Medical & Surgical Urology
Open Access
ISSN: 2168-9857
ISSN: 2168-9857
Research Article - (2018) Volume 7, Issue 4
Purpose: To distinguish the ESWL and PCNL treatment procedures of 1-2 cm of lower calyceal renal calculi in order to assess the ability and safety of the procedures.
Materials and Methods: Patients that undergone treatments within the time frame of June 2015 to March 2018 was selected for the study. 220 patients were identified, where; they were diagnosed with stone size ranging from 1-2 cm in lower calyceal. Selected patients were grouped into to Extracorporeal Shock Wave Lithotripsy (ESWL) and Percutaneous Nephrolithotomy (PCNL) groups. The demographic information comprising age, gender, size of the stone, operation time and stone-free rate (SFR) was collected and analyzed. After the operation, identified patients were tested with stone detection procedure (KUB and US) and CT scan at day 10th and 12th week respectively.
Result: It was observed that both groups were eligible for preoperative parameters comparison. The mean (SD) of operating time was significantly longer for Group B [6.71 (38) mins] compared to Group A, yet statistically significant as the p-value was <0.001. On the other hand, the SFR value obtained for both groups were different, 27% and 82% for Group A and Group B respectively.
Conclusion: In summary, it was proven that both ESWL and PCNL treatment procedures are comparable for treating lower calyceal stones ranging from 1-2 cm. Despite having the longer hospital stay and intraoperative complications, PCNL was observed to have longer operating time compared to ESWL. Besides that, PCNL also possesses a higher tendency of post-operative infection as the SFR value obtained was higher than ESWL.
Keywords: Lower pole calyx; Extracorporeal shockwave therapy; Percutaneous nephrolithotomy; Stone-free rate
KUB: Kidneys, Ureters, Bladder; US: Ultrasound; ESWL: Extracorporeal Shockwave Therapy; PCNL: Percutaneous Nephrolithotomy; SFR: Stone-free Rate; Cm: Centimeter; Mm: Millimeter; CT: Computed Tomography; i.v: Inter Venous; SPSS: Statistical Package for Social Sciences; SD: Standard Deviation; n: Number; h: Hour; Sec: Second; min: Minute
A significant rate of occurrence and economic cost has remained renal stones detection as one of the common urological problem occurring worldwide [1]. Existing researches predicted an increase in the kidney stones cases mainly caused by tremendous lifestyle changes, unhealthy diet, obesity and also global warming [2]. Great venture in health science and technology has developed advanced procedures in the kidney stones treatment. In the past, invasive open surgical techniques were widely used to treat kidney stones. However, with the advancement of science and technology in the medical field, the treatment is either non-invasive such as shockwave lithotripsy or minimally invasive such as ureteroscopy (endoscopic) and percutaneous nephrolithotomy [3]. Extracorporeal shockwave lithotripsy (ESWL) has been widely accepted as the treatment of choice for renal stones less than 2 cm, with variable success rates of 60%–99% across the globe [4]. Due to science and technological advancement, urologists and patients doubt ESWL as the most essential treatment for stone removal [5-7]. Since the 1970s, percutaneous nephrolithotomy (PCNL) has been used as a replacement of open surgery, especially for large stones. When the rate of kidney stone occurrence reduced, the urologists began to use the PCNL method for removal of mid-sized stones as well. Besides the stone size, body habitus, anatomy of the renal, costs involved, availability of infrastructure and patients’ preferences are among the factors that need to be considered while selecting the treatment mode for kidney stone [8]. Throughout the years, various studies have been conducted and found limited cases, various stones in lower calyx size with definition [9-12]. In this research work, the differences between PCNL and ESWL method is distinguished so that the efficiency and safety on handling lower calyceal stones within the range 1–2 cm can be assessed.
The study was carried out at Department of Urology, Shahid-Ghazi Hariri Surgical Specialists Hospital located in Medical City of Baghdad, Iraq. Patients who undergo kidney stone treatment from June 2015 to March 2018 were selected for this study. Over 260 patients were observed for the study. However, patients aged between 20-70 years were randomly selected. Loin pain, with or without hematuria resulting from calyceal stones of 1–2 cm were set as criteria of patients’ selection for the research. A radiologist was appointed to perform measurement on the size of calyceal stones via non-contrast abdomen CT procedure.
We did randomized controlled trial of patients with lower pole calculi stones of 1-2 cm in the Department of Urology. This randomized controlled trail was designed by the professional staff and was reported following the proposed Consolidated Standards of Reporting Trials (CONSORT) Statement [13]. We followed the current edition of the Declaration of Helsinki and our study was approved by the local Ethics and Research Committee. Informed consent was obtained from all participants, who declared that they had read the participation information booklet and understood the purposes and requirements of the study. All participants signed an informed consent form before enrolment. Selected 220 patients were divided into two groups of treatment method, following both surgeons' and patients' preference. For each patient, their medical history was collected alongside with medical examination and laboratory procedures. Laboratory proceedings comprise investigation on the kidney and liver functionality, blood count, fasting blood sugar level, bleeding profile, urine analysis and culture. Selection of patients for the study also includes those who were having lower pole stones of 1–2 cm with wellexcreting kidney in absence of congenital abnormalities. Patients younger than 20 years old and pregnant women were excluded from this study. Besides that, those diagnosed with multiple renal stones, renal pelvis stone, the presence of renal stone in anomalous kidney, high bleeding tendency, and renal failure, bilateral renal stones, the patients with real impairment and the patients who need second and third ESWL sessions were excluded from this study.
Procedure
Initially, patients in both groups were subjected for urine examination. Patients diagnosed with UTIs were provided with antibiotics following their urine culture and sensitivity. Then, urine examination was conducted again. Next, patients were provided with prophylactic antibiotic directly before the treatment process. It was supplied in the form of 1 g of ceftriaxone continuously for the following 48 hours. The treatment success is derived as the complete elimination of the lower calyx stones, the absence of stone or presence of clinically insignificant residual stones ranging <4 mm. The success rate of the treatment is also evaluated from the stone size and site [14].
Group A-ESWL
Group A consists of 110 patients. They were subjected for ESWL treatment using equipment of Siemens Model Lithostar Multiline, Nixdorf and Modular RLX2- 120.034.06. The equipment used in this study has an operating voltage of 104.4 kV, 4.2 mA current and power ranging from (0.1-9) watt. Besides that, the equipment has both ultrasonography and fluoroscopic display with huge energy density to attain optimum focus. These criteria enable the equipment to induce very minimal pain which happens seldom while mild sedation. For ESWL treatment, the maximum number of shock waves was set to 3000 with energy level 4 for one session. Similar with the existing modern equipment, the equipment used in the study used the electromagnetic source. Shock waves are transmitted to the body via water and focused with the aid of the acoustic lens system. This enables the reflection of released energy on the surface of the stone. Imaging techniques (KUB and ultrasound) are used to measure the stone size.
Group B-PCNL
Group B also consists of 110 patients, who were subjected for PCNL treatment method. Prior to the treatment process, all the patients were entitled to standard fluoroscopy-guided renal access. It was performed as the patient lying flat after the retrograde ureteric catheterization, under the influence of spinal or general anesthesia. It was performed by a surgeon well versed in endo-urological procedures. To ensure the accuracy of puncture fluoroscopically and to distend the pelvicalyceal system, the retrograde 5 F catheter was used. It was done by contrast injecting that delineates the posterior calyx precisely. Each patient was subjected to 10 mg of furosemide, i.v bolus diuretic injection before initiating the treatment procedure. Past medical histories proved that furosemide has the tendency of sustaining and uniformly distance pelvicalyceal system throughout the treatment duration. Besides that, furosemide also plays an essential role as a supplement for the installation of the saline through the retrograde catheter. The initial puncture was made using biplanar-C arm fluoroscopy. The nephroscope used were storz adult size with 24,26 fr, percutaneous nephrostomy (PCN), we`re left situ at the end of procedure. 18–20F nephrostomy tube were placed in all patients as required at the end of PCNL procedure. Generally, the posterior calyx is selected for puncture, unless if the stone is located directly on the anterior calyx since it will be difficult to approach via adjoining the posterior calyx. Stone fragmentationand removal were accomplished using lithotripter pneumatic, Besides that, patients of Group B were subjected for an ultrasound at 10th day and non-contrast CT at the 12th week of post PCNL treatment, to affirm that the stone has been removed completely. Throughout the follow-up process, all the complications faced by patients were recorded.
Sample size
Using the previously reported outcomes for stone-free rate from similar study [15], the rate was 37% and 85% in ESWL and PCNL, respectively. Following published guidelines [15], we calculated the sample size based on 95% statistical interval at a 5% significance level aimed to detect a difference between the two groups. A sample size of 200 was deemed. By allowing for an attrition rate of 30%, we estimated that a total sample size of participants 260 (130 per group) would be sufficient, with an expected drop-out rate of participants. Figure 1 shows the flow process of participants through trial.
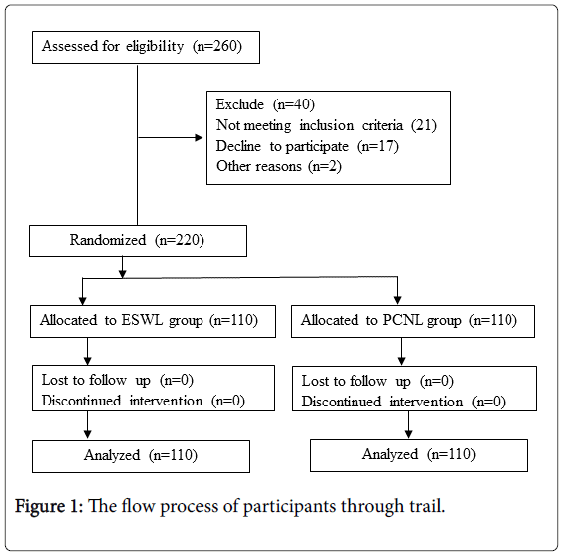
Figure 1: The flow process of participants through trail.
Statistical analysis
The inferential statistical approach was used in this study with the aid of IBM SPSS Statistics (Version 25.0; IBM Corp., Armonk, New York, USA). Results obtained are denoted as mean (SD) value or rate (%) where appropriate. t-test approach was used to distinguish both groups. Considering the data obtained as a normal distribution, Chi- Square Test method was used to compare categorical data (numerical). p-value lesser than 0.05 indicates that there is statistical significance.
Throughout the study, all the patients from both groups were treated at the same center. For Group A, ESWL treatment group, there were 64 men (58%) and 46 women (42%). For Group B, PCNL treatment group, there were 66 men (60%) and 44 women (40%). Overall, an approximate rate of 2:1 was observed for a male to female in this study. The comparable pre-operative parameters are tabulated in Table 1. For Group A, the average age of the patient is 40 years old, meanwhile, for Group B, it was 39 years old. In Group A, the average of stone size observed was 15 mm (within range of 10–20 mm) and for Group B the average is slightly higher, 17 mm (within the range 12–20 mm). However, there was no any difference distinguished between the 2 treatment modalities for both genders.
| Variable | Group A ESWEL |
Group B PCNL |
P-value |
|---|---|---|---|
| Gender. N (%) Males Females |
64 (58) 46 (42) |
66 (60) 44 (40) |
0.51 |
| Mean (SD) Age, years |
40 (10.7) | 39 (12.4) | 0.001* |
| Stone size, mm range | 15 (10-20) | 17 (12-20) | 0.001* |
| Stone side. n(%) Right kidney Left kidney |
50 (45.5) 60 (54.5) |
58 (52.7) 52 (47.3) |
0.21 |
Table 1: Clinical characteristics of treatment groups in the study.
Comparing the operation time, Group B has longer duration compared to Group A, with p-value <0.001, as tabulated in Table 2. 30 patients (27%) from Group A showed positive progress when they were diagnosed with zero stones at the 12th week. However, the number of patient with zero stones is higher in Group B, 90 patients (82%) were diagnosed to be fully free from renal stones on the 12th week of post-PCNL treatment. Besides that, the statistically significant difference was observed between the groups, in the context of SFR (p<0.001). The average time taken for fluoroscopic procedure is longer for Group A compared to Group B. However, Group B had a longer hospitalization duration compared to Group A. In context of complications, hematuria was observed in all patients in Group A, similar to Group B. However, for Group A, none of the patients developed severe bleeding despite the hematuria. For the PCNL group, neither patient faced secondary injury or organ injury. However, 8 patients (7.3%) of Group A had the infection and were hospitalized for treatment after the ESWL treatment. Similarly, 9 of Group B patients (8.2%), diagnosed with a post-operative infection and hospitalized for antibiotic treatments. 25 patients of Group A were treated with JJ stent right after their EWSL treatment.
| Variable | Group A ESWEL |
Group B PCNL |
P-value |
|---|---|---|---|
| Operative duration, min Mean (SD) range |
33 (0.00) 33 |
38 (6.71) 30-66 |
0.001* |
| Fluoroscopic time, sec Mean (SD) range |
59 (6.09) 40-77 |
55 (12.05) 30-90 |
0.001* |
| Hospital stay, h Mean (SD) range |
2 (0.00) 2 |
20 (2.88) 12-26 |
0.001* |
| Stone free rate, n (%) Yes No |
30 (27.3) 70 (72.7) |
90 (81.8) 20 (18.2) |
0.001* |
| Complication, n (%) Postoperative infection Hematuria |
8 (7.3) 110 (100) |
9 (8.2) 0 (0.0) |
0.38 |
Table 2: The patients’ operative characteristics.
Generally, ESWL treatments are essential and easy and always the common operation option for the kidney stone removal. It is less invasive compared to other treatment techniques. However, urologists face difficulty to achieve clearance for renal lower calyceal stone after the first ESWL session. Medical histories do not record the success story of renal lower calyceal stone removal by first ESWL session treatment process. In spite of the satisfactory discontinuity, the gravity drive holds up the pieces in the lower calyx which has a turnaround point [16,17]. Emerging studies compared and distinguished PCNL and ESWL methodology in order to establish the stringent treatment of lower calyceal stone with <2 cm size [18].
Similar to the latest studies, this research work also reports consistent results. The efficiency and safety of handling renal stones via a comparative study of PCNL and ESWL treatment methods are carried out by various researchers. Consistently, the studies are proving that PCNL offers a better solution for removal of renal stones [19,20]. Average age group of patients in the study was 39.6 ± 11.57, with a median of 39 years old. In this research, the age group of the patients is wide, 20–70 years old, similar with work of Fayad et al. which comprises patients in the age group of 20–60 years, with an average of 46.3 years. Comparing the work with previous studies, the sociodemographic characteristic resembles each other in the context of age and gender distribution. A study by Fayad, et al. [21] focused on 120 patients, with distribution of 60% male and 40% females, similar to this study. On the other hand, the average stone size observed for EWSL patients was 15(10-20) mm, meanwhile for PCNL patients, the average stone size was 17 (12-20) mm. From the existing literature by and Das, et al. [22] and Ather, et al. [23] the stone size for EWSL was 9 ± 4 mm and were 1.07 cm respectively, which deviates far from the findings of this study. However, for PCNL, the finding was statistically significant with Fayad, et al. study, 14.7 ± 0.3 mm.
SFR for PCNL explored in this study are similar to Albala et al., [18] as higher SFR is observed for PCNL compared to EWSL, with 95.8% and 40% respectively. Yuruk et al. [24] also reported that comparison of PCNL and EWSL resulted in 96.7% of SFR for PCNL meanwhile 56.7% for EWSL. The study was carried out with 62 patients with lower calyceal stones of <2.0 cm. His findings were better than the findings of Kuo, et al. [25] which documented 66.7% SFR for PCNL. However, SFR for EWLS relatively smaller compared to previous studies by Kumar, et al. [26] (86.6%) and Singh et al. (85.7%). Overall, comparing both treatment approach studied in this research, it can be concluded that SFR for PCNL is way better compared to ESWL, and it was significant statistically
In the context of complications, in this study, no intra-operative that needs the attention of a surgical or radiological approach occurred. Hematuria was a common complication for both groups in this research although it was observed in previous studies. Overall, in patients who treated by ESWL with on session an experienced unsuccessful stone free rate the management was done by go through second and third ESWL sessions but we exclude their results. There are certain limitations in the present study. These include its single center origin, relatively small sample size in the both groups, most patients with lack of information about the treatment methods of renal stones and refuse to collaborate in the study. some patients refused to do computerized tomography (CT) scan in order to radiation dose and high cost, which is more sensitive for this purpose, also we don’t use flexible lithotripters and baskets to reduce size of fragments [27]. All above shortcomings, leads to get small sample size.
It can be concluded that treatment of lower calyceal stones in the size of 1–2 cm is still a challenge for the urologists to identify the best SFR techniques from the existing treatment methods. Meanwhile, for treatment of lower calyceal stones, both PCNL and ESWL show inconsistency in the context of SFR, complications and hospitalization duration. Comparatively, ESWL method displayed statistically significant shorter operation time. Although PCNL holds its position as minimal invasion procedure, it has relatively longer operation time and possesses a higher tendency of post-operation fever and infection. It was also a common occurrence during the stone migration under PCNL treatment procedure.
The ethics committee approved the study and all patients were informed about the study and a signed written consent was obtained.
The author declared that there is no conflict of interests regarding the publication of this paper
None
Protocol/project development: Nima & Ibraheem
Data collection or management: Nima & Ibraheem
Data analysis: Ibraheem