Journal of Tumor Research
Open Access
ISSN: 2684-1258
ISSN: 2684-1258
Case Report - (2018) Volume 4, Issue 1
Dermatofibrosarcoma protuberans (DFSP) is a rarely observed tumor of a subcutaneous tissue. Its incidence is about 0.8-4.5/1000000. Fibrosarcomatous transformation of DFSP has been described in the literature, accounting for about 10% of DFSP cases. A high-grade sarcoma with fusiform and pleomorphic cells is a very rarely observed tumor. It is mainly located on proximal extremities and body; it is seldomly seen in the breast. The tumor grows gradually within the years. The local recurrence is frequently observed, however, the metastasis is rarely present. It is treated by a resection with free surgical margins. We presented Forty-three years old multipar patient a case of DFSP with a high-grade sarcoma, a histologic feature with spindle and pleomorphic cells in the breast. Up to date, on no cases with such a tumor in the breast has not been reported yet.
Keywords: Dermatofibrosarcoma, Breast, High-grade sarcoma
Dermatofibrosarcoma protuberans (DFSP) is a rarely observed tumor of a subcutaneous tissue. It was firstly defined by Darier and Ferrand [1] as nodular cutaneous tumor composed of fusiform cells with a storiform growth pattern in 1924. The name of DFSP was given by Hofmann [2]. Its incidence is about 0.8-4.5/1000000 [3,4]. It is mostly detected in young and middle-aged adults (between the ages of 20-50); however, the cases may be reported in any ages. It does not demonstrate a hereditary nature.
It is mainly located on proximal extremities and body; it is seldomly seen in the breast [3,4]. The tumor grows gradually within the years. The local recurrence is frequently observed, however, the metastasis is rarely present [5,6]. It is treated by a resection with free surgical margins. DFSP is relatively resistant to chemotherapy and radiotherapy [7]. Fibrosarcomatous transformation of DFSP has been described in the literature, accounting for about 10% of DFSP cases [8]. A high-grade sarcoma with fusiform and pleomorphic cells is a very rarely observed tumor. We presented a case of DFSP with a high-grade sarcoma, a histologic feature with spindle and pleomorphic cells in the breast. Up to date, on no cases with such a tumor in the breast has not been reported yet.
Forty three years old patient with a multipar was referred to our clinic with a complaint of a mass in the right breast that growed within the last six months. Any remarkable feature was not identified in her history. At the examination, she had a mobile mass with a size of nearly 10 cm, in the right upper outer quadrant of the breast, which was firm and had clearly distinguishable lobulated margins from breast tissue. At the right axilla, there was no clinically detectable lymph node. At mammography examination, there was high opacity nodules with smooth margin in a size as 3.5 cm for the bigger one and as 2.5 cm for the smaller one, which were presented as super-positioned with each other were detected in the right upper outer quadrant of the breast.
At the ultrasound examination, the solid nodule formations sized as 3.5 × 2.5 cm for the bigger one and 2.5 × 1.5 cm for smaller one with smooth margins and hypoechoic quality were identified at nearly 7 mm depth inside from the skin of the right upper outer quadrant of the breast. A histopathological examination with a pre-diagnosis of phyllodes tumor was recommended. A core needle biopsy was performed. At histopathological examination of core needle biopsy was reported as a mesenchymal tumor. The total excision of the mass was recommended, considering phyllodes tumor as a first diagnosis along with the current findings.
A tumorectomy was performed with free surgical margins (nearest margin is 1 mm), closed with intraglandular flap technique. The size of the tumor was 10 × 5 × 5 cm. The postoperative pathology of the patient was evaluated as malign mesenchymal tumor at our center. The case was referred to another pathology department which is more experienced about the soft tissue sarcoma. In the microscopic examination, the tumoral lesions were observed within the breast tissue, which had infiltrative margins and multinodular formation (Figure 1A). While the tumor with a heterogeneous appearance sometimes composed of spindle cells that gathered together in a storiform pattern, it demonstrated any noticeable atypical signs (Figures 1B and 1C), it somewhere consisted of pleomorphic components, which spread randomly in myxoid stroma and more cellular components, which undergone mitosis frequently (Figures 1D and 1E). At immunohistochemical examinations, a CD34 expression was detected in the spindle cell component of the lesion with a storiform pattern, while the CD34 staining was not identified in the other component (Figures 2A-2C). On the other hand, while Ki-67 proliferation index was nearly 40% in the cellular component of tumor, which was composed of pleomorphic cells, it was found to be decreased up to 10% in the other component (Figures 3A-3C). ERG, CD31, SMA, desmin, S100, caldesmon, myogenin and AE1/AE3 staining were found as negative. Along with these findings, the case was diagnosed as a high-grade sarcoma with spindle and pleomorphic cells at the base of dermatofibrosarcoma protuberans.
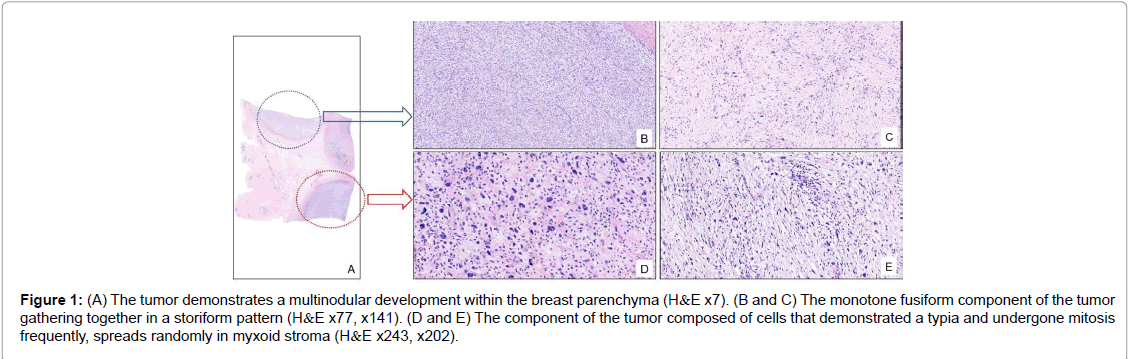
Figure 1:(A) The immunohystochemical heterogenous CD34 staining in the tumor (x13). (B) The CD34 positivity in the component of tumor with fusiform cells demonstrating storiform pattern (x97). (C) The loss of CD34 expressions in the component of the tumor presenting certain atypia and undergoing mitosis frequently (x242).
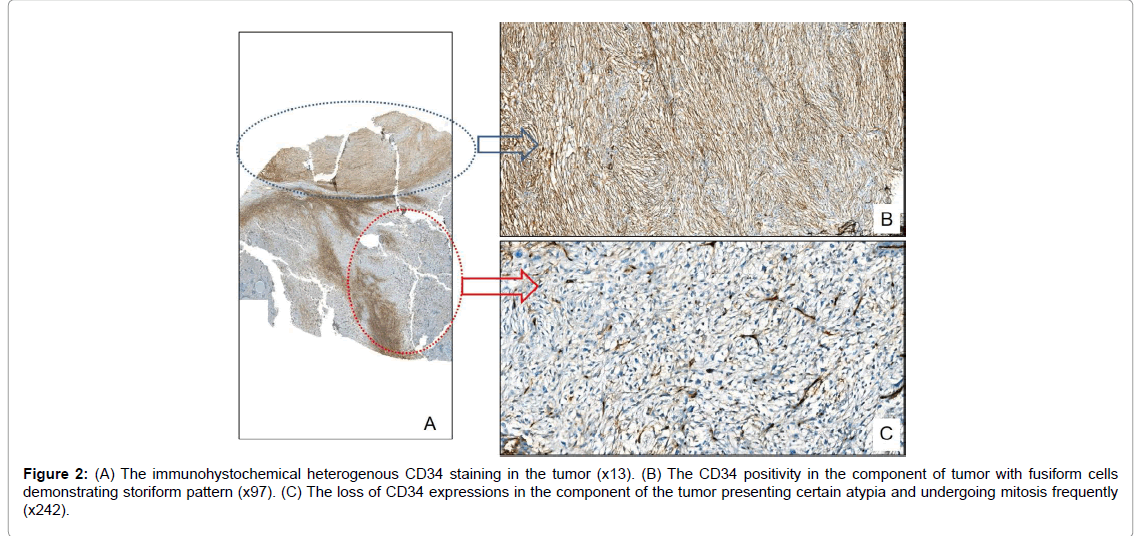
Figure 2:(A) The immunohystochemical heterogenous CD34 staining in the tumor (x13). (B) The CD34 positivity in the component of tumor with fusiform cells demonstrating storiform pattern (x97). (C) The loss of CD34 expressions in the component of the tumor presenting certain atypia and undergoing mitosis frequently (x242).
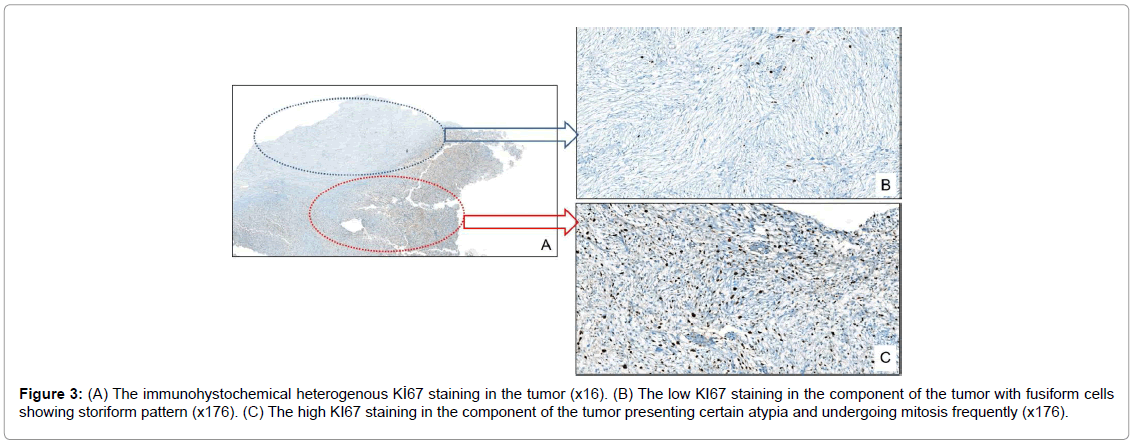
Figure 3:(A) The immunohystochemical heterogenous KI67 staining in the tumor (x16). (B) The low KI67 staining in the component of the tumor with fusiform cells showing storiform pattern (x176). (C) The high KI67 staining in the component of the tumor presenting certain atypia and undergoing mitosis frequently (x176).
The systemic screenings were completed and any signs of metastasis were not detected. The simple mastectomy was decided to be performed due to closed surgical margin. In the postoperative pathology findings, any residue tumor was not detected. Along with this finding, the patients had 5000 rad radiotherapy with 25 divided doses.
DFSP is a locally aggressive tumor of the dermis. While it constitutes 0.1% of malign neoplasm, it comprised of about 1% of soft tissue sarcomas. It emerges as a small-sized nodule with a redbrown color. By the time, it gradually develops and transforms into a multinodular and firm mass, in which bleeding areas and ulcerations may be observed [9]. DFSP is a rarely seen tumor on the breast tissue. DFSP is a seldomly-detected tumor in the breast. As our knowledge, the case with a high-grade sarcoma with pleomorphic cells at the base of DFSP in the breast is the first case in the literature.
Our case was atypical presentation which has not skin involvement even though reach large size. It presented as phyloides tumor with a lobulated margin at examination. At histologic examination, it is easily confused with phylloides tumors unexperienced pathologist about the soft tissue sarcoma.
Since there was no knowledge in the literature about the DFSP with pleomorphic sarcomatous differentiation in the breast, we treated the patients as high grade soft tissue sarcoma.
In a recent systematic review, clinical outcome of DFSP and DFSP with fibrosarcomatous features were compared resulting in a significant difference in risk of local recurrence (13.7 vs. 29.8%), risk of metastasis (1.1 vs. 14.4%) and death from disease (0.8 vs. 14.7%) [10].
A wide local excision was recommended for the surgical treatment of DFSP; however, there is no agreement on the width of the surgical margins. In the guideline of NCCN, a surgical margin of 2-4 cm and excision of the depth fascia of the tissue are recommended for DFSP [11]. In our case, a simple mastectomy was performed due to the proximity of microscopic surgical margin, after an extended local excision and inappropriateness of re-excision by a second surgery. According to the genetic studies, more than 90% of patients had a translocation between chromosome 17 and chromosome 22 [12,13]. As a result of this translocation, an excessive oscillation occurred at plateletderived growth factor receptor B (PDGFRB) [10,11]. Consequently, an imatinib msylate, which is also a protein kinase inhibitor, may be used for unresectable and locally recurrent tumors and in the treatment of DFSP [14]. The radiotherapy should be added to the treatment plan in order to decrease relapse rates in DFSP with high-grade sarcomatous differentiation, as occurred in our case [15-17]. Our patient has high probability of a relapse rate as high due to tumor size of 10 cm, the existence of pleomorphic sarcomatous changes and having a value of 40% for Ki 67 proliferation index.
The breast is an atypical location for the placement of DFSP and it may presents with an atypical clinic picture. The transformation of pleomorphic sarcomatous at the base of DFSP may be seldomly occurs. The occurrence of a high-grade sarcoma with spindle and pleomorphic cells at the base of dermatofibrosarcoma protuberans should be taken into consideration and an extended surgical resection should be performed. These lesions should be treated like sarcomas.