Biochemistry & Pharmacology: Open Access
Open Access
ISSN: 2167-0501
ISSN: 2167-0501
Research Article - (2015) Volume 4, Issue 4
Background: Lithium is used in prophylaxis of long term therapy of BPAD as a mood stabilizing agent. Thyroid function abnormality is very commonly seen adverse effect, more common in females than males. This study aims to correlate lithium levels and thyroid function abnormalities associated with it. Methods and materials: Evaluation of medical records of 150 patients in Fr Muller Medical College with BPAD who were treated for 6 months with lithium, Carried out from 12-02-2014 to 20-07-2014. S. lithium levels done by Ion elective electrode method in ilyte analyzer and TFT by electrochemiluminescence. Data are analyzed by Karl Pearson Correlation Coefficient. Results: Correlation of lithium levels and TFT in BPAD patients according to Karl Pearson correlation co-efficient was negative with significant p value of <0.002. Among 150 enrolled candidates 52 (34.67%) were females and 98 (65.4%) were males, 4% (6) patients (3males and 3 females) had TSH value <0.27 with an average lithium value of 1.35 mEq/l, 6% (9) patients (5 males and 4 females) had TSH value >4.2 with an average lithium levels of 0.44 mEq/l and 90% of the patients with an average lithium levels 0.66 mEq/l had no thyroid function abnormalities. Conclusion: As already known lithium is a drug of narrow therapeutic index and females are more prone for thyroid function abnormalities. Appropriate monitoring of serum lithium levels will aid in necessary dose adjustment and ensure proper utilization of drug.
<Bipolar affective disorder (BPAD) also known as manic depressive illness is a brain disorder that causes unusual shifts in mood, energy, activity levels and the ability to carry out day to day tasks. Proper treatment helps many people with bipolar disorder to gain better control of their mood swings and related symptoms. People with bipolar disorder are at higher risk for thyroid disease, migraine headaches, heart disease, diabetes, obesity, and other physical illnesses [1]. Bipolar disorder often appears in the late teens or early adult years. At least half of all cases start before the age of 25 years [2].
Lithium, used in the prophylaxis of Bipolar affective disorder reduces the severity and frequency of mania and also been shown to reduce suicidal risk and short term mortality [3]. Inspite of its efficacy, its use is associated with a number of short comings which include narrow therapeutic index, cardiac toxicity, renal tubular dysfunction and endocrinopathies like hypothyroidism, hyperthyroidism, hyperparathyroidism, hyperglycaemia and nephrogenic Diabetes insipidus. It was also found that thyroid function abnormalities were more common in females than males [4]. Lithium exerts its effects through multiple mechanisms which include inositol depletion as a consequence of which there is increased signaling within the cells [5], induction of autophagy because of which there is degradation of cellular proteins and organelles thus accounting for quality control function [6], Inhibition of NMDA receptor mediated signaling [1,8,10], Inhibition of glycogen synthase kinase 3 (GSK3), which is a proapoptotic and regulator of inflammation and increases the β catenins which is responsible for antiapoptosis of growth hormones [7]. Lithium is also known to exert its action through BDNF up regulation [11].
Lithium preparations are available mainly as lithium carbonate and lithium citrate as immediate and sustained release with a half-life of 1-2 hrs and 4-5 hrs, respectively. Lithium initially is distributed in the extracellular fluid, gradually gets accumulated in the tissues and does not bind much to plasma proteins with a bioavailability of almost 100%. The concentration of lithium in CSF is approximately 40-50% of the concentration in plasma. Lithium is a drug of narrow therapeutic window with a therapeutic range of 0.5-1.3 mEq/l. It is potentially toxic at doses >1.5 mEq/l. Blood for lithium levels should be drawn just prior to the next dose or at least 6-12 hr after the last dose. It has been shown in a retrospective study, that in recurrent depression, the 12 hour lithium levels should be between 0.5-0.8 mEq/l and in mania, levels of lithium between 0.9-1.4 is necessary for optimal results [8].
The normal functioning of the thyroid gland is affected by multiple mechanisms of lithium. Lithium gets accumulated in the thyroid gland and inhibits the synthesis and release of thyroid hormones probably by affecting cellular microtubule function. Lithium also alters the thyroglobulin structure and thus affects the function and protein conformation which leads to coupling defects of iodotyrosine. Lithium administration is associated with reduced hepatic de-iodination and clearance of free T4 by decreasing the activity of 1-5`de-iodinase enzyme. Lithium is also known to increase the propensity to thyroid autoimmunity in individuals who are susceptible [9]. The mechanism by which it exerts its mood stabilizing effects are still not clear. In this study an attempt to correlate the lithium levels and thyroid function abnormalities associated with it has been made.
The study was carried out from 01-03-2014 to 15-07-2014 for a period of 5 months. Patients clinically diagnosed with bipolar affective disorder on lithium between 18 yrs to 65 yrs of either sex were included in the study. Patients who are previously diagnosed with thyroid dysfunction and on treatment for the same and patients with serious medical disorder endangering life were excluded from the study. Data was collected from the department of Psychiatry, Father Muller Medical College Hospital from patients clinically diagnosed to have bipolar affective disorder. A sample size of 150 was studied. After a written informed consent was taken both from the patient as well as the patient`s relatives. Patients diagnosed with Bipolar Disorder who did not have a thyroid abnormality or on any drugs which can alter thyroid function at entry were evaluated. Serum lithium levels estimation was done by Ion selective electrode method in ilyte analyzer and TFT by electrochemiluminescence method. Data was analyzed by Karl Pearson Correlation Coefficient, Chi square and Standard deviation.
Correlation of lithium levels and TFT in BPAD patients according to Karl Pearson correlation co-efficient was negative with significant P value of <0.002. Among 150 enrolled candidates 52 (34.67%) were females and 98 (65.4%) were males. 6 patients (3 males and 3 females) had TSH value <0.27 with an average lithium value of 1.35 mEq/l.6%. 9 patients (5males and 4 females) had TSH value >4.2 with an average lithium levels of 0.44 mEq/l . 90% of the patients with an average lithium level 0.66 mEq/l had no thyroid function abnormalities (Table 1).
| Age Distribution | Number of Patients | Percentage |
|---|---|---|
| ≤ 20 | 8 | 5.34% |
| 20-30 | 37 | 24.67% |
| 30-40 | 36 | 24% |
| 40-50 | 37 | 24.67% |
| 50-60 | 15 | 10% |
| ≥ 60 | 17 | 11.34% |
Table 1: Percentage distribution based on age groups.
In our study we found that at higher serum lithium levels in the therapeutic window the most common thyroid abnormality seen was hyperthyroidism, i.e., at serum lithium level of 1.35 ± 0.15 mEq/l. Hypothyroidism was common at serum lithium levels of 0.44 ± 0.12 mEq/l and the patients with serum lithium values falling in between these values were apparently normal with respect to their thyroid function. T3 and T4 levels were not uniformly distributed because of which we could not correlate their levels with serum lithium levels (Figures 1-3).
Figure 1: Sex distribution in the study population.
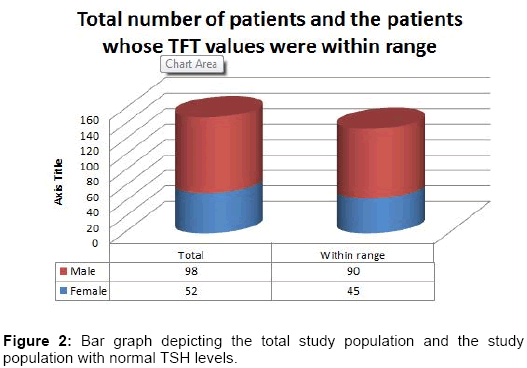
Figure 2: Bar graph depicting the total study population and the study population with normal TSH levels.
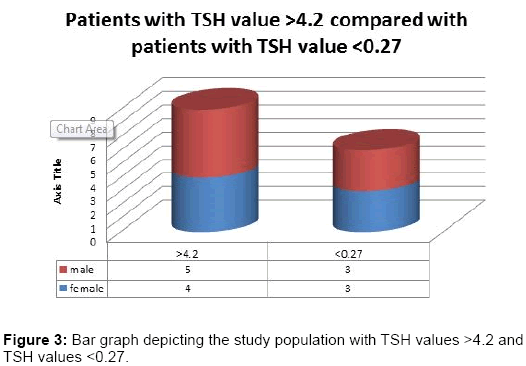
Figure 3: Bar graph depicting the study population with TSH values >4.2 and TSH values <0.27.
Perrild et al. and few other studies found that there is no gender difference with regard to thyroid dysfunction.[12] Several other studies have shown that there is higher incidence of lithium induced thyroid abnormality in women [13,14] which is in agreement with our findings.
In cross sectional study by Kirov et al. among 115 males and 159 females with affective disorders on long term lithium therapy in the UK, the prevalence of hypothyroidism was 10.3% [15]. Bocchetta et al. in a study among 150 ambulatory Sardinian patients on lithium therapy, no cases of clinical hypothyroidism was found. Subclinical hypothyroidism was noted in 19% of the patients. Among lithium treated patients with positive thyroid antibodies, the prevalence of subclinical hypothyroidism increased to 53%. The prevalence of specific anti-thyroid antibodies was positively correlated with age and duration of lithium treatment, and was higher among women [16].
Bocchetta et al. and Chakrabarti concluded that risk of developing lithium induced hypothyroidism has been shown to be significantly higher among females, with increasing age (>50 years), presence of family history of thyroid disease and thyroid auto-antibodies [17,18].
As the serum levels of lithium increases TSH levels decreases and vice versa. Females on lithium therapy are more prone for thyroid dysfunction hence the clinician must be more vigilant while treating females with lithium. Further studies are required to establish the particular thyroid dysfunction in correlation with serum lithium levels. With the help of which, the clinicians can set stage for the anticipated thyroid dysfunction.