Cell & Developmental Biology
Open Access
ISSN: 2168-9296
ISSN: 2168-9296
Research Article - (2015) Volume 4, Issue 2
Background: HIV Mother-to-child transmission is the second most common mode of HIV transmission in sub-Saharan Africa which includes Ethiopia. However; there is little study on determinants of mother-to-child HIV transmission in the country.
Objective: To assess determinants of Mother-To-Child HIV Transmission.
Methods: A case-control study on infants who were born to HIV positive mothers was conducted in Assela, Adama and Bishoftu Hospitals. One hundred and six HIV infected (cases) and 318 not infected infants (controls) were selected by stratified random sampling method.
Results: Mothers who knew their HIV sero-positivity during pregnancy and after delivery were found significantly more likely to transmit HIV to their babies compared with those who knew before getting pregnant (AOR [95% CI] = 4.71 [ 1.39-15.93 ] and 4.46 [1.40-16.22]), respectively. Similarly, mothers who took Zidovudine prophylaxis for < 4 weeks and no Zidovudine prophylaxis at all during pregnancy were found significantly more likely to transmit (AOR [95% CI] = 13.29 [2.34-75.33] and 15.63 [3.29-74.26]), respectively. Likewise, Mothers with CD4 cell count < 200 and 201-500 cells/μl during lactation were found significantly more likely to transmit (AOR [95% CI] = 7.65 [3.20-18.31] and 4. 07 [1.90-8.71]), respectively. Mother who had cracked nipple/mastitis while lactating and who were practicing mixed feeding were also found significantly more likely to transmit (AOR [95% CI] = 13.05 [1.23-138.21] and 3.55 [1.62-7.78]), in that order. On the other hand, infants who were given Zidovudine for 28 days or 7 days after birth were found significantly less likely to contract HIV than single done Nevirapine given ones (AOR [95% CI] = 0.19 [0.07-0.48].
Conclusions: Knowing HIV sero-positivity before getting pregnant, longer duration of Zidovudine prophylaxis during pregnancy, extended prophylaxis to infant with Zidovudine, higher maternal CD4 cell count and healthy maternal breast while lactating and exclusive breastfeeding were found significantly protective of HIV mother-to-child transmission.
<Keywords: HIV; Transmission; Breast feeding
HIV Mother-to-child transmission (MTCT) is when an Human Immune deficiency Virus (HIV) positive woman passes the virus to her baby. This can occur during pregnancy, labour and delivery (at birth), or breastfeeding. Without treatment, around 15-30% of babies born to HIV positive women will become infected with HIV-1 during pregnancy and at birth. A further 5-20% will become infected through breastfeeding to 18-24 months. More than 50% of postnatal transmission through breast feeding to 18-24 months occurs during the first 6 months of life [1].
Globally, the number of children younger than 15 years living with HIV increased from 1.6 million in 2001 to 2.0 million in 2007. In sub-Saharan Africa alone, the epidemic has orphaned nearly 12 million children aged less than 18 years. In sub-Saharan Africa, more than 90 % of HIV infection in under 15 years age is acquired from the mother [2-4]. Women account for nearly 60% of HIV infections in sub-Saharan Africa [5].
In 2007, the estimated number of people living with HIV is 977,394 in Ehiopia, including 64,813 children [6]. Even though the exact prevalence of HIV in children is not known, there are currently 134,586 children under 14 years living with HIV/Acquired Immune Deficiency Syndrome (AIDS) in Ethiopia and 14,093 births to HIV positives in 2008. Without treatment, 75% of HIV infected children will die before their fifth birthday [7].
Today, developed countries have reduced the rate of transmission to babies to less than 1% by a combination of interventions, most importantly by antiretroviral therapy. However; in most African countries the rate remains above 10% [2, 5]. At the end of 2009, In Prevention of HIV Mother-To-Child Transmission (PMTCT) service providing sites in Ethiopia, 10,267 (2.4%) of the pregnant women following Antenatal Care (ANC) were tested positive. Of the total pregnant women diagnosed with HIV, only 6,466 (63%) received antiretroviral prophylaxis but, the overall country coverage is only 8% [8]. ANC coverage in 2008 was 59.4% and HIV prevalence among pregnant women was 3.9% [9].
Most studies agree that the risk of transmission is maximum during labor and delivery compared to during pregnancy or via breastfeeding [1,10]. However; they reported different on statistical significance of the factors associated with risk of mother-to-child HIV transmission and moreover there is hardly adequate studies conducted in Ethiopia yet in the field [10-14]. This study, therefore, will contribute to the intensively continuing study in the field to identify factors independently associated with HIV MTCT and will have an input for interventional planning.
Study settings
The study was conducted in three purposively selected hospitals of Oromia Regional State namely; Asella, Adama and Bishoftu hospitals. Assela referral hospital is located in Arsi zone whose capital is Assela town. Adama hospital is situated in Adama town of East-Showa zone and Bishoftu hospital is also in East-Shoa zone. Assela is located 75 kilometers to Southeast of Adama town which in turn is 100 kilometers to the East of Ethiopia’s capital-Addis Ababa and 55 kilometers from Bishoftu town in the same direction. According to the 2007 Ethiopian population and Housing census, Asella town has a population of 67, 250 whereas Adama and Bishoftu towns have a population of 222,035 and 100,114, respectively [6].
These three hospitals stood from first to third in delivering overall quality HIV/AIDS services and recognized by Oromia Regional Health Bureau and Colombia University-Ethiopia in the year 2009/2010 and all of them send Dried Blood Sample (DBS) of HIV exposed infants to Adama Regional Laboratory for Deoxyribonucleic acid (DNA) polymerase chain reaction (PCR) HIV test and receive the result within a month to confirm HIV infection.
Study design and period
An unmatched case-control study was conducted from March to June 2010 employing retrospective record review of results of DNA PCR HIV virology test determined during March 2007 to April 2010 for infants who had follow up in Assela, Adama and Bishoftu hospitals.
Sampling method
Stratified random sampling method was employed to identify study subjects from each of the three hospital strata proportionate to their study population size as it is detailed under sampling procedure ahead. (Figure 1)
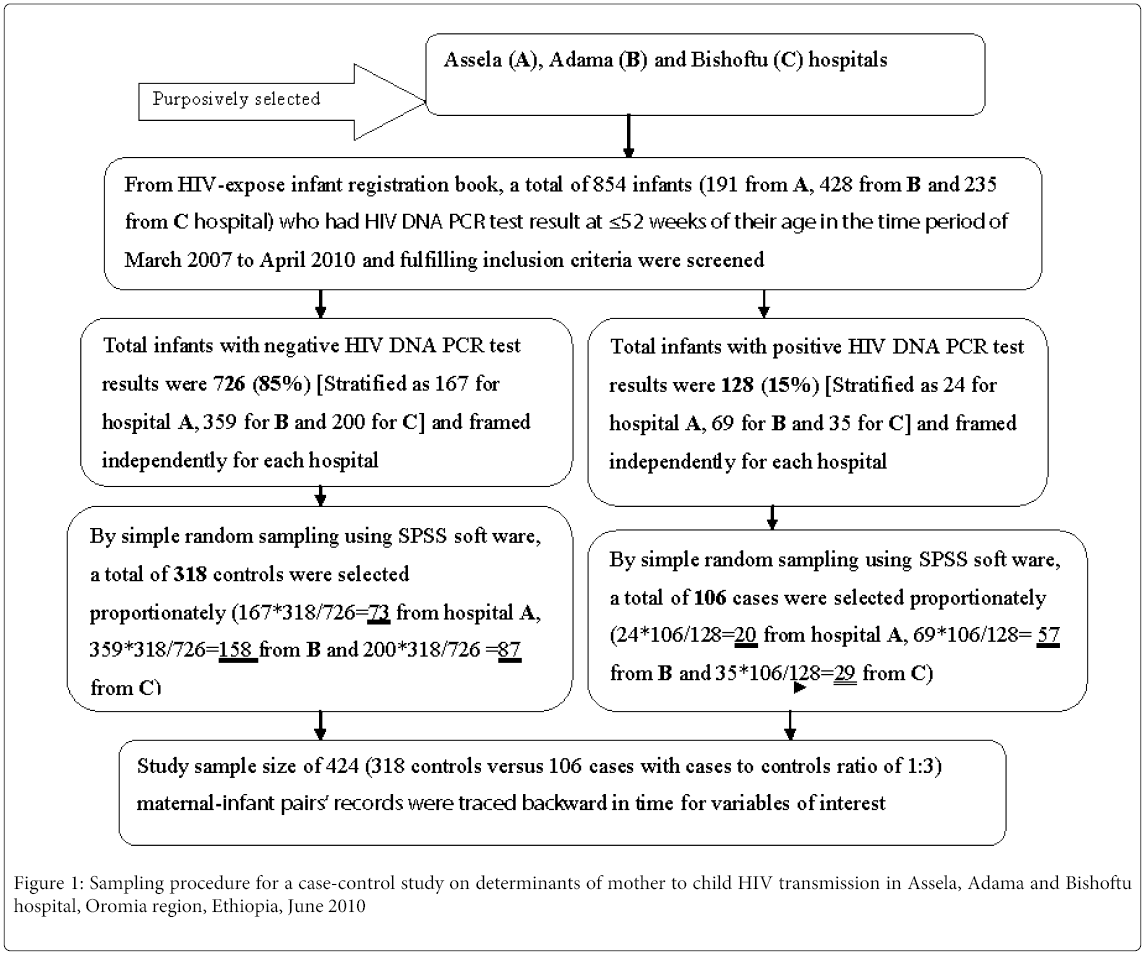
Figure 1: Sampling procedure for a case-control study on determinants of mother to child HIV transmission in Assela, Adama and Bishoftu hospital, Oromia region, Ethiopia, June 2010
Source population
All infants born to HIV positive mothers were the source population.
Study population
Infants born to HIV positive mothers and who have had DNA PCR HIV test result at ≤ 52 weeks of their age at Assela, Adama and Bishoftu hospitals were the study population.
Cases (HIV-infected infants)
Infants born to HIV positive mothers and found with at least one positive HIV DNA PCR test result at ≤52 weeks of age.
Controls (not HIV- infected infants)
Infants born to HIV positive mothers and found negative for HIV DNA PCR test at ≤52 weeks of age
Inclusion procedure
Singleton birth; Both maternal & infant’s record available in the hospital
Exclusion procedure
Orphaned/denied infants with no maternal record (i.e. those cared after by guardians were excluded)
Sample size determination
Using the methods of “difference between population proportions” with 80% power, 95% confidence interval, a ratio of cases to controls r being 1:3, odds ratio =3.05 and Percent exposure to “no ANC follow up” among infected group = 15.48% (from other study and which gave larger sample size), a sample size of 106 cases and 318 controls was calculated using Epi-info version 3.3.2, 2005; Sample size and power for unmatched case-control study.
A format that contains study variables of interest was prepared based on contents of health facility HIV/AIDS care records in touch of or directly addressing PMTCT and records of Anti-Retroviral Therapy (ART) to an infant or its mother. A nurse working in ART clinic (except a Health Officer used in Bishoftu hospital) and 2 data-clerks from each hospital were recruited and trained for 01 day on the format to be completed. Thereafter, data collectors reviewed sampled records of the infants and mothers and completed the format.
Operational definition of terms
Exclusive breastfeeding
Giving only breast milk during the first six months of infant’s age and no other drinks or food, not even water except syrup containing vitamins and minerals [4,15].
Mixed feeding
Giving breast milk with non-human milk and other fluids or solids [4, 15]
Exclusive replacement feeding
The use of breast milk substitute by totally avoiding breast milk [4, 15]
DNA PCR
Automated laboratory test that detects HIV-1 DNA in peripheral blood mononuclear cells. It is a qualitative test with sensitivity that approaches 96%-99% by 28 days of age. It is reliable in the presence of Anti-retro Viral (ARV) exposure for PMTCT or maternal ART [16].
DBS
Blood obtained from a heel or finger prick directly onto filter paper and dried at room temperature [16].
PCR
An automated process that enables researchers to produce millions of copies of a specific DNA sequence in approximately two hours [16].
Data processing and analysis
Data was entered using Epi-info version 3.3.2 and imported to SPSS version 15.0 for cleaning and analysis. Proportions between cases and controls were compared using cross tabulation. In the bivariate analyses, Odds Ratio (OR) with 95% confidence interval were computed for maternal socio-demographic, obstetric, immunological and clinical factors and infant factors in HIV-infected and non-infected infants to measure associations using binary logistic regression within Statistical Package for Social Sciences (SPSS) version 15.0. Variables that were significant at a P-value ≤ 0.10 in bivariate analyses were entered in to a multiple logistic regression model. In all the final multivariate models, any factor which does not include 1 in its 95% confidence interval of Adjusted Odds Ratio (AOR) was considered significantly associated.
Ethical clearance was obtained from Institutional Review Board of Medical faculty; Addis Ababa University by approval of the study proposal with protocol number of 100/09/SPH. A formal letter was obtained from Addis Ababa University, School of Public Health (SPH) and provided to Assela, Adama and Bishoftu Hospitals. Accordingly, permissions were obtained from the Hospitals’ higher officials to undergo the study. At each hospital, data were collected by HIV/AIDS care givers to whom parents of the infants already disclosed their HIV sero-positivity. Names of the study infants and their parents were avoided from the data collection format to assure confidentiality remained at data collector level (i.e. care givers). Hence there was no risk of confidentiality disclosure to be it the principal investigators or others who had potential access to a completed format.
From a total of 854 infants, 128 (15.0%) were HIV positive. From the above total, 424 infants were selected for this study. With controls to cases ratio of 3:1, 318 controls versus 106 cases were compared by the independent variables. The study infants were composed of 223 males (52.6%) and 201 (47.4%) females. The means ± standard deviations [Inter-quartile range] age of infants at time of HIV DNA PCR test had been done were 12.28 ± 10.23 [6-17] and 26.92 ± 17.50 [9-42.50] weeks for controls and cases, respectively. At 6 weeks age of their life, 186 (43.1%) infants were found had HIV DNA PCR test result determined. By 6 months (24 weeks) of age, DNA PCR test result of 277 (87.1%) controls versus 52 (49.1%) cases had been determined. Study infants’ mothers age group is from 25-34 years for 247 (58.3%) followed by 15-24 years of age for 137 (32.3%), and residences were urban for 285 (67.2%) and rural for 139 (32.8%). Concerning occupation, majority of the mothers, 249 (58.7%), were housewife followed by 67 (15.8%) daily laborers. Government or private sector employee makes 10.6% of the mothers. Regarding religion composition of the mothers, the majority (76.2%) were orthodox followed by Muslim which accounted for 13 %. Majority of the mothers, 331 (78.1%) were married and 47 (11.1%) mothers were divorced. By educational level, 144 (34%), 114 (26.9%), 100 (23.6%) and 59 (13.9%) of the mothers were with no schooling, grade 7-8, grade 9-12 and grade 1-6, respectively. Table 1 demonstrates the socio-demographic characteristics of infants and their mothers by cases and controls.
| Characteristics | HIV-ves (n=318) Frequency (%) |
HIV+ves (n=106) Frequency (%) |
Total (n=424) Frequency (%) |
| Sex of infants | |||
| Female | 154 (48.4) | 47 (44.3) | 201 (47.4) |
| Male | 164 (51.6) | 59 (55.7) | 223 (52.6) |
| Infants’ age when HIV DNA PCR test done (weeks) | |||
| 6 | 165 (51.9) | 21 (19.8) | 186 (43.9) |
| 7-12 | 58 (18.2) | 16 (15.1) | 74 (17.5) |
| 13-18 | 27 (8.5) | 7 (6.6) | 34 (8.0) |
| 19-24 | 27 (8.5) | 8 (7.3) | 35 (8.3) |
| ³ 25 | 41 (12.9) | 54 (50.9) | 95 (22.4) |
| Mean ± SD | 12.28 ± 10.23 | 26.92 ±17.48 | 15.94 ± 13.95 |
| Median | 6 | 25 | 8 |
| Interquartile range (IQR) | 6-17 | 9-42.50 | 8-23 |
| Mothers’ age group in years | |||
| 15-24 | 102 (32.1) | 35 (33.0) | 137 (32.3) |
| 25-34 | 189 (59.4) | 58 (54.7) | 247 (58.3) |
| 35-44 | 25 (7.9) | 12 (11.3) | 37 (8.7) |
| 45-50 | 2 (0.6) | 1 (0.9) | 3 (0.7) |
| Residence | |||
| Urban | 232 (73) | 53 (50.0) | 285 (67.2) |
| Rural | 86 (27) | 53 (50.0) | 139 (32.8) |
| Occupation | |||
| Housewife | 179 (56.3) | 70 (66) | 249 (58.7) |
| Employee | 32 (10.1) | 13 (12.2) | 45 (10.6) |
| Daily laborer | 56 (17.6) | 11 (10.4) | 67 (15.8) |
| Farmer | 21 (6.6) | 6 (5.7) | 27 (6.4) |
| Others | 30 (9.4) | 6 (5.7) | 36 (8.5) |
| Religion | |||
| Orthodox | 241(75.8) | 82 (77.4) | 323 (76.2) |
| Muslim | 40 (12.6) | 15 (14.2) | 55 (13.0) |
| Protestant | 35 (11.0) | 9 (8.5) | 44 (10.4) |
| Other | 2 (0.6) | 0 (0) | 2 (0.4) |
| Marital status | |||
| Married | 248 (78.0) | 83 (78.3) | 331 (78.1) |
| Single/unmarried | 8 (2.5) | 2 (1.9) | 10 (2.4) |
| Widowed | 25 (7.9) | 11 (10.4) | 47 (11.1) |
| Divorced | 37 (11.6) | 10 (9.4) | 36 (8.5) |
| Educational level | |||
| College/University | 5 (1.6) | 2 (1.9) | 7 (1.7) |
| Grade 9-12 | 88 (27.7) | 12 (11.3) | 100 (23.6) |
| Grade 7-8 | 86 (27.0) | 28 (26.4) | 114 (26.9) |
| Grade 1-6 | 43 (13.5) | 16 (15.1) | 59 (13.9) |
| No schooling | 96 (30.2) | 48 (45.3) | 144 (34.0) |
Table 1: HIV-infected mothers’ and their infants’ socio-demographic characteristics by cases and controls in Assela, Adama and Bishoftu Hospitals, Oromia Region, June 2010. HIV-ves = HIV negative infants (controls), HIV+ves = HIV positive infants (cases).
Though mothers’ educational level lower than grade 9-12 and residence in the rural were associated with HIV MTCT in the bivariate analysis, only grade 1-6 mothers’ educational level was significantly associated in multivariate analysis (AOR [95% CI] = 4.49 [1.21-16.71]). Other socio-demographic characteristics such as maternal age, occupation, marital status and religion were not significantly associated in the bivariate analysis (P-value > 0.10) and hence not included in the multivariate analysis as displayed in table2.
| Variable | Cases (n=106) | Controls (n=318) |
COR [95% CI] | P-value | AOR [95% CI] |
| Age group <30 |
73 | 232 | 1.00 | ||
| ≥30 | 33 | 86 | 1.22 [0.76-1.97] | 0.42 | NI |
| Educational level | |||||
| Grade 9-12 | 12 | 88 | 1.00 | 1.00¥ | |
| Grade 7-8 | 28 | 86 | 2.39 [1.14-5.00] | 0.02 | 1.69 [0.60-4.78] |
| Grade 1-6 | 16 | 43 | 2.73 [1.19-6.27] | 0.02 | 4.49 [1.21-16.71] |
| College/University | 2 | 5 | 2.93 [0.51-16.8] | 0.23 | NI |
| No schooling | 48 | 96 | 3.67 [1.83-7.35] | <0.001 | 1.68 [0.58-4.82] |
| Occupation | |||||
| Housewife | 70 | 179 | 1.00 | 1.00¥ | |
| Employee | 13 | 32 | 1.99 [0.99-4.02] | 0.10 | 0.92 [0.41-2.10] |
| Trader | 5 | 27 | 2.07 [0.83-5.15] | 0.12 | NI |
| Student | 1 | 3 | 0.94 [0.30-2.99] | 0.92 | NI |
| Farmer | 6 | 21 | 1.70 [0.16-17.86] | 0.66 | NI |
| Daily labor | 11 | 56 | 1.45 [0.48-4.43] | 0.51 | NI |
| Residence | |||||
| Urban | 53 | 232 | 1.00 | 1.00¥ | |
| Rural | 53 | 86 | 2.70 [1.71-4.25] | <0.001 | 1.44 [0.73-2.88] |
| Marital status | |||||
| Married | 83 | 248 | 1.00 | ||
| Single/unmarried | 2 | 8 | 0.75 [0.16-3.59] | 0.72 | NI |
| Widowed | 11 | 25 | 0.81 [0.39-1.70] | 0.57 | NI |
| Divorced | 10 | 37 | 1.32 [0.62-2.79] | 0.48 | NI |
| Religion | |||||
| Orthodox | 82 | 241 | 1.00 | ||
| Muslim | 15 | 40 | 1.1 [0.58-2.10] | 0.77 | NI |
| Protestant | 9 | 35 | 0.76 [0.35-1.64] | 0.48 | NI |
| Other | 0 | 2 | 0.16 [0.00-2.2E+06] | 0.67 | NI |
Table 2: association of maternal socio- demographic characteristics with HIV MTCT by bivariate and multivariate analyses in Assela, Adama and Bishoftu hospitals, Oromia region, Ethiopia, June 2010. COR= crude odds ratio, CI= confidence interval, AOR= adjusted odds ratio, NI= Not included in multivariate, ¥ =adjusted for residence, time mother learnt HIV sero-positivity, Zidovudine during pregnancy for PMTCT, in labour ARV drug, infant ARV prophylaxis and breast feeding option.
Maternal ARV and obstetric factors associated with HIV MTCT
After adjusting for possible confounders, mothers who didn’t use Zidovudine (AZT) prophylaxis during pregnancy for PMTCT were found about 15 times significantly more likely to transmit HIV to their babies than those mothers who took AZT for four or more weeks before birth (AOR [95% CI] = 15.63 [3.29-74.26]) . Similarly, mothers who used AZT for less than four weeks before birth were about 13 times significantly more likely to transmit the virus to their babies (AOR [95% CI] = 13.29 [2.34-75.33]). In relation to type of ARV prophylaxis taken during labour, mothers who took single dose Nevirapine (sdNVP) and those who didn’t use any prophylaxis were 4.42 and 7.52 times more likely to transmit HIV to their babies compared with three drugs combination prophylaxis users [i.e. AZT + Lamivudine (3TC) + sdNVP] in the bivariate analysis (COR [95% CI] = 4.42 [1.71-11.39] and 7.52 [3.70-15.26]), respectively. However; types of ARV prophylaxis interventions during labour didn’t retain its statistically significant difference in preventing HIV MTCT after controlling for other factors. Times of learning sero-positivity in relation with pregnancy by the mothers were also assessed. Accordingly, mothers who learn their sero-positivity during pregnancy and after delivery were more than 4 times significantly more likely to transmit HIV to their babies than those mothers who learnt their sero-positivity before getting pregnant (AOR [95% CI] = 4.71 [1.39-15.93] and 4.76 (1.40-16.22]), respectively. Nevertheless; knowing sero-positivity during labour failed to show statistically significant association with HIV MTCT in both bivariate and multivariate analysis. Mothers who didn’t attend ANC follow up were found 4.42 times more likely to transmit the virus to their babies (AOR [95% CI] = 4.42 [2.76-7.08] in the bivariate analysis. Likewise, mothers who had lesser number of ANC visits such as three times, twice and only once were significantly more likely to transmit HIV to their babies compared with those mothers who had more than four visits (COR [95% CI] = 8.30 [2.11-32.72], 15.56 [3.79-63.87] and17.29 [3.47-86.05]), respectively even though four times ANC visits showed no significant difference compared with more than four times visit. Concerning duration of ART taken by the mothers while pregnant, mothers who were treated for less than four weeks before birth were more than 6 times more likely to transmit HIV to their babies compared to those treated for four or more weeks (COR [95%] = 6.75 [1.10-41.44]). Places of delivery were also assessed and it was found that mothers who gave birth at home were 3.32 times [95% CI for COR = 2.07-5.32] more likely to transmit HIV to their babies than those who gave birth at hospital.
On the other hand, presence or absence of ANC follow up, numbers of ANC visits, duration of ART taken during pregnancy and type of delivery institution failed to show statistically significant difference in affecting HIV MTCT in the multivariate analysis as demonstrated in table3.
| Variables | Cases (n=106) |
Controls (n=318) |
COR [95% CI] | P-value | AOR [95% CI] |
| Pregnancy AZT | N=94 | N=179 | |||
| AZT for ≥ 4 weeks | 2 | 58 | 1.00 | 1.00† | |
| AZT for < 4 weeks | 7 | 20 | 10.15 [1.95-52.93] | 0.006 | 13.29 [2.34-75.33] |
| None | 85 | 101 | 24.41 [5.79-102.88] | <0.001 | 15.63 [3.29-74.26] |
| ARV during labour | N=94 | N=179 | |||
| AZT+3TC+sdNVP | 11 | 85 | 1.00 | 1.00† | |
| SdNVP only | 12 | 21 | 4.42 [1.71-11.39] | 0.002 | 0.86 [0.18-4.14] |
| None | 71 | 73 | 7.52 [3.70-15.26] | <0.001 | 0.66 [0.12-3.67] |
| Learn sero-positivity | |||||
| Before pregnancy | 8 | 159 | 1.00 | 1.00† | |
| During pregnancy | 41 | 96 | 8.49 [3.82-18.87] | <0.001 | 4.71 [1.39-15.93] |
| At labour | 2 | 9 | 4.42 [0.82-23.91] | 0.085 | 1.78 [0.19-16.82] |
| After delivery | 55 | 54 | 20.24 [9.07-45.20] | <0.001 | 4.76 [1.40-16.22] |
| ANC history | |||||
| Yes | 34 | 215 | 1.00 | 1.00 β | |
| No | 72 | 103 | 4.42 [2.76-7.08] | <0.001 | 0.72 [0.34-1.54] |
| ANC visits | N=34 | N=215 | |||
| >4 times | 3 | 83 | 1.00 | 1.00 β | |
| 4 times | 8 | 78 | 2.84 [0.73-11.08] | 0.13 | NI |
| 3 times | 9 | 30 | 8.30 [2.11-32.72] | 0.002 | 2.70 [0.34-21.39] |
| 2 times | 9 | 16 | 15.56 [3.79-63.87] | <0.001 | 5.30 [0.63-44.70] |
| Once | 5 | 8 | 17.29 [3.47-86.05] | <0.001 | 1.80 [0.17-19.40] |
| Pregnancy ART | N=12 | N=139 | |||
| ≥ 4 weeks | 10 | 135 | 1.00 | 1.00 α | |
| < 4 weeks | 2 | 4 | 6.75 [1.10-41.44] | 0.039 | 6.02 [0.85-42.39] |
| Delivery place | |||||
| Hospital | 37 | 198 | 1.00 | 1.00 α | |
| Health Center/clinic | 7 | 20 | 1.87 [0.74-4.74] | 0.19 | NI |
| Home | 62 | 100 | 3.32 [2.07-5.32] | <0.001 | 2.98 [0.81-10.95] |
Table 3: Maternal ARV drug and other interventions’ association with HIV MTCT in Assela, Adama and Bishoftu hospitals, Oromia region, Ethiopia, June 2010. †adjusted for residence, educational level, time mother learn sero-positivity, pregnancy AZT, in labour ARV prophylaxis, infant ARV prophylaxis, breast feeding and computed excluding those on ART, β=adjusted for pregnancy AZT & infant ARV, α=adjusted for pregnancy ART, delivery place, infant ARV and age at enrolment.
This study had also assessed association of HIV MTCT with mothers’ clinical conditions, which are put as clinical stage I through IV by World Health Organization based on presence or absence of different opportunistic infections in HIV infected individuals, and mothers’ immunity conditions. As a result no significant difference detected amongst maternal Third Trimester (TTM) clinical stages, TTM CD4 levels and postnatal clinical stages in affecting HIV MTCT. However; mothers with lower postnatal CD4 were more likely to transmit HIV, i.e. mothers who had postnatal CD4 cells/µl < 200 were 7.65 times [95% CI for the AOR = 3.20-18.31] more likely to transmit the virus than those mothers who had CD4 > 500 cells/µl. likewise, mothers who had CD4 of 201-500 cells/µl were assessed 4.07 times [95% CI for the AOR = 1.90-8.71] more likely to transmit HIV. Mothers’ immunological condition assessed other than CD4 cell count was the breast condition. Accordingly, mothers who had cracked nipple or mastitis while lactating were also significantly more likely to transmit HIV to their infants (AOR [95% CI =13.05 [1.23-138.21]) as presented in Table 4.
| Variables | Cases (n=106) | Controls (n=318) | COR [95% CI] | P-value | AOR [95% CI] |
| TTM clinical stage | N=39 | N=236 | |||
| Stage I | 17 | 82 | 1.00 | ||
| Stage II | 10 | 59 | 0.82 [0.35-1.92] | 0.64 | NI |
| Stage III | 12 | 85 | 0.68 [0.31-1.51] | 0.35 | NI |
| Stage IV | 0 | 10 | - | - | - |
| TTM CD4 cell count/µl | N=37 | N=231 | |||
| >500 | 5 | 65 | 1.00 | 1.00 µ | |
| 201-500 | 23 | 127 | 2.35 [0.86-6.48] | 0.10 | 2.21 [0.33-14.83] |
| ≤200 | 9 | 39 | 3.00 [0.94-9.60] | 0.06 | 1.73 [0.51-5.88] |
| Postnatal clinical stage | N=92 | N=276 | |||
| Stage I | 35 | 107 | 1.00 | ||
| Stage II | 24 | 62 | 1.18 [0.65-2.17] | 0.59 | NI |
| Stage III | 28 | 94 | 0.91 [0.52-1.61] | 0.75 | NI |
| Stage IV | 5 | 13 | 1.18 [0.39-3.53] | 0.77 | NI |
| Postnatal CD4 cell/ µl | N=92 | N=276 | |||
| >500 | 9 | 94 | 1.00 | 1.00£ | |
| 201-500 | 59 | 148 | 4.16 [1.97-8.79] | <.001 | 4.07 [1.90-8.71] |
| ≤200 | 24 | 34 | 7.37 [3.12-17.43] | <.001 | 7.65 [3.20-18.31] |
| Breast condition | N=92 | N=276 | |||
| Normal | 88 | 275 | 1.00 | 1.00£ | |
| Cracked/Mastitis | 4 | 1 | 12.50 [1.38-113] | 0.025 | 13.05 [1.23-138.21] |
Table 4: Maternal clinical and immunological factors associated with HIV MTCT in Assela, Adama and Bishoftu hospitals, Oromia region, Ethiopia, June 2010. μ= controlled for ANC follow up, AZT drug during pregnancy for PMTCT , £= controlled for infant oral lesion, breast lesion during lactation/post natal maternal CD4 cell count and only computed for breast feeding infants. TTM = third trimester pregnancy (from 28 weeks of gestation onwards).
From infant related factors, sex and age at enrolment to follow up clinic were not significantly associated with HIV MTCT though infants’ age of > 8 weeks at enrolment was associated in the bivariate analysis (COR [95% CI] = 5.28 [3.19-8.72]). Regarding types of ARV prophylaxis given to infants after birth, infants those provided no ARV prophylaxis and provided sdNVP only were about 7 times and 5 times significantly more likely to contract HIV from their mothers than to those infants provided with sdNVP + AZT for 7 or 28 days (AOR [95% CI] = 7.57 [2.84-20.22] and 5.35 [2.08-13.79]), in the same order. Looking at infant feeding option, infants on mixed feeding (MF) were 3.55 times [95% CI for AOR = 1.62-7.78] more likely to contract HIV from their mothers than infants on exclusive breast feeding (EBF) but that didn’t hold true for infants on exclusive replacement feeding (ERF) and for those shifted from EBF to ERF. Infants’ oral lesion didn’t retain its statistical significance in the final multivariate analysis as showed in Table 5.
| Variable | Cases (n=106) | Controls (n=318) | P-value | COR [95% CI] | AOR [95% CI] |
| Sex | |||||
| Female | 47 | 154 | 1.00 | ||
| Male | 59 | 164 | 0.47 | 1.18 [0.76-1.83] | NI |
| Age at enrolment | |||||
| ≤08 weeks | 25 | 197 | 1.00 | 1.00™ | |
| >08 weeks | 81 | 121 | <0.001 | 5.28 [3.19-8.72] | 1.45 [0.37-5.65] |
| Infant ARV prophylaxis | |||||
| sdNVP+AZT 7/28 | 13 | 168 | 1.00 | 1.00@ | |
| SdNVP only | 17 | 47 | <0.001 | 4.67 [2.12-10.31] | 5.35 [2.08-13.79] |
| None | 76 | 103 | <0.001 | 9.53 [5.04-18.03] | 7.57 [2.84-20.22] |
| First 6 month’s feeding | |||||
| EBF | 55 | 249 | 1.00 | 1.00¶ | |
| ERF | 14 | 42 | 0.23 | 1.51 [0.77-2.95] | NI |
| MF | 33 | 21 | <0.001 | 7.11 [3.83-13.23] | 3.55 [1.62-7.78] |
| from EBF to ERF | 4 | 6 | 0.095 | 3.02 [0.82-11.06] | 2.55 [0.46-14.06] |
| Oral lesion | N=92 | N=276 | |||
| No | 9 | 11 | 1.00 | 1.00# | |
| Yes | 83 | 265 | 0.04 | 2.61 [1.05-6.52] | 2.06 [0.75-5.65] |
Table 5: Infant factors associated with HIV MTCT in Assela, Adama and Bishoftu hospitals, Oromia region, Ethiopia, June 2010.™controlled for maternal ART during pregnancy and delivery place, @ controlled for residence, maternal educational level, delivery place and breast feeding option, ¶ controlled for residence, maternal educational level, time mother learnt sero-positivity, AZT during pregnancy for PMTCT, in labour ARV prophylaxis and infant ARV prophylaxis, # controlled for postnatal maternal CD4 cell count and breast lesion during lactation, AZT 7/28= AZT for 7 days or 28 days to infant after birth based on duration of AZT used by the mother.
This study analyzed maternal socio-demographic, maternal ARV and obstetric interventions, maternal clinical and immunological and infant factors potentially associated with HIV Mother-to-child Transmission during pregnancy, at labour and delivery and postnatally via breast feeding.
Maternal age of at least 30 years at delivery period was not significantly associated with HIV MTCT. This is consistent with the findings of cohort studies in Newyork and South Africa [17, 18].
Maternal educational level of grade 1-6 was significantly and positively associated with HIV MTCT though the reason remained unclear to the scope of this study.
Maternal religion and occupation type were not significantly associated with HIV MTCT and there are similar reports from United Kingdom and Ireland [19].
Intake of AZT for four or more weeks before birth by the mother was significantly protective of HIV MTCT. This is in agreement with the study by TanarakPlipat in Thailand which had stratified the duration of AZT given to the pregnant before birth. But it is in contrast to the cohort study by Sheldon H. Landesman on comparable sample size (525) which showed that AZT during pregnancy was not significantly protective of HIV MTCT. The likely explanation for the difference between the cohort study and this study could be that the cohort study didn’t stratify the duration of AZT given during pregnancy and compared only grossly as no AZT versus AZT given groups. On the other hand, a study in Abidjan-Cote d’Ivoire showed the difference of AZT drug during pregnancy for more than 20 days versus for maximum of 20 days remained below statistical significance unlike this study which compared ARV duration for more than 4 weeks versus less than 4 weeks. This difference may be due to compared durations of AZT during pregnancy in this study were wider than that of Cote d’ivoire study to detect the difference AZT intervention could bring in preventing HIV MTCT [11, 17, 20].
There was no significant difference showed between less than four weeks maternal ART and four or more weeks ART duration during pregnancy in reducing HIV MTCT. As revealed by a study in Unite Kingdom and Ireland, ART at conception was associated with a lower risk of HIV MTCT than ART started in pregnancy (0.1% versus 1%; P=0.001), but this was only of borderline significance after adjusting for mode of delivery, sex and maternal plasma viral load (AOR, 0.18; 95% CI, 0.02-1.33) which could be due to residual in-utero transmission before initiation of ART and this study has no different explanation [19].
There was no significant difference between giving no ARV, sdNVP and AZT+3TC+sdNVP during labour to the mother for PMTCT. However; because this study didn’t assessed the timing of in labour ARV drug administration in relation with child expulsion time (recommended to be 2 hours before child expulsion), it cannot judge that in labour ARV has no protective value. A clinical trial study by Shapiro in Botswana indicated that there is no difference between sdNVP and AZT to the mother during pregnancy in protecting the infant from HIV transmission in the early life. Though comparing the different ARV for PMTCT directly is difficult, another study in Cote d’Ivoire showed that adding 3TC to AZT + sdNVP had no adding value in reducing HIV MTCT and using AZT alone as reference of HIV transmission at 6 weeks, the protective effect of two-drug combination (AZT+ sdNVP) was strong enough for PMTCT [11, 20].
Knowing HIV sero-positivity by the mother before pregnancy was associated with reduced HIV MTCT in this study than knowing during pregnancy or after delivery and is in contrast to that of Thailand study. The possible reason for the difference could be, in Thai’s study, 24.2% of the infants in birth cohort had incomplete follow-up or inconclusive HIV status outcome, and it appears that those without outcomes (knew sero-positivity during pregnancy and after delivery) may had had a higher transmission risk due to poor adherence to heath care services for PMTCT [11].
Both history of ANC follow-up and number of ANC visit were not associated with HIV MTCT. This result is consistent with the cross-sectional study in South Africa by Mark C, with the study in Thailand and Malawi. However pregnant women who had ANC follow-up history were more likely to use ARV drugs for PMTCT during pregnancy [11, 21, 22].
In this study, delivery places didn’t reach significance level in their association with HIV MTCT. However; sero-positive mothers who delivered at hospital or health center level were more likely to take intra-partum ARV drug for PMTCT (53.2% for hospital delivery and 31.6% for health center, excluding those on ART) and to give ARV drug to their infants during postnatal (85.9% for hospital and 70.3% health center deliveries) than those mothers who delivered at home (only 14.8% received intra-partum ARV drug and 9.7% of infants received ARV prophylaxis). Lack of association between delivery place and HIV MTCT in this study is in agreement with the study of Landesman, Plipat, Mwapasa and Coovadia [17, 11, 19, 22].
Regarding third trimester clinical stage, studies in the United Kingdom and Ireland showed maternal WHO clinical stages were not associated with HIV MTCT. Nevertheless, in this study the odds for clinical stage II and III were lesser (0.82 and 0.68, respectively) than stage I (asymptomatic stage). This can be explained either by maternal viral load is higher during early stage of HIV infection and thus increasing HIV MTCT or because stage II and III are symptomatic mothers would be insisted by their illness to seek health care and thereby more likely to get ARV treatment [4, 15, 19].
Maternal third trimester CD4 cell count per micro-liter didn’t show statistically significant association with HIV MTCT. This result is in agreement with Botswana’s, Malawi’s and study in Thailand but is against that of Cote d’Ivoire’s. One cohort study reported that there could be discordant virological and immunological responses in individuals on ARV drugs. Accordingly, CD4 T-lymphocyte raised in certain individuals despite high plasma HIV-1 RNA levels. Alternatively, CD4 T-lymphocyte numbers failed to rise in other individuals despite undetectable plasma HIV RNA [20, 22-25].
Unlike that of third trimester, postnatal maternal CD4 cell count during breast feeding that was measured within 6 months following birth was significantly associated with increased HIV MTCT when less than 500 cells/µl. Equivalently, the study in South Africa indicated infants exclusively breastfed by women with CD4-cell counts < 200 per µl were significantly twice as likely to become infected and almost 4 times more likely to die before 6 months of age than were infants exclusively breastfed by women with CD4-cell count above 500 per µl after adjusting on the viral load. The study in Cote d’Ivoire also reported significant association between HIV MTCT and postnatal maternal CD4 cell count less than 500 per µl. The possible explanation for the difference between third trimester and postnatal CD4 in association with HIV MTCT could be, those who were infected in-utero and miscarried by mothers with lower CD4-cell counts could fallaciously cause the lack of association by because they were not included and diluting the number of actually infected offspring in low CD4 cell count mothers which otherwise could be higher [2, 18, 20].
Maternal breast lesion while lactating was significantly associated with greater HIV MTCT. The observation of an association between maternal breast lesions and HIV MTCT is consistent with the study in Malawi [22].
Delivering prolonged ARV prophylaxis (AZT in this study) to the infant for seven days or 28 days, based on maternal ART or AZT intake duration, during postnatal period was significantly protective from HIV MTCT. Inconsistent to this finding, a randomized controlled trial in Malawi by Taha reported mother to child transmission at 6 to 8 weeks was not significantly different for infants who received sdNVP regimen versus infants received sdNVP with extended AZT for one week. However, the study group didn’t conceal that the AZT regimen was administered for one week and with the exception of the first dose, all the doses were administered at home by the mother, and adherence reports might not have been accurate though self reported was as high as 90% which was so in this study too. However; there was residual difference in HIV transmission at birth between the compared groups [8.1% in infants receiving only sdNVP and 10.1% in those receiving AZT plus sdNVP) which might affect the association at 6-8 weeks of infants age [13].
Mixed feeding was seen significantly and positively associated with HIV MTCT. A study in South Africa revealed, infants with mixed feeding were 11 times more likely to be infected with HIV than exclusively breastfeeding group. Similar to this study, in studies in Malawi, Thailand and Cote d’Ivoire, no significant difference was observed between exclusive replacement and exclusive breast feeding with regard to HIV MTCT at 6 weeks of life [11, 20, 22].
Knowing HIV sero-positivity before getting pregnant, longer duration of AZT prophylaxis during pregnancy, extended prophylaxis to infant with AZT, higher maternal CD4 cell count and healthy maternal breast while lactating and exclusive breastfeeding were found significantly protective of HIV mother-to-child transmission.
Knowing HIV sero-status prior to getting pregnant need to be part of intended pregnancy parameters in the country’s health policy.Sero-positive pregnant women should be reached with AZT prophylaxis, if not eligible for ART, earlier than four weeks before birth to substantially reduce HIV MTCT.Increasing maternal CD4 cell count using ARV drugs and educating the mother on preventing or getting treatment early for any breast lesion while lactating are also paramount importance in helping HIV infected mothers grow up HIV free child. Finally, this study recommends to the government of Ethiopia to consider and pay commitment in increasing maternity leave from the currently three months to six months, postnatally, for mothers who are employee to inspire them feed their infants exclusively with breast milk till six months of infants’ age though it seems resource intensive to put into action.
As this is a case control study mainly based on record review for data collection some variables like duration of membrane breakage and maternal sexually transmitted infections (for instance syphilis) were not included in the study.
The authors are indebted to Addis Ababa University, School of Public Health, for its financial support to undertake this study. We are also thankful to data collectors.