Advanced Techniques in Biology & Medicine
Open Access
ISSN: 2379-1764
ISSN: 2379-1764
Case Report - (2013) Volume 1, Issue 2
Pilomatricoma is benign skin tumor originates from outer sheath of hair follicle cells and is usually locates on head, neck and upper extremities. 40% of pilomatricomas are diagnosed in the first decade of life. It is most commonly seen between the ages of 8-13 in children. These nodular tumors are rarely multiple and familial. Pediatricians are not so familiar to these tumors, so true initial diagnosisis is not usually feasible. The definitive diagnosis is made by histopathological examination of tissue obtained by excisional biopsy. Although its rare, because of tumors metastasis potential and recurrence potentiality in cases that accurate excision could not be obtained, wide surgical excision should be performed. The incidence of recurrence is very low. In this report; 10 months old male patient with pilomatricoma, diagnosed by pathology procedures, is presented who was examined detailly many times due to huge puffy mass in the head kept growing from 4 months of age.
Pilomatricoma (Malherben’s calcifying epithelioma) is usually slow-growing, asymptomatic, benign skin tumor. The tumor cells originate from outer sheath cells of hair follicle. These tumors are wellcircumscribed, rigid, 5-30 mm in size, deep dermal and subcutaneous masses and are generally seen between 5-15 years of age, on the head, neck and upper limb. Pilomatricoma is often solitary nodule, but also can be multiple and familial. Diagnosis is made by histopathological examination of the excisional biopsy [1,2].
In general, clinical diagnosis is overlooked by physicians who are not familiar with this tumor. Improve in physicians’s knowledge about pilomatricoma should decrease unnecessary detailled investigations and increase true clinical initial diagnosis rates.
Ten-month-old male patient was admitted because of a mass growing on the forehead. The mass was noticed for the first time at four months of age and antibiotics were used with abscess diagnosis. The patient had not a history of trauma exposure and infection. Physical examination showed stable vital signs and semi-mobile, mediumhard, hairless, rough, very fluffy, pink purple, 3×2.5 cm sized mass on frontal vertex (Figure 1). Other systemic examinations were normal. Laboratory testings showed WBC: 8300/mm3, Hb: 11 mg/L, Hct: 32%, platelets: 276000/mm3, ESR: 18 mm/h. Biochemistry and urinalysis were normal. Alpha-fetoprotein level, viewed with suspicion of initial diagnosis teratoma, was 32 ng/mL (0-80).
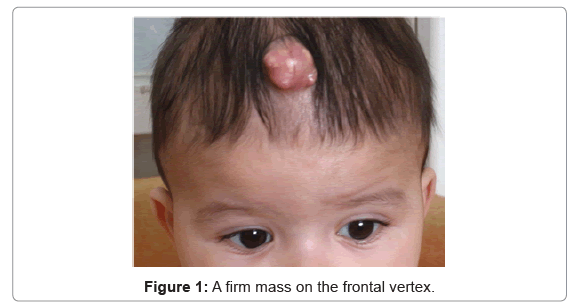
Figure 1: A firm mass on the frontal vertex.
By ultrasonography; hypoechoic, globe, mobile, regular contoured, 2 cm in diameter mass in subcutaneous adipose tissue on the frontal area was detected. A well-circumscribed 1.5×2 cm sized round mass with calcified appendages is detected by computed tomography at an external center of 4 months of age. Excisional biopsy of the lesion is made by total removal. The histopathological examination of mass showed eosinophilic stained, and in some areas calcified, epithelial islands formed from basoloid cells. Vascular and perineural invasion was not observed (Figure 2). Case was diagnosed as pilomatricoma, by these histopathological signs. The physical examination of patient was normal at 2 years old, and relapse was not observed during follow-up.
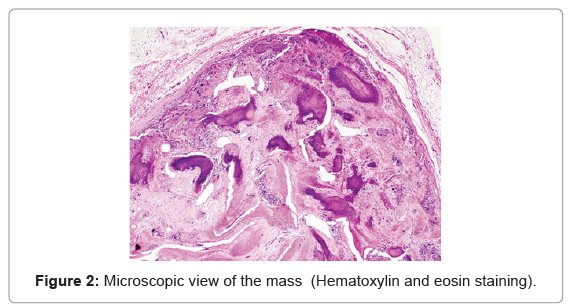
Figure 2: Microscopic view of the mass (Hematoxylin and eosin staining).
Pilomatricoma is seen usually at the head, neck and upper extremities, and less frequently at trunk and lower extremities. Lesion is solitary, firm, well-circumscribed, slow-growing, asymptomatic, 5-30 mm in size, located deep dermal or subcutaneous and covered with normal skin tissue [1]. Superficial lesions may be reddish or purplish due to hemorrhage [2]. Lesions are often defined at age 5-15. Female/ male ratio is 1.1/1 and the majority of cases reported in white race [3,4]. It has perforating, exophytic, multinodular, giant and bullous clinical types.6,7 Our case is clinically consistent with the perforating and exophytic type.
Physical examination shows mobile, stiff as cartilage or bone and sometimes painful tumor with smooth borders. Melanin pigment and calcification may be present up to 75-80% in the tumor. These tumors are generally solitar but should be 2-3% multiple and rarely familial [1,3,5]. Although multiple tumors were attempted to be related with muscular dystrophy, sarcoidosis, Rubistein Taybi, Turner syndrome, Goldenhar syndrome, Kabuki syndrome, Sotos syndrome; no relationship has founded with pilomatricoma. Cystic skin changes like pilomatricoma’s can also be seen in Gardner’s syndrome [6-10]. In our case, the tumor was solitar, and there was no clinical sign of other diseases.
In the pathogenesis it is recently suggested that 75% of the cases result from mutation in lymphoid enhancer factor-1 (LEF-1) located in the nucleus and beta-cate (CTNNB1) genes, despite the opinion that disorder impoves due to defect in proto-oncogene like bcl-2. Mutations in these genes may cause disorder by corrupting the DNA repair system in the cell [11,12].
Radiologically, plain radiographs can show non-specific calcifications. Tumor is visualised as solitary, well-circumscribed, subcutaneous mass by ultrasonography, CT and MRI. In the tumor, calcifications may be rare or widespread [13,14]. In our case, the diagnosis of teratoma was suggested because the tumor located midline and there was no calcification at CT. Normal values for alphafetoprotein chased us from this diagnosis. We think that radiological tests such as CT and plain graphies are not necessary if the clinical diagnosis is definite for pilomatricoma and excisional biopsy can be performed in this conditions. The definitive diagnosis is made by histopathologic examination of the mass obtained by excisional biopsy. Histopathological examination of pilomatricoma shows a capsule formed by connective tissue. Irregularly shaped islands of epithelial cells are localized in a cellular stroma. In these islands, there are basophilic and shadow cells without nuclear atypia. There are small, round, eosinophilic keratinization centers in the most of the tumors [15,16].
The treatment of choice and standard therapy for benign pilomatricoma is complete surgical excision. Occasionally, overlying skin will need to be excised secondary to tumor adherence to the dermis [17]. A wide excision with 1-2 cm of healthy tissue surrounding the mass must be performed. Morales and McGoey1 have advocated incision and curettement for cosmetic preservation in large tumors or for those in exposed areas [18].
The role of radiation is unknown owing to the small number of reported cases, but may help in locoregional control [19].
The incidence of recurrence is very low in patients with fully extraction. Pilomatricomas are benign lesions, but pleomorphism at basaloid cells, increased mitotic activity, local invasion or vascular invasion suggest pilomatrix carcinom. Pilomatrix carcinom is more common in older age and male gender. Local invasion and distant metastasis may be related with death [20].
In our patient, mass was removed under general anesthesia. No complication and recurrence developed during follow-up. Striking feature of this case is that pilomatricoma was a vegetative mass at midline. This is a rare presentation.
As a result, pilomatricoma is a rare, benign tumor in children. It could be misdiagnosed as other skin tumors. Because its clinical features are not well known, it has no specific signs or markers and it is seen in different regions in different forms. Mansur et al. [21] reported 25 patients with same presentation and 7 of them have clinically diagnosed as pilomatricoma. Our case was evaluated by several clinics, but could not diagnosed accurately. Definitive diagnosis is performed by biopsy, merely. Increasing knowledge of pediatricians about pilomatricoma, should prevent delay in diagnosis and unnecessary investigations; and make clinicians think this disorder more often in pre-diagnosis about tumors arising from the skin joints.
All author of this article are thankful to the patient’s family.