Journal of Medical Diagnostic Methods
Open Access
ISSN: 2168-9784
ISSN: 2168-9784
Research Article - (2016) Volume 5, Issue 3
A descriptive study was conducted with the aim to evaluate the dental patients’ knowledge about the consequences of smoking on health and to explore the patient’s approach towards the role of dentists in smoking cessation. Study population consisted of patients visiting Dental OPD of tertiary care facility, Karachi in the month of November 2015 using a questionnaire. Findings revealed that patients had adequate level of knowledge about the association of smoking and lung cancer (86.5%), heart disease (74%) and oral cancer (71.5%). Patients had affirmative approach towards the role of dentists and revealed willingness to quit smoking if recommended by the dentist. Hence, dentists should involve actively in smoking cessation and grab this chance to improve the health of community.
Keywords: Knowledge; Dentists’ role; Prevention; Smoking cessation
The tobacco epidemic represents a leading public health challenge. In the 20th century, tobacco has been accountable for 100 million deaths globally. It is expected to be liable for a staggering one billion casualties in the 21st century unless urgent action is taken. The data underline the enormity of the challenge that has an effect on all countries [1]. Pakistan has the peak burning up of tobacco in South Asia spending Rs. 250 billion in the fiscal year FY14. The State Bank’s Statistical Bulletin reports that Pakistanis smoked 64.48 bn cigarettes in the year FY-14. Pakistan Demographic Health Survey revealed that 46 % men and 5.7 % women smoke tobacco [2].
Tobacco utilization is the major preventable source of mortality and premature death. Tobacco smoke contains some 4,000 known chemicals; more than 50 of them are identified to be a source of cancer in human beings. Tobacco smoke in enclosed spaces is inhaled by every person around, divulging smokers and non-smokers in a similar way to its detrimental effects. Mortality and morbidity related with tobacco use is the effect of a countless of multifaceted interactions in the human body [3]. Tobacco control aims to improve the health of community by eradicating, or reducing, burning up of tobacco products and contact to tobacco smoke [4]. It is currently accepted globally that ‘helping tobacco users to quit is part of the role of health professionals, including dentists and other oral health professionals’ and that ‘tobacco cessation is part of the practice of dentistry’. The ethical, moral and practical motives for involvement of oral health professional in tobacco cessation programmes have been established [5]. Health care delivery systems are obliged to recognize and document tobacco use status and treat every tobacco user observed in health care vicinity. Dental professionals play an important job in recognizing smokers, as they may observe intraoral signs such as odour, tooth stains, and oral hygiene problems earlier than other healthcare professionals; consequently they are in a better position to offer preventive care [6]. Additionally, they have access to protocols that support smoking cessation and pharmaceutical facilities if desirable [7]. Dentists’ comprehension about tobacco use and methods offered for its cessation is critical, along with amplified contribution of dental professionals in antismoking campaigns to minimize smokingrelated detrimental effects [8]. Therefore a descriptive study was conducted with the aim to evaluate the dental patients’ knowledge about the consequences of smoking on health and to explore the patient’s approach towards the role of dentists in smoking cessation.
Study tool
An explanatory study was conducted in November 2015 using questionnaire adopted from previous study [9]. The questionnaire includes: Patients’ knowledge about effects of smoking on health (eleven questions), perception toward the role of dentist in smoking cessation (8 questions) and smokers’ willingness to quit smoking on dentists’ advice. As the questionnaire previously used in another research was adopted and modified, Cronbach’s alpha was calculated to measure internal reliability among items.
Study population
Study population consisted of patients visiting Dental OPD of tertiary care facility, Karachi. The study population includes:
• Male or female aged above 15 years
• Smokers (regular and occasional), non-smokers or ex-smokers
• Capable to read, comprehend and respond the survey form
• Give verbal consent to contribute in the study
Data analysis
The collected data were entered into Statistical Package for Social Sciences (SPSS), version 20.0 and were analysed for frequency distributions and χ2.
All patients present at the time of study in Dental OPD completed the survey forms; hence the response rate was 100%. Of 200 subjects, 143(71.5%) were males and 52(26%) were females. The study subjects include regular smokers 70(35%), occasional smokers 40(20%) and non-smokers 64(32%). Smokers were inquired about the reason and inspiration to start smoking. Pleasure seeking (19.5%), curiosity (17%) and hanging outs with friends (15%) were observed the major reasons to start smoking (Figure 1). Media (39%) was observed as the major source of inspiration to start smoking (Figure 2). Twenty three (11.5%) were Ex-smokers; family pressure (42.9%) and health problems (28.6%) were the major stated reasons by Ex-smokers to quit smoking. More than half (52.5%) belonged to the age group of 15-25 years. Eighty seven (43.5%) belonged to lower middle class (Table 1). Mean age of the subjects when they initially start smoking was 18±6.08 years. The internal reliability score for questions in used in study was 0.747.
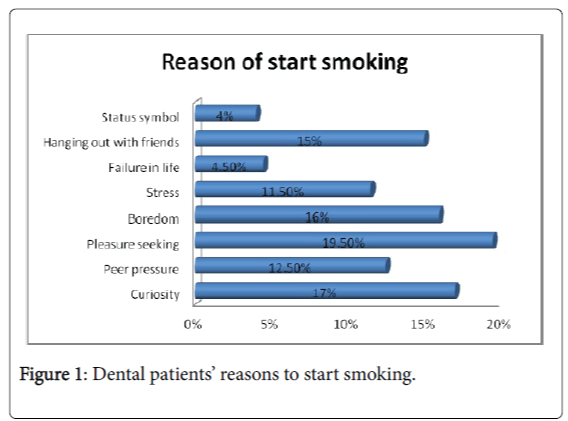
Figure 1: Dental patients’ reasons to start smoking.
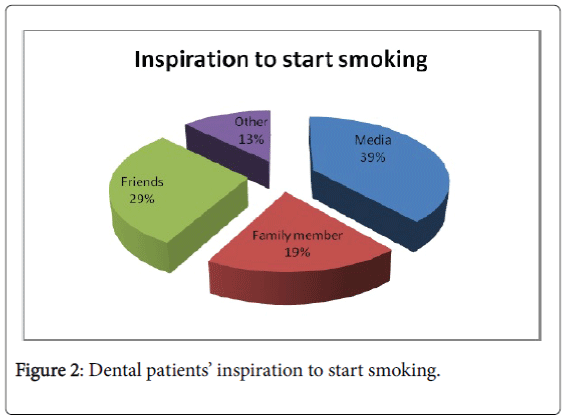
Figure 2: Dental patients’ inspiration to start smoking.
| Variable | Frequency (Percentages) |
|---|---|
| Gender | |
| Male | 143(71.5%) |
| Female | 52(26%) |
| Age(years) | |
| 15-20 | 47(23.5%) |
| 21-25 | 58(29%) |
| 25-30 | 36(18%) |
| 31 -35 | 19(9.5%) |
| 36-40 | 12(6%) |
| 41-45 | 12(6%) |
| 46-50 | 6(3%) |
| 51 and above | 8(4%) |
| Education | |
| Illiterate | 20(10%) |
| Matric | 30(15%) |
| Inter | 49(24.5%) |
| Graduation | 72(36%) |
| Post graduation | 16(8%) |
| Others | 8(4%) |
| Monthly income | |
| Below Rs 25,000 | 78(38.5%) |
| Rs 25,000- Rs 35,000 | 42(21%) |
| Rs 35,000- Rs 50,000 | 21(10.5%) |
| Rs 50,000- Rs 70,000 | 27(13.5%) |
| Rs 70,000 and above | 32(16%) |
| Social status | |
| Lower class | 34(17%) |
| Lower middle class | 87(43.5%) |
| Upper middle class | 45(22.5%) |
| Upper class | 29(14.5%) |
| Smoking status | |
| Smokers | 70(35%) |
| Ex smokers | 23(11.5%) |
| Occasional smokers | 40(20%) |
| Non smokers | 64(32%) |
Table 1: Characteristics of study participants.
In general patients had adequate level of knowledge that smoking causes lung cancer (86.5%), heart disease (74%) and oral cancer (71.5%) (Figure 3). The knowledge of smokers and non-smokers was statistically significant about the facts that smoking causes heart disease (p=0.034) and bad smell from the mouth due to smoking (p=0.030). Non-smokers were well versed of the above facts. Patients’ knowledge about effects of smoking on general and oral health was significantly associated with their age that smoking causes heart disease (p=0.009), discoloration of lips (p <0.0001), periodontitis (p=0.041), bronchitis (p <0.0001) and allergic reactions (p=0.003). Highly significant association was also observed between knowledge of patients and their educational status.
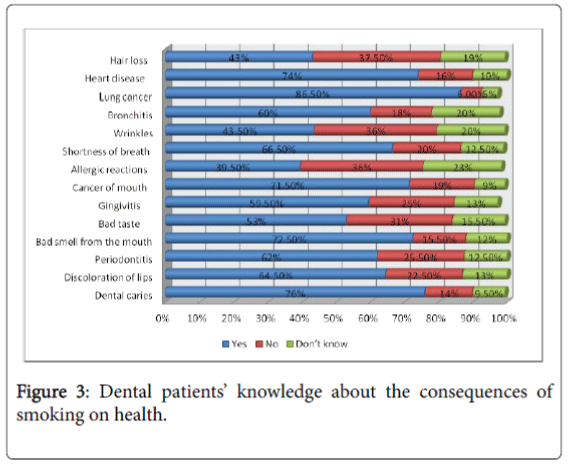
Figure 3: Dental patients’ knowledge about the consequences of smoking on health.
Majority was affirmative about the role of dentist in smoking cessation activities (Table 2). Significant difference was observed in the perception of smokers and non-smokers i.e., their expectation from dentist to provide treatment and tell about smoking (p=0.031), dentist to be interested in smoking status of their patients (p=0.014), dentists should give advice regarding how to stop smoking (p=0.026). Nonsmokers patients were more affirmative for dentist who provides smoking cessation advice to smokers (p=0.046), and ask about patient’s smoking status on each and every visit (p=0.001). No significant association was observed between other independent variables including gender and social status of patients on their perception about the role of dentists.
| Statement | Yes | No | Don’t know |
|---|---|---|---|
| I would expect my dentist to provide treatment and tell about smoking | 124(62%) | 56(28%) | 18(9%) |
| I’d expect my dentist to be interested in smoking status of their patients | 116(58%) | 62(31%) | 17(8.5%) |
| I think dentists should explain effects of smoking on oral health | 128(64%) | 53(26.5%) | 13(6.5%) |
| Dentists can help patients stop smoking | 119(59.5%) | 49(24.5%) | 26(13%) |
| Dentists should give advice regarding how to stop smoking | 124(62%) | 51(25.5%) | 18(9%) |
| Do you like dentist who provides smoking cessation advice to smokers | 116(58%) | 63(31.5%) | 11(5.5%) |
| I would change my dentist if one dentist asks about my smoking status | 97(48.5%) | 68(34%) | 28(14%) |
| Dentist should ask about patient’s smoking status on each and every visit | 122(61%) | 54(27%) | 16(8%) |
Table 2: Patients’ perceptions regarding the role of dentist in smoking
cessation.
Majority (58.5%) smokers agreed to stop smoking if suggested by the dentist (Table 3). They also (63%) agreed to put more efforts to quit if the dentist explains its effect on the oral cavity. Occasional smokers were more willing stop smoking if a dentist suggested so (p=0.004), put more efforts to quit smoking (p=0.010) and go to a specialist for consultation if suggested by the dentist (p=0.001).
| Statement | Yes | No | Don’t know |
|---|---|---|---|
| I would try to stop smokingif a dentist suggested so | 117(58.5%) | 51(25.5%) | 25(12.5%) |
| I would put more efforts to quit smoking if a dentist showed me its effects on the mouth | 126(63%) | 46(23%) | 20(10%) |
| I would go to a specialist for consultation if a dentist suggested so | 124(62%) | 39(19.5%) | 28(14%) |
Table 3: Attitude of smokers toward smoking cessation advice.
In current study the percentage of smoker’s i.e., regular smokers (35%) and occasional smokers (20%) is a fairly good representation of the whole population (46% men and 5.7% women smoke tobacco in Pakistan) [2]. The effects of smoking were in general well recognized by study participants. Patients knew the relationship of smoking and lung cancer (86.5%) which is similar to that reported by other studies [10,11]. Several campaigns and commercials have focused on the smoking as a causal factor for lung cancer therefore the relationship between these two variables are generally known by the public. Association of smoking and heart diseases was somewhat less understood; 74% of the patients knew that smoking cause heart disease owed to the reason that the direct effect of smoking on heart diseases is not manifested and other factors also play a significant role. Another study reported fairly higher level of knowledge [11]. In the present study patient were not adequately well versed that smoking can cause hair loss, allergic reactions and wrinkle formation. Majority (76%) agreed that smoking causes dental caries. Analogous and contradictory results have been reported in other studies [12,13]. The association of smoking and dental caries is a controversial element of research. Recent research indicates that cigarette smoke impairs salivary function and hence leads to encouraging conditions for dental caries [14,15]. Nearly 60% patients in this study believed that smoking can cause gum diseases. Other researches indicate relatively higher percentage [13]. Around 72% agreed that smoking causes oral cancer; Poonam reported nearly 80% patients agreed that smoking causes oral cancer [9].
It has been well acknowledged globally that oral health professionals should incorporate tobacco use prevention and cessation services into their practice [16]. They examine several smokers on regular basis and their counselling could be valuable in promoting healthier life styles. They can help out their patients to stop smoking by identifying oral signs of tobacco use, notifying patients of these and inquiring patients their willingness to discontinue. Dentists’ participation in the tobacco control field will have a dual advantage for their patients: not only to improve oral health but also to contribute in prevention of all the smoking related diseases [17]. In this study, the expectation of patients from dentist to provide treatment and tell about smoking was different among smokers and non-smokers (p=0.031). Some patients consider that choice of quit smoking is one’s personal decision. Moreover, many believe that asking about smoking status and quitting status may be discomforting [18]. The majority of smoking patients showed interest in quitting smoking if the relation among smoking and oral health is proven to them. Findings of the study may assist in focusing educational and interventional programs to patients having greatest risk for these oral conditions.
Dental patients had a good knowledge about the effects of smoking. Majority was affirmative about the role of dentist in smoking cessation activities. It is suggested that oral health professionals should counsel their patients to stop smoking on regular basis as it could be valuable in promoting healthier life styles.
The authors would like to acknowledge Dr. Sadaf Nisar, Manahil Mazhar, Auj Naeem and Ayesha Nisar for their valuable support in collection of data.