentage (Legs) | 41.94 ± 5.21 | 43.94 ± 4.65 | 42.06 ± 4.94 | 43.78 ± 4.95 | - 0.701b | 0. 14 |
| 20 | Sit ups | 32.95 ± 7.02 | 31.5 ± 9.38 | 30.21 ± 8.74 | 26.78 ± 7.36 | - 0.942b | 0.09 |
| 21 | Flamingo Balance test | 60.70 ± 37.07 | 65.75 ± 38.48 | 72.17 ± 56.41 | 91.89 ± 58.65 | 1.568a | 0.11 |
aMann-Whitney U test
bIndependent samples t-test
∞significant at 0.05
Table 4: Result of In between group analysis.
Systolic blood pressure (p=0.009), diastolic blood pressure (p=0.004) reduced significantly whereas pulse rate (p=0.435), whole body subcutaneous fat (p=0.250), arm subcutaneous fat (p=0.319) reduced but without significance. Weight (p=0.100), BMI (p=0.914), mid arm circumference (p=0.246), resting metabolism (p=0.198), whole body muscle percentage (p=0.290) and Flamingo balance test (p=0.241) increased but without significance.
Analysis of in between Yoga and control group states that abdominal circumference of Yoga group is decreased significantly than that of Control group (p=0.05). Weight, BMI, mid-arm circumference, hip circumference, total body fat percentage, subcutaneous fat of whole body, arm, trunk and legs has been reduced more in Yoga group than that of Control group but without significance. Number of situps, systolic blood pressure and diastolic blood pressure is decreased in control group more than that of Yoga group but without significance. Pulse rate is found to be increased in Yoga group whereas that of control group is reduced but without significance. Waist circumference is increased more in control group than that of Yoga group but without significance. Resting metabolism, muscle percentage of whole body, arm, trunk and legs are increased more in Yoga group than that of Control group but without significance. Flamingo balance test has been increased more in control group than that of Yoga group but without significance.
Obesity especially abdominal is related to academic achievement and cognitive functions in children. Visceral adipose tissues have negative impact on cognitive functions leading to academic decrease among children with obesity because of its dangerous metabolic nature [18].
Excessive adipose tissue also affects the physical inactivity leading to psychological increased sensitivity. These childhoods obesity leaded poorer cognitive function results in decreased measures of intra individual response, even after accounting for intellectual abilities, aerobic fitness [19]. So focus of this study was to evaluate the yoga based validated intervention on anthropometric and physical variables in adolescent Obesity [20]. Specific anthropometric and physical tests are selected as variables were selected in order to conserve comfort and convenience of the participants with average age of 11 ± 1.4 years. Hip circumference, total body fat percentage, subcutaneous fat of trunk and legs whereas these parameters are reduced in control group but without significance. Subcutaneous fat reduction leads to significant increase of muscle percentage of trunk and leg region. This provides evidence of efficacy of validated yoga based intervention on reduction of adipose tissues in hip, trunk and leg region resulting in reduction of total body fat percentage and overall body weight. Abdominal circumference is reduced significantly in Yoga group and without significance in control group. Yoga group has improved significantly better in this parameter than control group. Yoga intervention practices like dynamic surya namaskara, asana, loosening practices are focused to reduced abdominal adipose tissue. According to one RCT, yoga intervention had moderately strong positive effects on anthropometric variables in women with abdominal obesity. Yoga is safe in women and can be recommended as a technique for combating abdominal obesity in women [21]. Our study provides efficacy of Yoga in same concern in adolescent population. Yoga improves emotional wellbeing in children. The mechanisms underlying these benefits have not been clearly worked out and may involve complex neuro-chemical changes and modified functioning of brain areas within the limbic circuit. Physical activities of control group was not monitored and compared with test group. This is limitation of the study.
Yoga based intervention is effective to reduced obesity in adolescent children with respect to anthropometric and physical assessments. This study provides evidence to prove efficacy of Yoga to manage increased subcutaneous adiposity in trunk, hip and leg region resulting in weight reduction in adolescent children.
We are thankful to Mr. Ramkumar Rathi and Rathi foundation for his support. We also acknowledge the kind cooperation of Kaveri group of education, Pune.