Journal of Medical Diagnostic Methods
Open Access
ISSN: 2168-9784
ISSN: 2168-9784
Review Article - (2015) Volume 4, Issue 4
Infections remain the most common immediate causes of morbidity in immune compromised hosts. The abated host defences are responsible for an increased susceptibility to various uncommon and opportunistic pathogens, and to a lowered host inflammatory response. Skin lesions develop in up to a third of infections in these patients, and they possibly represent the initial step of a systemic illness. Superficial mycoses are occasionally present under unusual atypical presentations. The resulting clinical infections are at times difficult to diagnose. Some of them are recalcitrant to common conventional therapies. The broad scope of cutaneous manifestations of infections in compromised patients are classified based on four presumed underlying physio-pathologic mechanisms, and on the vast array of potential pathogens so far identified. For mild superficial infections, prompt adequate therapy decreases morbidity and lessens the risk of complications. For more severe involvement, early detection of opportunistic fungal infections helps increasing both the cure and survival rates.
Keywords: Mycosis; Dermatophytosis; Immune defense; Cyanoacrylate skin surface stripping
The immunocompromised hosts include patients with primary or congenital immune deficiency diseases, such as severe combined immunodeficiency, thymic aplasia or diverse immunoglobulin deficiencies, common variable immunodeficiency, patients under chemotherapy, organ transplant recipients, splenectomised patients, as well as various autoimmune diseases under steroid or cytotoxic therapy. The prevalence of dermatophytoses is unfrequently increased in patients with AIDS or suffering from malnutrition, diabetes mellitus, alcoholism, peripheral vascular disorders, neurotrophic ulcers and severe burns.
The number of immunocompromised individuals at risk for fungal infections is steadily growing in the global population. The immunocompromised condition depends on a diversity of biological defects [1,2]. Mycotic infections remain common morbidities in the compromised host, and the clinical presentations are usually atypical. The diagnosis is sometimes difficult to establish by clinicians. The abated host defences fuel an increased susceptibility to a number of uncommon and opportunistic pathogens, and to failing of the host inflammatory responses. Nonvirulent skin fungi are usually ubiquitous in the environment and, at times, they intermittently colonize and cause local and superficial skin infections. Opportunistic microorganisms rarely cause disease in immune competent hosts. In some instances, the lesions represent an immediate cause of death.
The occurrence and development of any given mycotic infection depends on specific interactions between the incoming microorganism and the host response. The clinical manifestations result from the aggressiveness of the microorganism and the response of the underlying defence status of the host (Figure 1). With compromised host defences, patients are at increased risk of skin infections with a wide variety of less virulent microorganisms. This is the crux of the problem of infections in immunocompromised patients. The adhesion of microorganisms to the stratum corneum (SC) [3,4], and its barrier system represent additive components of the skin protection.
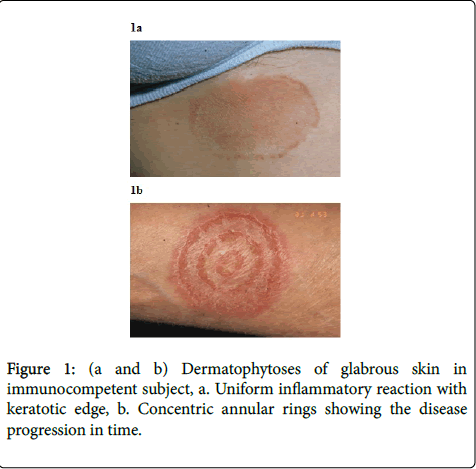
Figure 1: (a and b) Dermatophytoses of glabrous skin in immunocompetent subject, a. Uniform inflammatory reaction with keratotic edge, b. Concentric annular rings showing the disease progression in time.
CSSS diagnostic method
One of the most convenient ways to collect and examine the infected superficial skin layers is the cyanocrylate skin surface stripping (CSSS), formerly named skin surface biopsy [5-10]. In its most widely appreciated context, the SC exerts a major barrier function against microorganisms, ultraviolet radiations, oxidants, and a variety of other toxic xenobiotics. In addition, the SC protects from loss of water and biologically important electrolytes from the body. The SC structure is highly specialized and under constant renewal controlling a steady state in its composition and thickness [11].
CSSS is initiated by depositing a drop of cyanoacrylate adhesive onto a supple transparent sheet of polyethylene, 175 μm thick, cut to the size of a conventional coverslip (1.5 x 6 cm). The material (3S-Biokit, CK Technology, Visé, Belgium) is pressed firmly on the target lesion [9,10]. After 15-30 s, an unbroken sheet of SC is usually conveniently harvested. As the adhesion mechanism of cyanoacrylate results from a chemical hardening, the thickness of the removed SC relies on the depth of penetration of the adhesive before polymerisation. The cleavage level of the CSSS sampling is exclusively restricted inside the SC. The sampling procedure is bloodless and often painless. The cost is minimal. The following laboratory procedure is quite simple and not time-consuming.
CSSS are conveniently collected from any part of the body, with three main provisos. First, oozing and eroded lesions are not adequately studied using CSSS due to the lack of adhesion. Second, CSSS samplings from a hairy area turns out to be painful following pulling out hairs. In addition, the CSSS quality is then poor owing to the erratic contact with the SC. Thus, it is advisable to shave such areas before CSSS sampling. Third, the intercorneocyte cohesion on the palms and soles [11] is commonly stronger than the cyanoacrylate bond, thus impairing the collection of an unbroken sheet of corneocytes. Anyhow, CSSS samplings from these sites are possible in some physiopathological conditions associated with a compromised texture and cohesion of the SC [9].
Dermatomycoses in the immune compromised patient
Dermatophytoses in the immunocompromised host are probably best classified according to the presumed immunopathological mechanism and the nature of the infectious intruder microorganism. Four categories of skin clinical manifestations are distinguished, namely: (a) infections originating in the skin with common microorganisms that tend to spread more than in normal hosts; (b) extensive skin involvement with microorganisms that usually cause restricted infection in a normal patient, but leads to more severe involvement in the immunocompromised host; (c) infection with opportunistic microorganisms responsible for a primary skin infection with local or systemic dissemination and (d) cutaneous dissemination of the fungus caused by a systemic disease elsewhere in the body.
Dermatophyte infections are common in some otherwise healthy patients, but more prevalent in immunocompromised hosts. The most common of these are individuals with lymphopenia showing up to 20% in prevalence when T-cell counts are less than 400 cells/mm. The groin, trunk, feet, and hands are frequently involved, whereas infection of the face and scalp is less common.
Common nonvirulent agents are ubiquitous in the environment, and they intermittently contaminate and colorize the skin leading to superficial infections in normal hosts. They correspond to dermatophytes (Trichophyton spp, Microsporum spp, Epiderphyton spp) and a few nondermatophyte molds (Fusarium spp, Alternaria spp, Aspergillus spp). These fungi are adapted to the nonliving cornified cells of the SC, hair and nails. Some observations suggested an increased frequency of fungal colonization in immunocompromised patients at sites usually free of the microorganisms in normal hosts. Dermatophytosis is a contagious disease resulting from the direct or indirect transfer of arthroconidia, hyphae or cornified cell debris containing such microorganisms from a primary habitat or an an infected host to the uninfected susceptible recipient. Dermatophytes typically remain viable in cornified cells and fomites for long periods. Some infections are caused by a wide array of opportunistic microorganisms, in particular fungi, including Histoplasma, Blastomyces, Aspergillus, Paecilomyces, Candida, Mucor and other phycomyces.
Dermatophytes are in part classified based on their origin. Anthropophilic dermatophytes are derived from humans, zoophilic dermatophytes originate from animals, and geophilic dermatophytes are rooted in the soil. Anthropophilic dermatophytes cause relatively noninflammatory clinical presentations, whereas geophilic and zoophilic fungal infections are frequently more acute and highly inflammatory. Dissemination of dermatophytes depends on direct or indirect contacts between infected and uninfected hosts. The first step in the infection process corresponds to colonisation of the cornified layers of the SC [3,4]. Fungal cells representing the contagious and infectious propagules correspond to arthroconidia and hyphal fragments adhering to, or contained within some corneocytes. The initial contact between arthroconidia and corneocytes is a crucial event in the initiation and establishment of the skin infection. The adherence of fungi to host cells is mediated through fungal adhesins and their interactions with host receptors. The relatively large size of dermatophytes in the cornified tissue, provides a rapid diagnostic clue under microscopic examination. Microscopy provides the definitive diagnosis of a dermatophyte infection, even in absence of growth in culture.
The sensitivity of microscopy is enhanced using a variety of dyes, or a fluorescent brightener such as Calcofluor white or Blankophor BA. The fungal penetration of the SC starts with the emergence of germ tubes from the arthroconidia. Hyphae penetrate both parallel to and perpendicular through the thickness of the SC. By about 7 days of incubation, hyphae form arthroconidia, thereby completing the vegetative growth cycle of the fungus.
Both geographic and ecologic differences are present in the various dermatophyte species. Dermatophytoses of glabrous skin begin as erythematous papules progressing to scaling-forming sharply circumscribed raised erythematous edges. In otherwise normal individuals, several target-like erythematous rings are occasionally present (Figure 1). The appearance of infection in the immunocompromised patient is often not substantially different from that present in healthy individuals. However, the immunocompromised host, dermatophytoses tend to be more extensive, more numerous and with defective inflammatory response with undistinaguished scaling margins. Similarly, patients who have applied topical corticosteroids to dermatophyte lesions develop a modified presentation of ringworm sometimes known as tinea incognito [12].
CSSS in dermatomycoses
Straightforward diagnoses are commonly established using CSSS in superficial, infectious skin diseases [9,10]. Microscopy provides a basic but rapid test for the diagnosis of a dermatophyte infection, the fungi showing distinctive morphological forms of hyphae and arthroconidia, and their relatively large size. Fungi, including yeasts and dermatophytes, form clusters or a network of globular and filamentous structures [7-10,13-15]. The aspect is typically altered by antifungal treatments (Figure 2a-2d). This method is an important aid to diagnosis. Morphological examination of CSSS, possibly combined with fungal cultures, is conveniently carried out to identify these dermatoses. Infectious agents embedded in cyanoacrylate on top of the skin surface on CSSS are not visible on such sampling [9]. Only, those invading the SC are readily identified.
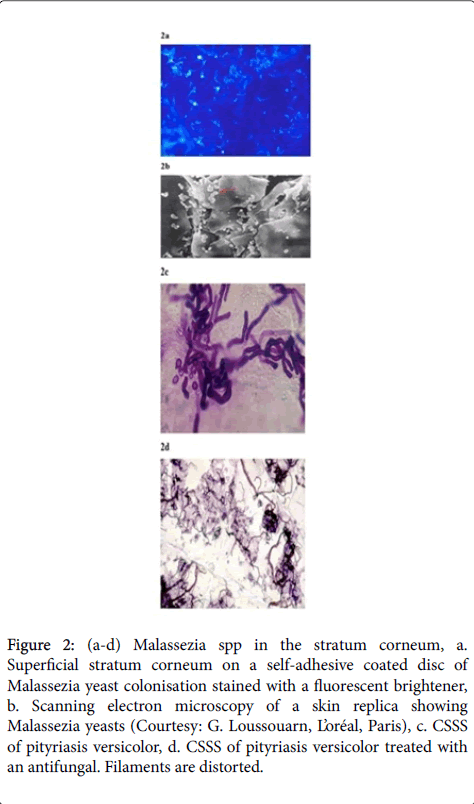
Figure 2: (a-d) Malassezia spp in the stratum corneum, a. Superficial stratum corneum on a self-adhesive coated disc of Malassezia yeast colonisation stained with a fluorescent brightener, b. Scanning electron microscopy of a skin replica showing Malassezia yeasts (Courtesy: G. Loussouarn, L’oréal, Paris), c. CSSS of pityriasis versicolor, d. CSSS of pityriasis versicolor treated with an antifungal. Filaments are distorted.
Definite diagnoses are reached in superficial dermatophytoses using CSSS. In immunocompetent patients, the dermatophyte hyphae are usually dispersed without any clumps. Serous deposits are frequently abundant in association with parakeratotic cells (Figure 3a and 3b). By contrast, in immunocompromised patients, the network of hyphae is commonly dense and focally compact (Figure 4a-4e), showing, aspects reminiscent of radial thigmotropism [16]. Serous deposits are typically absent. In such instances, fungal cells are frequently observed beyond the limits of the clinical lesion.
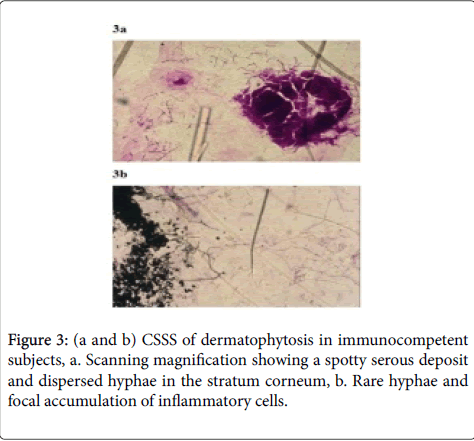
Figure 3: (a and b) CSSS of dermatophytosis in immunocompetent subjects, a. Scanning magnification showing a spotty serous deposit and dispersed hyphae in the stratum corneum, b. Rare hyphae and focal accumulation of inflammatory cells.
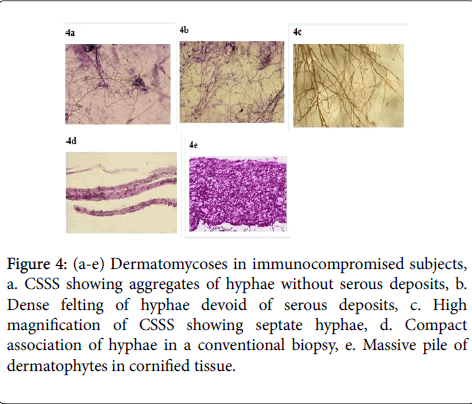
Figure 4: (a-e) Dermatomycoses in immunocompromised subjects, a. CSSS showing aggregates of hyphae without serous deposits, b. Dense felting of hyphae devoid of serous deposits, c. High magnification of CSSS showing septate hyphae, d. Compact association of hyphae in a conventional biopsy, e. Massive pile of dermatophytes in cornified tissue.
Corneofungimetry analytical bioassay
The relationships between dermatophytes and the human SC are complex and recognized for a long time. Dermatophytes are a group of fungi that share the ability to invade and digest keratin as saprophytes in vitro. Most species also grow as parasites in the SC, causing clinically distinct lesions. The fungal morphology in the parasitic growth phase is different from the morphology exhibited in their in vitro saprophytic phase (Figure 5a-5d).
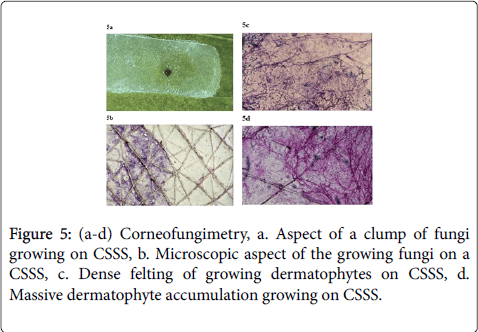
Figure 5: (a-d) Corneofungimetry, a. Aspect of a clump of fungi growing on CSSS, b. Microscopic aspect of the growing fungi on a CSSS, c. Dense felting of growing dermatophytes on CSSS, d. Massive dermatophyte accumulation growing on CSSS.
Fungal cells of superficial dermatophytoses are readily visible on CSSS. In the corneofungimetry procedure, a number of fungi are possibly cultured on corneocytes, particularly CSSS. In experimental settings, some analytical assessments of disease severity and therapeutic activity on dermatophytoses are possibly performed on CSSS using computerized image analysis of the corneofungimetry bioassay [17-21]. Beyond conventional antifungigrams [22] quantifications of the restricted fungal extent following antifungals are conveniently performed in experimental dermatomycosis [10,17,23]. Oral or topical antifungals are initially administered to healthy volunteers for a defined restricted period of time (usually a couple of days) before CSSS samplings. A controlled amount of arthroconidia collected from primary cultures is deposited onto the CSSS supposedly impregnated by the antifungal drug under consideration. After a given period of time (about 10 days) of dermatophyte culture on corneocytes in a clean environment, the CSSS are stained for revealing growing fungi. Computerized image analysis is used to fine-tune the quantification of the mycelium growing on CSSS. The comparison with control untreated CSSS allows to derive the percentage of inhibition of the fungal growth induced by the antifungal under evaluation. Image analysis of corneofungimetry allows the analytical evaluation of the test and allows comparisons in the growth progression of specific fungal species, and on the fungal growth inhibition exerted by tested antifungals [17,20].
During the early phases of corneofungimetry following arthroconidia adhesion to corneocytes, a radial spread of hyphae is observed, irrespective of the nature of the dermatophyte. In the next stage, the orientation becomes commonly more erratic. Growing hyphae are crossing over each other. The radial thigmotropism is therefore lost when apparently the hyphal density reaches some density. The length of the fungal hyphae could represent another reason for the failure of the radial thigmotropism of the fungal colony. We never saw formation of microconidia on CSSS, and macroconidia similar to in vitro fungal cultures.
Corneofungimetry has some advantages over conventional in vitro anti fungigrams that are clearly influenced by both the culture medium composition and the physiological state of the microorganism [23]: (a) the treatment is applied in vivo in conditions normally encountered by patients, (b) the initial fungal load is possibly controlled, (c) the growth substrate is only composed of corneocytes without any additional compounds, and (d) any influence of corneocytes including natural antimicrobial peptides and Toll-like receptors is respected. An appropriate choice of treatment is helped by this procedure, and should reduce some inappropriate therapeutic decisions [24].
Corneofungimetry is little or not influenced by the immunocompromised status of the patient because the bioassay is performed on the SC alone outside the influence of inflammatory cells. Thus, this method somewhat represents an ex-vivo model of the early dermatophyte invasion of the SC similar to the condition of the immunocompromised host.
Clinicians should be keenly aware of any unusual skin lesion as possible early sign of dermatomycosis in immunocompromised host. Many of these diseases are exogenous in origin, caused by pathogenic fungi which are capable of invading tissue irrespective of the underlying condition of the hosts. The infectious propagule of a dermatophyte is a modified vegetative hyphal cell, the arthroconidia. The first phase of invasion of the skin is adherence of the arthroconidia to the SC, a time-dependent process which is followed by germination and penetration of the SC by the fungal germ tube. A prompt search for diagnosis should be initiated, possibly using CSSS. The risk of extension and dissemination increases when waiting for further clues to identify the disease process at a later stage.
The ultimate cause of a dermatophyte infection in immunocompromised hosts is contact with an infective inoculum which is of two different origins: in some cases the infective propagules originate from sources from where they are transmitted directly or indirectly, or, usually, the infective inoculum originates from infected material, skin, scales, or hairs, from which the propagules are transmitted directly or indirectly.
Biometrology applied to CSSS represents an important analytical tool showing much sensitivity in detecting superficial dermatomycoses, particularly when clinical observation alone is not conclusive. This is particularly the case in immunocompromised patients. Corneofungimetry provides comparative information with regard to the intrinsic growth of fungal species on SC alone, and about the efficacy of antifungals in the relationship between the fungi and the SC.