Journal of Pharmaceutical Care & Health Systems
Open Access
ISSN: 2376-0419
ISSN: 2376-0419
Research Article - (2016) Volume 3, Issue 2
Objective: Infections caused by multidrug resistant (MDR) Acinetobacter baumannii (ACB) are an increasing global problem. This review identifies and summarizes available research concerning resource utilization associated with MDR ACB, assesses strengths and weaknesses of the published research and identifies future research priorities. Methods: A structured review of the literature using MEDLINE enhanced by search of reference lists was conducted. Included articles reported on resource utilization or costs and described MDR ACB patients or compared cases to controls. Controls included patients with susceptible ACB, other organisms, or uninfected patients. Initial searches of the literature returned 204 potential citations for review. Title and abstract review excluded 171 articles, and full text review excluded 23 additional articles, leaving a total of 10 articles eligible for data abstraction and review. The full text of the 10 remaining articles was reviewed. Data on the characteristics of the studies and outcomes of interest were collected and organized into summary tables. All data were reviewed by a second reviewer. Results: Patients with MDR ACB had longer length of stay (LOS) than control groups across all studies, though findings were not always statistically significant. Within intensive care unit settings, LOS differences were significant in two of three studies. Hospital costs or charges were higher, sometimes significantly so, among patients with MDR ACB compared to controls. Conclusion: There was a consistent trend towards worse economic outcomes (longer LOS, higher costs) among patients with MDR ACB versus controls. Given the variety of study types and settings and the lack of multivariate analyses, there is considerable need for future studies.
Keywords: Cost and cost analysis; Cross infection; Catheter-related infections; Soft tissue infections; Respiratory tract infections; Acinetobacter baumannii
The growing prevalence of multi-drug resistant pathogens of the ESKAPE group presents a challenge to the healthcare system [1-3]. In particular, Acinetobacter baumannii (ACB), a gram-negative pathogen, has emerged as an important nosocomial pathogen with a prevalence of 12,000-46,000 cases annually in the USA and up to a million cases worldwide [4]. An estimate of direct healthcare costs associated with carbapenem-resistant ACB yielded an annual burden exceeding $389 million [4], however, the economic burden of multidrug resistant (MDR) ACB has yet to be quantified and is the objective of this structured literature review.
ACB’s shift from being present in healthcare settings to becoming a primary source of nosocomial infections has been facilitated by its ability to evolve and persist on environmental surfaces [5-7]. It commonly manifests as community- or hospital-acquired pneumonia, but can also cause urinary tract infection, bloodstream infection, and others [8]. Multiple risk factors for ACB have been identified, including intensive care unit (ICU) admission, surgery, catheter use, and ventilator use. The organism’s “success” [8] is demonstrated by increasing resistance to antibiotics such as carbapenems [9], frequency of outbreaks rather than individual cases [10], and national presence [11].
In addition to its existence in the acute care setting, ACB has been identified as a concern elsewhere. Several US military facilities have experienced ACB outbreaks [12], and it is a frequent concern among burn victims [13] and residents in long-term care facilities [14]. Recently, resistance to common antibiotics has been shown, requiring new paradigms for hygiene and treatment [15]. With few treatment options available, the increasing proportion of MDR strains worldwide is particularly alarming [16], including instances of pan-resistance [17].
Over the past decade, multiple small studies of ACB have been conducted. Reviews agree on the challenges of prevention, management of outbreaks, and difficulties with treatment [18-20], but empiric evidence on ACB, particularly MDR ACB, is sparse and significant knowledge gaps exist. Expectations that MDR ACB appears to be associated with an increased burden compared to other pathogens for patients and providers are expressed, but no structured review has quantified this burden.
To fill that gap, this review identifies, evaluates, and critiques the published data available related to resource utilization and economic burden associated with MDR ACB in the United States.
A PubMed search was conducted to identify articles specific to infections and ACB published from 10/27/2004 to 10/24/2014. Most terms were searched across “All Fields,” which automatically searches across multiple tags, including Medical Subject Heading (MeSH) terms, MeSH subheadings, pharmacologic action terms, and supplementary concept names, among others, and as a “Title/Abstract” word.
Also included are exclusions (indicated by “NOT”) and limiters (publication date, language, and humans). Individual terms were tested to ensure validity. The search strategy was implemented as follows:
(("costs and cost analysis"[All Fields] OR "economics, hospital"[ All Fields] OR "economics, medical"[ All Fields] OR "economics, nursing"[ All Fields]) OR "economics, pharmaceutical"[ All Fields] OR "fees and charges"[ All Fields] OR "health care sector"[ All Fields] OR “length of stay”[ All Fields]
OR
OR "cost*” [Title/Abstract] OR "economic*"[ Title/Abstract] OR "fees” [Title]Abstract] OR “charges"[ Title/Abstract] OR “length of stay” [ Title/Abstract])
AND
("cross infection"[All Fields] OR "infectious disease transmission, patient-to-professional"[All Fields] OR "infectious disease transmission, professional-to-patient"[All Fields] OR "catheter-related infections"[ All Fields] OR "urinary tract infections"[All Fields] OR "soft tissue infections"[ All Fields] OR "wound infection"[All Fields] OR "respiratory tract infections"[ All Fields] OR "skin diseases, infectious"[All Fields]
OR
"cross infection"[Title/Abstract] OR "catheter-related infections"[Title/Abstract] OR "urinary tract infections"[Title/Abstract] OR "soft tissue infections" [Title/Abstract] OR "wound infection"[Title/ Abstract] OR "respiratory tract infections"[Title/Abstract] OR "skin disease "[Title/Abstract])
AND
("anti-bacterial agents"[All Fields] OR "drug resistance, bacterial"[All Fields] OR "anti-bacterial agents"[Title/Abstract] OR " resistan*"[Title/Abstract])
NOT tb[All Fields]
NOT tuberculosis[All Fields]
NOT influenza[All Fields]
NOT tb[Title/Abstract]
NOT tuberculosis[Title/Abstract]
NOT influenza[Title/Abstract]
AND
("2004/10/27"[PDat] : "2014/10/24"[PDat] AND "humans"[MeSH Terms] AND English[lang]))
An initial review of article titles and abstracts was conducted. Exclusion criteria used to identify papers that did not qualify for fulltext review included: studies not including original or unique data, studies reporting no data on length of stay or costs studies not pertinent to infections, or studies conducted outside the United States.
Editorials, case studies, and reviews were excluded although reference lists were examined. Articles were not required to have been case-control studies; they could be descriptive, as well. Length of stay was included in the search strategy as a measure of resource utilization and as a proxy for differences in costs.
Papers were described by study and patient characteristics. When possible, studies were aggregated using a weighted average (by sample size) to provide a sense for the average and range of values, although studies were too heterogeneous to perform a formal meta-analysis.
Article selection and exclusion
A total of 204 articles were identified for title/abstract review. This set comprised 180 papers retrieved by the PubMed search and an additional 24 articles identified using alternate strategies (reference review, that is reviewing reference lists of articles identified in the abstract review; pearl finding, that is, using the “similar articles” feature in PubMed or typing article titles into an Internet search engine to identify related papers; allowing co-authors to suggest papers that they believe would be of interest that did not show up in the original PubMed search).
Manual title/abstract review excluded 171 articles, leaving 33 articles for full-text review. Full-text review excluded an additional 23 articles, leaving 10 articles eligible for abstraction [21-30]. Exclusion criteria used to identify papers that did not qualify for full-text review included: studies reporting no metric of resource utilization (no cost, length of stay, or other indication of units of resource utilization) across patient groups, studies not pertinent to healthcare-associated infections, or studies conducted outside the United States. There were three studies that quantified length of stay, but not in terms of whether the patients had MDR ACB; thus these studies were not included in the review [31-33].
Figure 1 details the process of article selection and exclusion at each stage of the review process and reasons for exclusion for the initial and full-text reviews. Some reasons appear in both exclusion lists as some articles required full-text review in order to determine inclusion/ exclusion when adherence to inclusion criteria was unclear from the abstract.
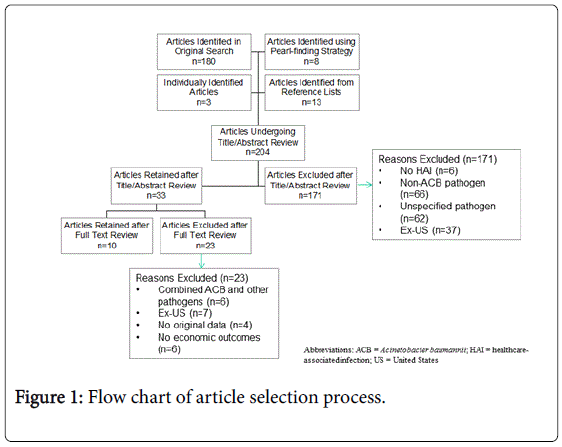
Figure 1: Flow chart of article selection process.
Study characteristics
Table 1 summarizes study characteristics. Among the 10 abstracted papers, studies were conducted in ICUs [23,24,27,30], burn centers or wards [29], and throughout hospitals [21,22,25,26,28] without specified wards. Seven studies [21-24,26,28-30] compared cases (defined in various ways) with controls.
| Citation | Study Design | Pathogen(s) and Infection Type(s) | Number/Type of Facilities and Location | Patient Characteristics |
|---|---|---|---|---|
| Brooklyn Antibiotic Task Force [21] | retrospective case-control study | S. aureus, K. pneumoniae, A. baumannii, P. aeruginosa. Any infection (among cases and matched controls: 60% RTI, 20% wound infection, 10% BSI, 10% UTI) | 7 hospitals reporting clinical data of 15 participating in study of pathogen isolates. NY (Brooklyn) | 77 total patients with ACB. 10 cases (of among 44) with carbapanem-resistant ACB (CRAB) were matched to 10 controls with carbapanem-sensitive ACB (CSAB) |
| Daniels et al. [23] | propensity-matched pairs analysis within retrospective cohort study | A. baumannii. Any infection (among cases and matched controls: 83% VAP, 14% BSI, 2% UTI) | 1 hospital, TN (Nashville) | 42 patients with MDR ACB matched with 42 patients with non-MDR ACB |
| Eberle et al. [24] | retrospective case-control study | A. baumannii, Any infection (among cases and controls, 81% HAP, 13% BSI, 6% UTI) | 2 ICUs, CA (Los Angeles) | 31 ACB patients matched to 62 controls with evidence of infection caused by other microorganisms |
| Esterly et al. [22] | retrospective case-control study | A. baumannii, BSI | 1 hospital, IL (Chicago) | 79 patients/cultures, 37 were carbapenem resistant ACB (CRAB), 42 were carbapenem nonresistant ACB (CNRAB) |
| Kollef et al.[25] | retrospective, observational cohort study | P. aeruginosa, Acinetobacter species and Stenotrophomonasmaltophilia, VAP | 1 hospital, MO (St. Louis) | Out of 76 total patients, 6 had ACB infections. Of these six, three survived 30 days. |
| Lautenbach et al. [26] | case-control study | A. baumannii, Any infection (distribution not reported) | 2 hospitals, PA (Philadelphia) | 69 case patients with imipenem-resistant ACB (IRAB) and 297 controls with imipenem-sensitive ACB (ISAB) |
| Lee et al. [27] | decision analytic model re A. baumannii in ICU | A. baumannii, Any infection | n/a, n/a | Simulated 1000 ICU patients. |
| Sunenshine et al. [28] | retrospective matched cohort | A. baumannii, BSI, pneumonia, surgical site, UTI, sterile site (other than blood), either healthcare-acquired or community-acquired | 2 hospitals, MD (Baltimore) | 96 MDR ACB case patients matched with two control groups: 91 patients with susceptible ACB infection and 89 uninfected hospitalized patients. |
| Wilson et al. [29] | case-control study | A. baumannii, Any infection, with 65% of patients having multiple infections (79% wounds, 59% RTI, 44% BSI, 12% UTI, 35% other) | 1 ICU burn unit, IN (Indianapolis) | 34 burn patients who acquired MDR ACB more than 48 hours after admission. Matched with 34 controls from patients treated in 1999 (before the emergence of MDR ACB at this institution). |
| Young et al. [30] | case-control study | A. baumannii, VAP, bacteremia, postoperative wound infections, central venous catheter-associated infections and UTI | 1 ICU, CO (Denver) | 67 patients with MDR ACB isolated during the study period. Matched with hospitalized control patients currently hospitalized |
Table 1: Summarizes study characteristics, among the 10 abstracted papers.
The included papers reflect remarkable geographic variability. Lee’s decision-analytic model [27] had national scope. The remaining 10 studies included at least two studies conducted in each of the regions identified by the United States Census Bureau [34] (West, Midwest, South, and Northeast). Each region is further divided into two or three divisions; only two (New England, West South Central) of the nine divisions were not represented.
Among the case-control studies, the specification of cases and controls varied greatly. Table 2 shows the variation in cases and controls and the number of patients in each cohort. In some cases, patients with resistant vs. susceptible strains of the same organism were compared while in others patients with MDR ACB were compared to patients with non-MDR ACB or to patients with other pathogens.
| Citation | Case Definition | Control Definition | LOS | ICU LOS | Costs/Charges |
|---|---|---|---|---|---|
| Brooklyn Antibiotic Task Force [21] | Carbapenem-resistant ACB (CRAB) (n=10) | Carbapenem-sensitive ACB (CSAB) (n=10) | 35 ± 21 vs. 16 ± 15 (mean), p=0.01, 31.5 vs. 13 (median), p=0.014 | NR | NR |
| Daniels et al. [23] | MDR ACB (n=42) | Non-MDR ACB (n=42) | 32.5 (IQR 22-51) vs. 26.5 (IQR 9-33) (median) | NR | NR |
| Eberle et al. [24] | ACB (n=31) | Patients with other pathogens (n=62) | 63 ± 58 vs. 40 ± 46 (mean), p=0.04 | 38 ± 34 vs. 25 ± 24, p=0.03 (mean) | NR |
| Esterly et al. [22] | CRAB (n=37) | CSAB (n=42) | NR | NR | NR |
| Kollef et al.[25] | Out of 76 total patients, 6 had ACB infections. Of these six, three survived 30 days. | Across all pathogens: 34.6 ± 23.4 (30-day survivors) vs. 19.9 ± 15.4 (30-day nonsurvivors), p=0.015 (mean), 32.8 ± 22.5 (appropriate initial antibiotic treatment) vs. 24.5 ± 21.9 (inappropriate initial antibiotic treatment), p=0.183 (mean) | Across all pathogens: 19.2 ± 18.5 (30-day survivors) vs. 15.7 ± 13.7 930-day nonsurvivors), NS (mean), 18.2 ± 16.3 (appropriate initial antibiotic treatment) vs. 19.0 ± 21.3 (inappropriate initial antibiotic treatment), p=0.881 (mean) | Mean total hospital costs, Across all pathogens: $86,644 vs. $68,597 (patients receiving an inappropriate initial antibiotic treatment vs. appropriate treatment), p= 0.390 | |
| Lautenbach et al. [26] | Imipenem-resistant ACB (IRAB) (n=69) | Imipenem-sensitive ACB (ISAB) (n=297) | Post-culture stay: 21 vs. 16, p=0.07 (median) | NR | Mean hospital charges after culture $334,516 vs. $276,059, p=0.03 |
| Lee et al. [27] | Decision analytic model | Assumed 25.23 ± 10.59 as input to model | NR | Hospital cost per ACB infection, Base case of model: $8,246 ± $4,472, National annual estimate of ACB in hospitals estimated at $7.4 to $26.1 million. | |
| Sunenshine et al. [28] | MDR ACB (n=96) | Control 1: Susceptible ACB infection (n=91), Control 2: Uninfected hospitalized patients (n=89) | 27.5 vs. 19.8 (Control 1), p=0.02 (mean), 27.5 vs. 18.6 (Control 2), p<0.01 (mean) | 13.3 vs. 6.7 (Control 1), p=0.04 (mean), 13.3 vs. 7.3 (Control 2), p<0.01 (mean) | NR |
| Wilson et al. [29] | Burn patients with MDR ACB (n=34) | Burn patients without MDR ACB (n=183) | 36.8 vs. 25.6, p<0.06 (mean) | NR | Mean total hospital costs, $201,558 vs. $102,983, p <0.01, Mean hospital cost per day, $5607 vs. $4017, p <0 .01 |
| Young et al. [30] | Cases: MDR ACB (n=67) Controls: uninfected patients (n=67) | 25.4 vs. 7.6, p<0.001 (mean), Multivariate analysis: MDR ACB contributed 13 days of hospitalization. | NR | Mean hospital charges, $306,877 vs. $135,986, p<0.001, Multivariate analysis: MDR ACB contributed $60,913 in incremental charges. | |
| ACB: Acinetobacter baumannii; BAL: Bronchoalveolar Lavage; BSI: Bloodstream Infection; ICU: Intensive Care Unit; MDR: Multidrug Resistant; NR: Not Reported; RTI: Respiratory Tract Infection; UTI: Urinary Tract Infection; VAP: Ventilator-Associated Pneumonia |
|||||
Table 2: Variation in cases and controls and the number of patients in each cohort.
Length of stay
Length of stay was reported in nine studies [21-26,28-30]. Table 2 presents length of stay for general ward and ICU. In case control studies, case patients had longer LOS than control groups in all studies, but the findings were not always statistically significant and the specific metrics varied. This trend was consistent within the ICU setting, and the difference between cases and controls was significant in two [24,28] of three [23] studies. Given the heterogeneity across studies a metaanalysis could not be conducted. Summarized across studies, the total hospital LOS was 1.51 times higher for cases than controls; when the analysis was weighted by the number of patients in each study, LOS was 1.53 times higher. This summary analysis excludes the study by Kollef et al. [25] that included patients with pathogens other than MDR ACB.
Three studies compared LOS among MDR ACB to uninfected controls. Young [30] reported a mean total LOS that was significantly longer for patients with MDR ACB compared to uninfected controls. Sunenshine et al. [28] found significantly longer mean total LOS among patients with MDR ACB compared to uninfected controls. Patterns for mean ICU LOS were similar, with significantly longer mean ICU LOS between MDR ACB-infected cases and susceptible ACB patients or between MDR ACB-infected cases and uninfected controls. Notably, the mean ICU stay was longer for the uninfected control group than for the susceptible ACB patients [28]. Wilson et al. [29] comparison of the mean total LOS for patients with MDR ACB vs. historical controls infected with other pathogens, identified from a period prior to MDR ACB emergence at the facility, found no significant difference.
The studies comparing carbapenem- or imipenem-resistant vs. susceptible strains also showed longer stays for patients with resistant strains compared to susceptible strains, although findings were not always significant. The Brooklyn study [21] found a significant difference in the mean total LOS for patients with CRAB vs. CSAB although the median was not significantly different. Esterly et al. [22] compared post-infection LOS for survivors with CRAB vs. CSAB and found a significant difference. Lautenbach et al. [26] reported that post-culture LOS was not significantly different between patients with imipenem-resistant ACB (IRAB) vs. imipenem-susceptible ACB (ISAB).
Patients with MDR ACB showed increased total and ICU LOS over patients with susceptible ACB, though not all findings were significant. Daniels et al. [23] did not find significant differences in the total LOS or the post-infection LOS. Sunenshine et al. [28] found significantly longer mean total LOS and mean ICU LOS when comparing patients with MDR vs. susceptible ACB.
Kollef et al. [25] compared LOS for 30-day survivors vs. nonsurvivors and patients treated with appropriate vs. inappropriate initial antibiotic therapies across a variety of infections. Thirty-day nonsurvivors had significantly shorter hospital LOS than non-survivors. Given the small number of MDR ACB patients in this study, the implications for MDR ACB are uncertain.
Eberle et al. [24] reported the median ICU LOS was longer for ACB cases whose susceptibility was not reported compared to controls infected with other organisms in a trauma ICU setting.
Four studies reported on hospital costs or charges [25,26,29,30] and one simulated them based on inputs from a literature review [27]. Details are presented in Table 2. Trends were consistent across three studies [26,29,30] indicating higher costs or charges associated with MDR ACB vs. controls (some findings were significant). Summarizing across these three studies, mean hospital costs (or charges) averaged 1.81 times higher for cases compared to controls; that ratio dropped to 1.27 times higher once the studies were weighted by the number of patients. This analysis summarized the relative expenditures for cases versus controls across studies without correcting for differences fiscal years or cost types included. It is expected that the ratio would be consistent despite these differences.
The fourth study Kollef et al. [25] did not compare MDR ACB vs. controls but rather compared patients who received appropriate vs. inappropriate initial treatment, and the simulation study [27] did not include a comparator.
Wilson et al. [29] found that total mean hospital costs in a burn facility were significantly greater for cases with MDR ACB vs. matched controls, and mean daily costs were also significantly higher for cases vs. controls. The costs were derived by multiplying detailed hospital bills by the cost to charge ratio (CCR) for the burn department. Costs were inflated to 2001 values using annual “medical inflation rates in the public sector” although exact details were not reported.
Young et al. [30] reported mean hospital charges were $306,877 for cases and $135,986 for controls (p<0.001). A multivariate model including patient and infection characteristics estimated that patients with MDR ACB infections had mean excess hospital charges of $60,913 compared to matched hospitalized control patients. Charges were collected from December 2004 through August 2005; they were not obviously adjusted or inflated. Only hospital charges were included.
Lautenbach et al. [26] found that mean hospital charges after culture were significantly higher for patients with IRAB vs. ISAB. This difference was no longer significant after adjusting for selected confounders (i.e., those that met pre-specified criteria for effect size, specifically IRAB infection, ICU at time of culture, transfer from another facility, and the number of hospital days prior to culture). The year of costing is not reported.
Kollef et al. [25] compared mean total hospitalization costs for ventilator-associated pneumonia (VAP) patients who received appropriate vs. inappropriate initial antibiotic treatment. There were no significant differences among patients who received initial inappropriate antibiotics vs. appropriate. It is believed that these values are means and standard deviations but it is not specified. The costs were derived by multiplying detailed hospital bills by the CCR for each relevant department. The year of costing is not reported.
A model created by Lee et al. [27] presents a framework for analysis of the cost of MDR ACB to a hospital. The report does not provide detailed source information, although the authors describe having conducted a literature review. In describing the inputs to the model, the authors indicate that their assumptions are based on limited information and should be considered carefully. Multiple scenarios are provided, assuming that 20-70% of patients colonized with ACB develop an infection. It is unclear whether type of infection was taken into account. Mean hospital costs per patient associated with ACB ranged from $8,246 to $49,608 (2010 US$), depending on the rate of infection and the number of days attributable to the infection. These costs are based on hospital cost per bed-day rather than cost per services provided. It is noted that this approach may underestimate costs although the authors speculate about the accuracy of including additional services for critically ill patients.
This structured literature review on resource utilization and costs of MDR ACB demonstrates trends across reviewed studies towards longer LOS and higher costs or charges among patients with MDR ACB compared to various types of control groups, and in several cases the findings were statistically significant. With the prevalence of MDR ACB in hospital settings increasing, these trends suggest a significant and likely growing economic burden associated with MDR ACB.
The search and article review processes for this study were consistent with best practices for systematic reviews, including detailing search terms and tracking article inclusion and exclusion based on a pre-defined checklist. However, as the review progressed, it became clear that the existing studies on the economic and resource burden of MDR ACB were insufficient to conduct a meta-analysis or statistically meaningful pooling of results. Our initial approach was to limit studies to a relatively recent time period and to the United States. While it is possible that extending back farther or including other countries or regions might have enlarged the pool of available studies and enabled such an analysis, the initial approach was deliberate and to extend these parameters without considering the impact they would have on the interpretation of findings would also be inappropriate. Thus, while the presentation of findings may be reminiscent of a descriptive review, the summary reflects a thoughtful aggregation of limited data identified by a structured and systematic search and review process.
This review identified limitations in both quantity and quality of existing studies. Only 10 relevant studies conducted in the United States were identified with some limitations regarding their applicability to MDR ACB. For example, some studies combined multiple infection types while others did not report on each pathogen separately. There is also evidence that facility characteristics may be relevant, even among acute-care hospitals [35]; the present analysis did not consider this factor. Another important limitation, variation in definitions of cases and controls, was raised by several authors in their own discussion sections [24,28,30] and clearly has even more importance when trying to synthesize findings across studies. Given the small numbers, we understand the interest in aggregating findings but each study could contribute more to the overall understanding of MDR ACB if reporting were detailed. The increased availability of online-only data supplements may facilitate presenting more information to interested readers. Because of the healthcare risk and significant and likely growing economic burden associated with MDR ACB, there is need for future studies to overcome these limitations and to gain confidence in and an accurate estimate of the magnitude of the impact of MDR ACB.
A number of improvements could be implemented for future studies. For example, study sizes should be adjusted to increase the likelihood of having sufficient statistical power to obtain significant findings. This may require collaborations across institutions. Data collection and reporting should be improved to allow for metaanalysis, with more complete reporting on subgroups and distributional metrics. Definitions of cases and controls should ideally be designed for broad applicability. Data on resource use should be presented in terms of units rather than costs to simplify comparisons across studies. Studies should be conducted both in- and outside the United States, accounting for differences by country. Follow-up that would capture re-admissions and long-term disability would also be useful to building a comprehensive economic estimate of the impact of MDR ACB.
In summary, this review demonstrates a significant and likely growing economic burden associated with MDR ACB, along with the need for additional studies to estimate this burden and understand its key drivers more accurately. Efforts and investments required to conduct such additional larger-scale studies of MDR ACB may be significant. However, these studies also bear a return of investment potential in terms of savings from gained insights that will offer options to control key drivers of the economic burden.
A grant was provided by The Medicines Company to Exponent for this research.