Drug Designing: Open Access
Open Access
ISSN: 2169-0138
ISSN: 2169-0138
Case Report - (2014) Volume 3, Issue 3
The main objective of this clinical case presentation is to attract attention to the risk of contraceptive pills in the development of nodules in the breast.
<Keywords: Contraceptives pills, Breast cancer
During the last few decades, many contraceptive methods and medications have been developed. Some of these methods and medications are steroidal in nature (pills) whereas others are mechanical. Today, pharmaceutics offer different contraceptive products, from which people may select. Ideally, contraceptives should give the maximum contraceptive outcomes as well as a minimum of side effects. Although the current contraceptive pills have been found to be significantly effective in producing contraception, the question is “are they really safe?" Many investigations have shown that women using steroidal contraceptive pills have had serious side effects such as: clots in the legs and lungs, breast lumps, depression, headache, nausea, vomiting.
We present the clinical case of a 32 years old woman who started the use of contraceptives pills at 22 years old. So she used contraceptive pills for a long period of time– approximately for ten years with short periods free 2-3 months/year. She used Diane 35 – this type of contraceptive pill during that period. She took one pill/day for 21days with 7 days free in ten years with a pause 2-3 months/year. These pills are biphasic contraceptives because they contain a combination of two important components: cyproterone and ethinyl estradiolCyproterone represent antiandrogens group and ethinyl estradiol significant a group of medications known as estrogens. She didn’t try other types, like triphasic birth control pills. These pills are contraindicated if we suspect a tumor development due to an estrogen on breast cancer.
When she came to the consultation she felt pain in the right upper lateral area of the thorax and under the right breast and was very anxious, depressed and said, she had lost approximately 8 kg of weight and also have appetite.
At the objective examination she was pale, thin, with evident asymmetry of the breast- the right breast bigger compared to the left breast, at the palpation of the right breast a nodule was discovered with approximate dimensions of 1,5/1,2cm, with increase consistence, irregular border, painful, with low mobility compared to the tissues around. No lymph nodes in both axilas. The appearances of the patient follow in the images below where we see: the paleness of the face, the paleness of the palms (natural hemoglobin meter) (Figure 1), the asymmetry of the breasts (Figure 2).
Figure 1: The paleness of the palms
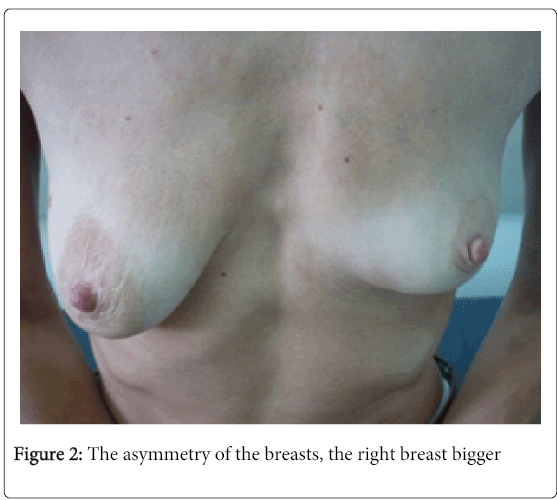
Figure 2: The asymmetry of the breasts, the right breast bigger
The nodule was also confirmed after the mammography examination (Figure 3) and ultrasonography of the breast (Figure 4).
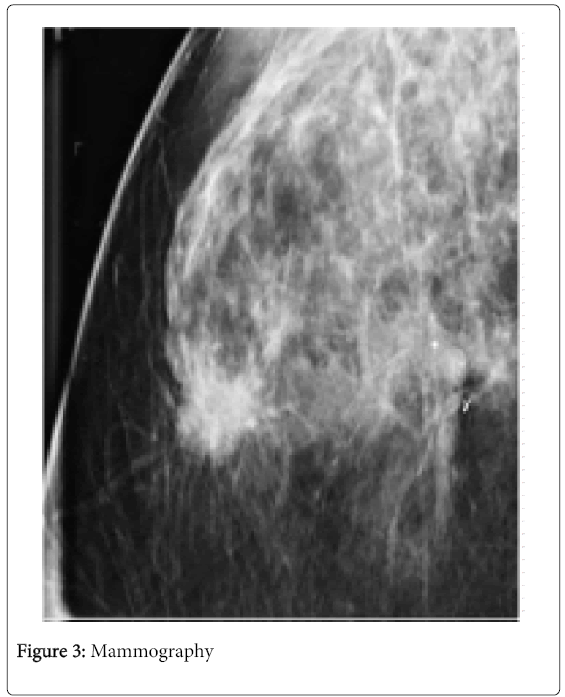
Figure 3: Mammography
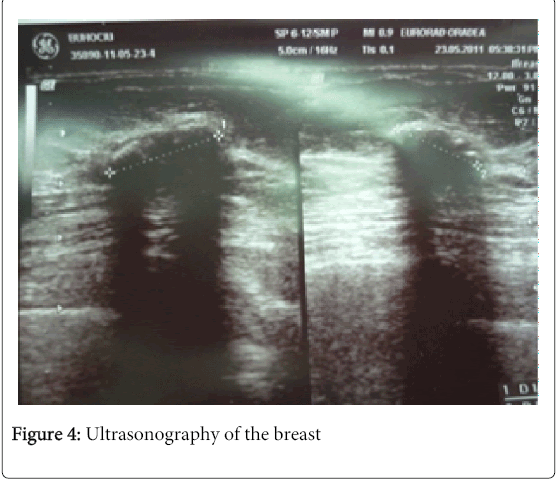
Figure 4: Ultrasonography of the breast
The blood tests revealed: ESR=88/102mm1h-2h, fibrinogen=583mg%, Hb=10g/dl, Ht=39%, Red blood cell=3milions/mm³, other lab tests where in normal range except the marker CA 15.3 positive. The patient refused biopsy of the nodule of the breast but accepted the surgical intervention. After this was performed the histopathological examination (Figure 5) from the operator piece confirmed adenocarcinoma of the breast.
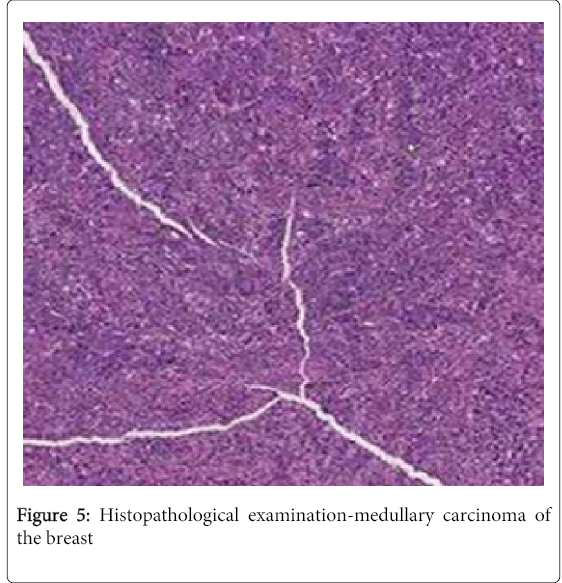
Figure 5: Histopathological examination-medullary carcinoma of the breast
The immunohistochemistry examination (Figure 6a and 6b) of this patient with medullary carcinoma of the breast was ER negative / PR negative tumor with good prognosis (ER- estrogen receptor, PR-progesterone receptor).
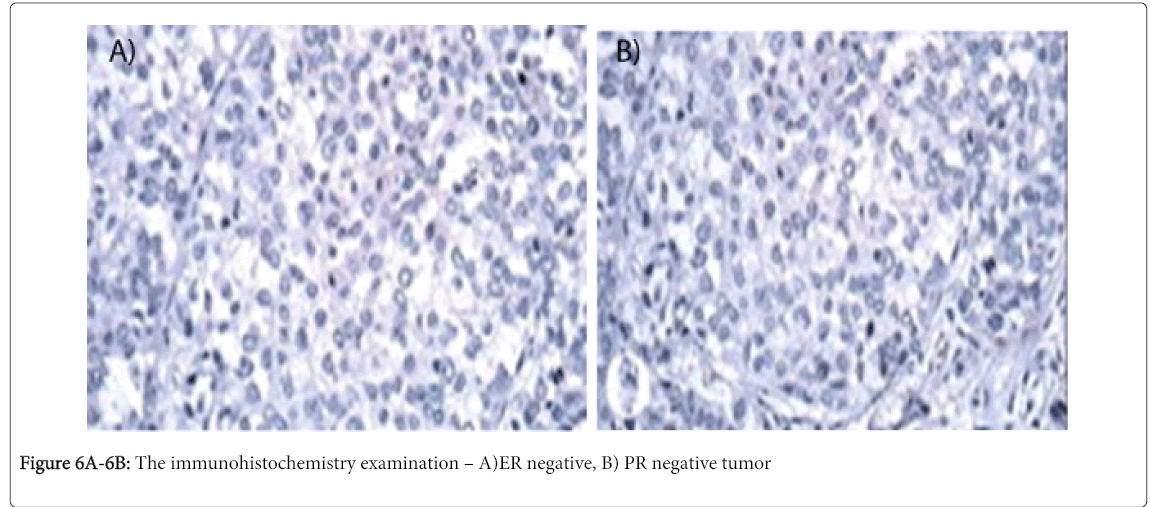
Figure 6: The immunohistochemistry examination – A)ER negative, B) PR negative tumor
Actually, these immunohistochemistry markers are usually performed in the breast cancer: specifically estrogen receptors, progesterone receptors and HER2 (human epidermal growth factor receptor 2). Also HER2 was negative at this patient.
She performed after the surgery the complete protocol with irradiation and chemotherapy with good evolution of the patient’s clinical picture. We mentioned that she didn’t have a history of breast cancer in the family. She has a very good life style, and does not consume any toxic products (coffee, alcohol, cigarettes and drugs), performed sports (aerobic) twice per week, without other risks factors in her personal history. The genetic screening test was negative. The patient was checked for mutations in her BRCA1 and BRCA2 genes which have a 50-80% lifetime risk of developing into breast cancer, but was negative. Some studies take a look at how birth control can affect those who already have a genetic risk of developing breast cancer. In our long medical practice, we observed many women patients with a similar situation.
We observed more than 50 patients in the same clinical context, with negative mutation in their BRCA1 and BRCA2 genes and after a different period of consumption of the contraceptives pills (Diane 35), the nodules in the breast appear and all the cases were after surgery of the breast and histopathology examination, medullary carcinoma of the breast and all the women were without genetic risk, without a history of the breast cancer in the family. Other observations were about 40 women with ovarian cyst disease who followed a contraceptive pill scheme therapy to prevent the increase in volume of the ovarian cyst and could avoid surgical intervention, but after a variable period of therapy in all the patients there appeared nodules in the breast confirmed after a histopathology examination, like carcinoma of the breast and more than that they had to perform a partial or total resection of the ovary because the cyst increased in volume after contraceptive pill consumption.
Of course, the length of contraceptive use increased the risk, but we saw young women who developed nodules in the breast after only five, four or three years after consumption. Another observation is that very young women are more sensitive and the evolution of the breast cancer is very fast because there exists an increase cell turn over for the young patient.
After so many clinical observations- more than 50 cases - from my medical practice, after 15 years, we feel a duty to write this article because women are in danger with this method of contraception and majority of them know nothing about this. More than that, today, we have other possibilities for contraceptive methods to protect the women against pregnancy. How is it possible for this to happen?
A 1996 analysis of epidemiologic data from more than 50 studies worldwide by the Collaborative Group on Hormonal Factors in Breast Cancer found that women who were current or recent users of birth control pills had a slightly higher risk of developing breast cancer than women who had never used the pill [1].
A recent analysis of data from the Nurses’ Health Study, which has been following more than 116,000 female nurses who were 24 to 43 years old when they enrolled in the study in 1989 [2], found that the participants who used oral contraceptives had a slight increase in breast cancer risk. However, nearly all of the increased risk was seen among women who took a specific type of oral contraceptive, a “triphasic” pill, in which the dose of hormones is changed in three stages over the course of a woman’s monthly cycle.
Last summer, in a study of more than 50,000 African-American women, Boston University epidemiologist Lynn Rosenberg found a 65 percent increase in a particularly aggressive form of breast cancer among those who had ever taken the birth-control pill. The risk doubles for those who had used the contraceptive within the past five years and had taken it for longer than 10 years [3].
The best data available suggest that women who currently use oral contraceptives or who have used them in the previous 10 years have a slightly increased risk of breast cancer, whereas women who have used oral contraceptives less recently do not have an increased risk [1,4].
A recent study [5] suggested that among women who had a first-degree relative with breast cancer, the risk of breast cancer among those who had used oral contraceptives before 1976 (when preparations were likely to contain high doses of estrogen and progestin) was three times as high as the risk among women who had never used oral contraceptives.
Young women with BRCA1 or BRCA2 mutations who have used oral contraceptives may have an increased risk of breast cancer [6].
The balance between the level of estrogens and progesterone hormones from the contraceptives pills has an important role in this process. The CA 153 marker was positive in all these cases. The question is how is it possible for all these Side effects to occur? It is clear that a connection exists after many clinical observations and the explanation is the presence of estrogen and progesterone hormones in contraceptives pills. The higher the levels of estrogen contained in the pill the higher the risks.
The other risk category represents the women with ovarian cyst who follow therapy with contraceptive pills to prevent the increase in dimensions of an ovarian cyst. Very many cases of women with this pathology have been observed in our medical practice, when the discovery of the ovarian cyst is late it is followed by us surgical intervention after which this therapy must be observed. These are the real clinical observations, pertinent and worrying and should not be ignored, more importantly this should be taken seriously into account in order to avoid this situation in the future. We have to learn something from the negative and unhappy experiences of others in order to prevent this in the future.
Contraceptive pill consumption presents risk factors in development of nodules in the breast and the histopathology examination confirmed medullary carcinoma of the breast For women without genetic risk factors. The Longer the duration of the consumption the greater the risk and very young women are more sensitive because there exists an increase cell turnover at young age and this is the reason for a fast evolution. In the end the question is: there represents a large variety contraceptive methods today do they represents a much smaller risk to the health of women?
•The contraceptives pills consumption represents the risk factor in development of nodules in the breast and the histopathology examination confirmed medullary carcinoma of the breast in the women without genetic risk factors.
•The longer the duration of consumption of these pills the greater the risk.
•Younger women are more sensitive due to the faster turnover of cells making the evolution faster.
•In the end the questions are: does the contraceptive pill represent the best option in an era where there are many other choices for contraception, when many of the other methods have had much lower side effect?
•Contraceptive pills represent the best choice treatment in an ovarian cyst?