Journal of Cell Science & Therapy
Open Access
ISSN: 2157-7013
ISSN: 2157-7013
Review Article - (2015) Volume 6, Issue 5
The World Health Organization (WHO) estimates that the causative agent of tuberculosis (TB) currently infects one third of the global population and is responsible for about 2 million deaths among those infected annually. Current therapy for TB consists of multiple expensive antibiotics (Isoniazid, Rifampicin, Pyrazinamide, and Ethambutol) and is lengthy, up to six months for drug-susceptible, and nine months or more for drug-resistant variants of TB. Although current TB treatment eradicates M.tb from the host body it also causes severe hepatotoxicity and other adverse side effects, causing a large number of patients to withdraw early from therapy. Additionally, displaying a phenomenon called therapy-related immune impairment; TB-treated patients are vulnerable to reactivation or reinfection of the disease. Once patients start feeling better, they often withdraw from treatment, especially those that live in resource-limited environments. Treatment withdrawal is largely responsible for the generation of drug-resistant variants of M.tb, including multidrug-resistant (MDR) and extremely drug-resistant (XDR) forms of M.tb. Therefore, new treatment approaches that reduce treatment regimen lengths and limit hepatotoxicity and other side effects are urgently needed.
Keywords: Tuberculosis; Adverse effects of DOTS; Toxic effects of ATT
Tuberculosis is the deadliest infectious disease after HIV/AIDS, with latest WHO incidence reports claiming that in 2013, 9 million people fell ill with TB and 1.5 - 2 million dying from the disease worldwide. One third of the global population is latently infected with M.tb, which represents a huge pool of hosts at risk of M.tb reactivation [1]. Conditions such as immune impairment and HIV co-infection further increase risk of TB reactivation [2]. HIV co-infection increases the risk of TB reactivation substantially. In the absence of HIV coinfection only 5-10 % of latently infected individuals develop TB in their life time, compared to 30 % in HIV positive individuals [3].
Bacillus Calmette-Guérin (BCG) is the only TB vaccine presently available. It has been widely used throughout the world since its development in 1921, and an estimated three billion people have received it. It’s efficacy against adult pulmonary TB varies dramatically between 0-80% in different populations, depending on ethnicity and geographical location [4]. Nevertheless, BCG is very effective against disseminated and meningeal TB in young children [5].
These findings suggest that host protective immune responses induced by BCG wane over a period during the life-time of a vaccinated individual. Although a decline in the pool of memory T cells is a natural process, restoring memory responses to BCG might be challenging, it may be possible to alter the magnitude of the memory cells by conjunctively using immunomodulators. And while many new vaccine candidates have shown promise in the animal model, their translation to viable and clinically efficacious vaccines remains elusive. It is well established that CD4+ helper T cells play a pivotal role in host resistance to infection [6]. Studies have revealed that mutations in the receptor for IFN-γ and any other factors that impair IFN-γ production increase TB susceptibility [7]. Therefore, it is evident that type 1 helper T (Th1) cells contribute to host protection from M.tb infection [8]. Therefore, eliciting Th1 responses against M.tb holds significant promise for developing vaccines and immune therapies for TB [9].
Given that TB is an ancient scourge and anti-TB drugs have been used for decades, strains that are resistant to at least one first-line anti-TB drug have now been documented in every country surveyed. Multidrugresistant tuberculosis (MDR-TB) is classified as a form of TB caused by M.tb that does not respond to, at least, isoniazid and rifampicin, the two most successful, first-line drugs. TB caused by MDR strains fails to respond to conventional therapy, though it can be completely cured by using an appropriate combination of second-line drugs. However, there are significant drawbacks to the treatment such as an even lengthier regimen (up to two years of treatment), limited second-line treatment options, more costly, and substantially severer adverse side effects. Consequently, noncompliance to MDR-TB treatment can in some cases lead to development of Extensively drug-resistant (XDR)-TB, which is classified as a form of MDR-TB that acquires resistance even to the most effective second-line anti-TB drugs. About 480 000 people developed MDR-TB in the world in 2013. More than half of these cases were in India, China and the Russian Federation. It is estimated that about 9.0% of MDR-TB cases had XDR-TB.
Due to use of multiple expensive antibiotics, each with substantial toxicity, a significant number of TB patients halt treatment mid course. This non-compliance with the prescribed treatment regimen has been linked with the emergence and evolution of drug-resistant forms of TB [10,11]. Across the globe, virtually every region, irrespective of its socioeconomic conditions, is now under threat from drug-resistant TB [12,13]. And while now for almost a decade the discovery of new generation antibiotics has been trailing sluggishly behind in the race against drug-resistant TB, the emergence of a Totally Drug Resistant (TDR) form of TB has made matters significantly worse [14-16].
In 2006 the WHO recommended “Stop TB strategy” with its objectives of reducing global burden of TB by 2015 and, by 2050 eliminating it as a global health problem. At this moment however, improved data due to increased surveillance shows an increase in incidence compared to previous years. Thus, acceleration in current rates of decline are needed to meet all targets, making its achievement an uphill battle. The Stop TB strategy is executed as a set of Millennium Development Goals, of which, two key components are to pursue high-quality DOTS expansion and to address TB-HIV and Multi drug resistant (MDR)-TB. Role of inefficiently executed DOTS has been debated in generation of MDR, XDR and TDR strains, as their emergence and incidence are reportedly in locations with largely poor TB control strategies.
In this review, we assimilate the current understanding of anti-TB drug-induced side effects of first- and second-line drugs. Many of these side effects involve perturbation of the immune system, and it may be beneficial to look for adjuvants and/or immunomodulators that can be co-administered to reduce at least the harmful long-term effects of TB treatment regimens.
The current internationally Accepted Date: therapy by Directly Observed Treatment, Short-Course (DOTS) for drug-susceptible TB consists of multiple expensive antibiotics and is lengthy [17,18]. Adherence and compliance are critical for optimal efficacy of these drug regimens. The regimen chosen for treatment of TB is largely based on two indicators – first, whether the patient has previously been treated for tuberculosis and second, the drug-susceptibility status of infecting bacilli. Figure 1 outlines the WHO recommended first and second-line drugs and their doses for treatment of TB DOTS strategy for treatment of drugsusceptible TB involves administration of Isoniazid (INH), Rifampicin (RIF), Pyrazinamide (PZA), and Ethambutol (E) during the first two months in the active phase of the disease, followed by an additional four months of treatment with INH and Rifampicin. Much longer and more extensive treatment in the form of combinatorial therapy is required for curing drug-resistant forms of TB [17-19].
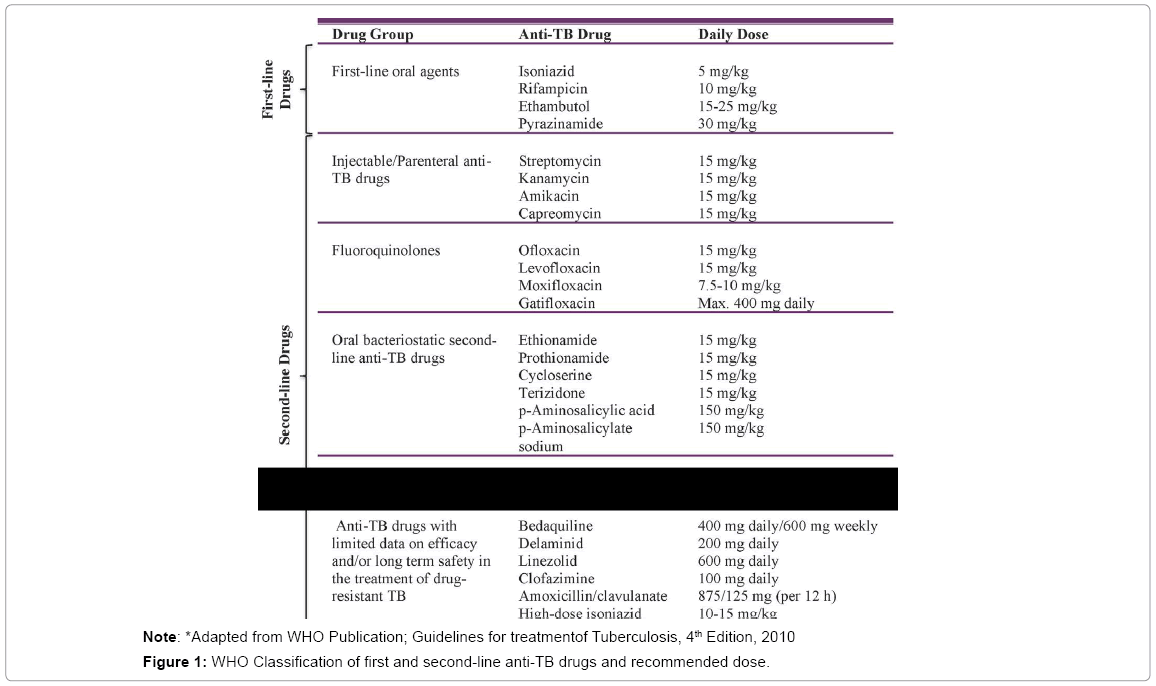
Figure 1: WHO Classification of first and second-line anti-TB drugs and recommended dose.
Access to various drug-susceptibility diagnostic capabilities forms the basis of correct and efficacious treatment of MDR-TB. At minimum drug-susceptibility testing (DST) is critical for improved patient outcomes. This is because resistance to drugs varies among strains and treatment regimes are most effective when designed based on DST results. However, in most resource poor settings, DST is either absent or limited to INH and RIF testing. In such situations, WHO recommends a ‘standardized regimen’ based on the geographies drug-resistance surveillance. The standardized regimen uses four effective second-line anti-TB drugs (oral and injectable) plus pyrazinamide for the entire duration of treatment, which is a minimum of 8 months. Treatment of MDR-TB includes drugs, which display even more severe side effects when compared to the first-line drugs.
M.tb-infected individuals mount anti-tubercular immune responses as evidenced by delayed-type hypersensitivity (DTH) against purified protein derivative (PPD), and induction of T cells secreting IFN-γ. However, these immune responses are not sufficient to eradicate the harbored organisms in a primary infection because M.tb mobilizes multiple immune evasion mechanisms even before the adaptive immune response is generated. Therefore, it is expected that upon effective treatment of TB with antibiotics, individuals should retain host protective immune memory responses. However, epidemiological data indicate that individuals treated for TB have even a higher risk for re-infection or reactivation of M.tb [20-23]. The relative contribution of TB re-infection and relapse to the overall incidence and the risk factors associated with recurrent TB is not well understood. A recently published work has shown that treatment with INH, one of the antibiotics used in DOTS, exhibits severe hepatotoxicity and also induces apoptosis in activated T cells [24]. Considering T cells play a central role in host protective immune responses against M.tb and other organisms [21], it is likely that their elimination caused by treatment with INH is responsible for making the individual vulnerable to re-infection and or reactivation of the disease once the treatment is withdrawn [21]. Thus, while DOTS therapy for TB is very effective in controlling the disease, it is also associated with a significant number of adverse effects (Figure 2).
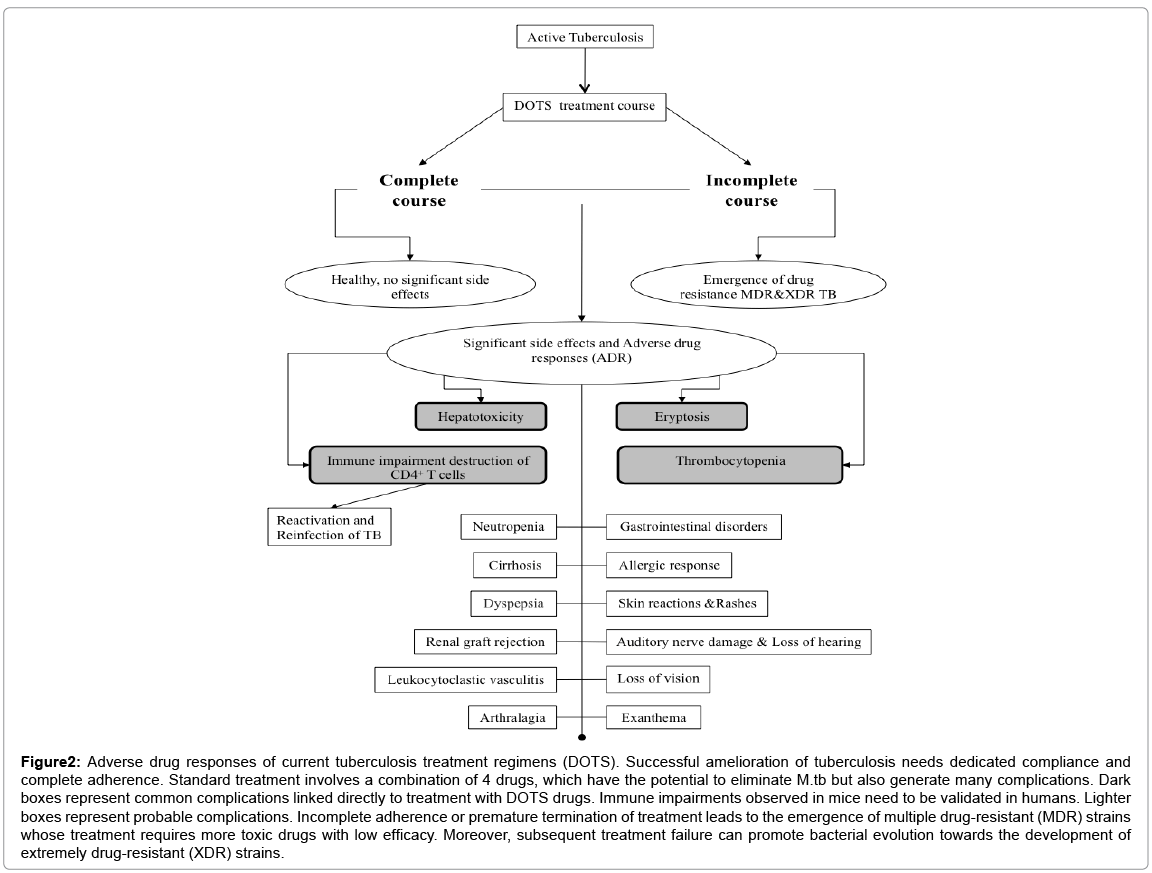
Figure 2: Adverse drug responses of current tuberculosis treatment regimens (DOTS). Successful amelioration of tuberculosis needs dedicated compliance and complete adherence. Standard treatment involves a combination of 4 drugs, which have the potential to eliminate M.tb but also generate many complications. Dark boxes represent common complications linked directly to treatment with DOTS drugs. Immune impairments observed in mice need to be validated in humans. Lighter boxes represent probable complications. Incomplete adherence or premature termination of treatment leads to the emergence of multiple drug-resistant (MDR) strains whose treatment requires more toxic drugs with low efficacy. Moreover, subsequent treatment failure can promote bacterial evolution towards the development of extremely drug-resistant (XDR) strains.
Hepatotoxicity
Hepatotoxicity is the most serious complication arising from the first line of TB treatment. Isoniazid, rifampicin and pyrazinamide are potentially hepatotoxic drugs [25]. The probability to developing hepatotoxicity varies between 2% to 28% in all patients, and taking into consideration their comparative risk, associated with substantial morbidity and mortality. The liver metabolizes these drugs and hepatotoxicity is presumed by a 3- to 5-fold increase in transaminase levels above the upper limit of the normal range [26]. Clinically, it is assessed by measuring serum levels of three enzymes, aspartate amino transferase (AST; normal range 7-40 IU), alanine aminotransferase (ALT; normal range 5-50 IU) and bilirubin (normal range in adult 0.3 to 1.9 mg/dL). Maximum transaminase levels are observed during the first 4 months of treatment (72% of patients) [27]. Clinical biochemistry profiling has shown that pathological transaminase levels were comparable for different patients. Mild ALT elevations may evoke non-progressive liver injury whereas elevated AST levels may lead to mitochondrial oxidative damage [25].
Significantly, about 0.5% patients show hepatotoxicity to INH mono-therapy. The percentage was higher for combination therapies. It is not INH levels in the serum that is toxic but rather its metabolites, especially hydrazine. N-acetyltransferase 2 (NAT-2) in humans acetylates INH to form acetylisoniazid, which further undergoes hydrolysis to generate acetylhydrazine. Polymorphic variants of NAT-2 redirect some INH towards an alternative oxidative pathway via P450 to generate hydrazine [28]. Acetylhydrazine and hydrazine participate in complex reactions to produce free radicals that generate an environment conducive to oxidative stress. INH metabolites bind covalently with cellular macromolecules, which clinically manifests primarily as hepatocellular steatosis and necrosis wherein lipid vacuoles and mitochondrial swelling are found in periportal and midzonal hepatocytes.
Many children (41%) receiving prophylactic treatment of TB for more than 4 months show elevated Transaminase levels [27]. This is even more frequent in children younger than nine years of age (62%) when compared to those between 10-18 years of age (28%). Generally, hepatotoxicity shows geographical variations. Asian populations, especially Indian patients show the highest rates, where as sub-Saharan populations show minimal rates, although this may be due to the lack of all the routine testing and adequate region surveillance.
RIF also interacts with antiretroviral drugs to influence their plasma levels and consequently produces hepatotoxicity [29]. RIF enhances hepatotoxicity of INH by promoting the generation of the metabolites acetylhydrazine and hydrazine. It also competes with bilirubin for clearance at sinusoidal membranes in a dose-dependent manner, which leads to hepatic cell injury, mild asymptomatic unconjugated hyperbilirubinemia or jaundice without hepatocellular changes, or centrilobular necrosis, possibly associated with cholestasis. Histopathological findings from DOTS-treated patients show a range of pathologies from spotty to diffuse necrosis with more-or-less complete cholestasis [29].
PZA is presumed as a serious contributor to hepatotoxicity and shows other complications such as rashes. Molecular mechanisms responsible for hepatotoxicity due to PZA are still not clear. Pyrazinoic acid (PA) and 5-Hydroxy Pyrazinoic acid (5-OH-PA) are the main metabolites responsible for PZA-mediated hepatotoxicity. PA is converted by xanthine oxidase hydrolysis to 5-OH-PA. Urine samples from patients undergoing TB treatment showed a correlation between an increase in PA/PZA drug ratio and 5-OH-PA/PZA metabolite ratio and hepatotoxic severity. Oral administration of the amidase inhibitor bis-para-nitrophenylphosphate (BNPP) restores PZA-mediated but not PA-mediated toxicity, thus firmly establishing PA as the main culprit of hepatotoxicity [30]. It is well known that TB patients taking both PZA and E show a 4-fold increase in transaminase levels, whereas E alone causes no significant increase in transaminase levels.
Erptosis and thrombocytopenia
Thrombocytopenia is defined as a condition when thrombocyte counts are lower than 150,000/mm3. Although thrombocytopenia is rare, it is a life threatening condition. Previous studies [31] have firmly established a role of drugs employed during DOTS in thrombocytopenia. INH and RIF are capable of causing thrombocytopenia either together or individually. RIF plays a prominent role in anti-TB-associated thrombocytopenia where it is known as drug-induced immune thrombocytopenia (DIIT). A characteristic feature of this clinical disorder is the presence of drug-dependent antibodies (DDAbs), which have the unique ability to bind antigen only in the presence of the respective drugs. RIF binds to glycoprotein (GP) Ib-IX to form a complex antigen epitope, to which DDAbs bind non-covalently on the platelet surface, which eventually results in platelet destruction [32]. A drop in the platelet level below 20,000 (platelets/pL) may cause spontaneous bleeding and ecchymosis. The precise mechanism of INH-induced thrombocytopenia is not well defined, but may acutely cause leukocytosis, and may induce chronic anemia (hemolytic, sideroblastic, aplastic, or megaloblastic), agranulocytosis, eosinophilia; disseminated intravascular coagulation and lymphadenopathy due to hypersensitivity reactions has also been reported. It exacerbates RIF-induced complications that might result in development of Antituberculosis drug induced hepatotoxicity (ADTH).
Other side effects of DOTS
Long-term intake of INH can cause peripheral neuritis and CNS effects, as well as sideroblastic anemia. Peripheral neuritis is linked to pyridoxine (vitamin B6) depletion, and is the reason why pyridoxine supplementation is prescribed along with standard INH dosing for safety reasons. INH is one of drugs that can cause DILE (drug-induced lupus erythematosus) [33]. Studies have provided strong evidence for a link between INH treatment and DILE, as these conditions disappears upon drug discontinuation. INH induces anti-nuclear antibodies (ANA) in 25% of patients and DILE in 1% of patients [34]. Some studies have also implicated INH in pleural effusion. Delayed emergence of effusion has been reported after starting anti-TB treatment. This clinical scenario is presumed due to a paradoxical response. The exact mechanism by which INH induces pleural effusion is yet to be elucidated. Some reports have provided evidence for an “immunological rebound model” in which excessive antigen load produced by bacterial lysis causes ‘revved up cell-mediated immunity [35]. A non-specific increase of ANA levels in serum and resolution of pleural effusion upon INH discontinuation is consistent with DILE. As this condition was partially alleviated with anti-inflammatory agents such as corticosteroids, these side effects were consistent with inflammation.
RIF, an integral component of DOTS therapy for normal M.tb as well as drug-resistant M.tb strains, is highly effective. However, many complications and adverse drug responses restrict its use. This adverse drug response is manifested as segmental necrotizing glomerulonephritis, acute renal failure [36,37] and hemolytic anemia [38]. Additionally, RIF can also cause the life-threatening side effect of angioedema [39]. In patients undergoing transplantation procedures, calcineurin concentrations in serum are known to reduce due to unfruitful crosstalk between RIF and immune suppressive drugs [40,41]. Moreover, in those receiving TB treatment, the possibility of renal graft rejection may is reportedly increased [42].
It has also been reported that RIF stimulates suicidal eryptosis or erythrocyte death [43]. Rifampicin stimulates Ca2+ permeable cation channels, which facilitates Ca2+ entry into RBC from extracellular spaces. Increases in cytosolic Ca2+ levels induce hyperpolarization of cells by release of K+ via K+ channels. Hyperpolarization of cells further induces Cl- release. Exodus of K+ and Cl- ions promote water to be leached by osmosis, which ultimately leads to characteristic cell shrinkage and scrambling. Cell scrambling abolishes asymmetry of phosphatidylserine (PS). PS translocates to the erythrocyte surface and contributes along with other factors to increase ceramide production. Ceramide increases the Ca2+-sensitivity of cell membrane scrambling and thus stimulates eryptosis. PS exposure in turn causes erythrocytes to bind with PS receptors on phagocytic cells [44]. Rifampicin-mediated ceramide production has toxic effects on many cell types. Ceramide induces apoptosis and may contribute to the patho physiology of several clinical syndromes such as diabetes, Parkinson disease, Alzheimer disease, and cardiovascular disease.
As nomenclature goes, MDR-TB is defined as resistance to at least two crucial first-line drugs INH and RIF. XDR TB strain displays resistance to INH and RIF, plus any fluoroquinolone and at least one of three injectable second-line drugs (i.e., amikacin, kanamycin, or capreomycin). Each group of second line drugs (e.g. aminoglycosides, fluoroquinolones etc.) present with similar adverse effects. Compared to the basic DOTS regimen for drug-susceptible TB, drugs for treatment of MDR-TB are generally lesser effective and problematically toxic as well as more expensive. By and large, while severity of adverse reactions observed varies greatly in patient population, there is little data on their direct role in immune system perturbation.
Aminoglycosides
Streptomycin, kanamycin and amikacin constitute the group of second-line drugs that are parenterally administered. The most severe adverse reaction to aminoglycosides is ototoxicity caused by damage to cranial nerve VIII. Concomitant symptoms of vertigo, ataxia, and nystagmus and cochlear damage that can lead to hearing loss have been reported [45]. Risk of toxicity increases with age, duration of treatment, and total accumulated dose.
Aminoglycosides can also produce severe renal toxic effects due to their accumulation in the renal tubules. Though these effects have been reported to be more prevalent in elderly individuals and patients with history of kidney disease. Nephrotoxicity presents ashypouresis, urinary casts, proteinuria, and decreased creatinine clearance, and consequently increased serum levels of urea and creatinine. Comparatively, nephrotoxicity seems more common in patients onamikacin(3.4-8.7%) than in those on streptomycin (2%) [46].
Fluoroquinolones
The most effective fluoroquinolones against M.tb in order of efficacy are moxifloxacin and gatifloxacin, followed by levofloxacin, ofloxacin, and ciprofloxacin [47]. Adverse reactions to this group of drugs are very varied and range in severity as well. Gastrointestinal side effects are most common (3–17%) and include symptoms like nausea, vomiting, aerophagy, anorexia, abdominal discomfort, and diarrhea. Relatively rare (less than 10%) side effects can involve the nervous system (dizziness, headache, insomnia, tremors etc.), erythema, pruritus, and skin rash. Use of this group of drugs is restricted in children, as arthropathy and cartilage erosion have been reported in young animals treated with fluoroquinolones [48].
Among the adverse reactions to second-line TB drugs, neurological symptoms are among the most severe side effects. Cycloserine/ terizidone not only display neurological side effects like headache, vertigo, dysarthria, convulsions, and memory deficit) but also present psychiatric adverse effects and increase risk of suicide. These are more common when daily dose is higher than 500 mg or when cycloserine/ terizidone is administered in conjunction with other neurotoxic drugs, such as INH and ethionamide. The administration of pyridoxine can aid in preventing the neurotoxic effects. Ethionamide is structurally similar to INH but varies in its mode of action on M.tb. Ethionamide inhibits the activity of the inhA gene as compared to INH which is a pro-drug that releases free radicals when activated by the M.tb enzyme KatG. Both drugs ultimately inhibit protein synthesis and preventing mycolic acid biosynthesis [49]. Given the similar structure ethionamide and INH also show similar side effects. Hepatotoxicity (4.3%) and neuro toxicity (1-2%) are the two most commonly reported side effects.
Mechanisms of action of other drugs such as capreomycin and PAS are not thoroughly elucidated, nor are their exclusive adverse reactions precisely correlated in patients being treated with them.
This is most likely because both these drugs are always administered concomitantly with other anti-TB drugs and it is not well characterized whether the side effects are a result of cross-reactions among drugs or a direct effect of the drug itself. The polypeptide antibiotic capreomycin is structurally different from aminoglycosides, but displays similar antibacterial activity as well as side effects. The mechanism of action of this drug has yet to be elucidated convincingly, though it is believed that the drug somehow interferes with bacterial protein synthesis. Common side effects include nephrotoxicity (20-25%), renal tubular damage, proteinuria and urticarial. The severe side effect of ototoxicity is also known to occur but only very rarely. In patients being treated with PAS gastrointestinal side effects and hypothyroidism are those reported most. Although reported in significantly lesser cases, more severe side effects of PAS also include hepatitis (0.3-0.5%) and hemolytic anemia [50].
The global use of DOTS was initiated during the last decade of the 20th century. Around 2-3 billion people have been treated with it to combat TB. Although effective, it is associated with some serious side effects. Adverse outcomes vary from drug-induced hepatotoxicity to thrombocytopenia and immune impairment. Mouse models have shown that DOTS is associated with immune dysfunction, which subsequently provides the opportunity to the pathogen to reactivate or recurrence [24]. Incomplete adherence to the therapeutic regimen and premature treatment termination not only show clinical unresponsiveness but also lead to the emergence of drug-resistant strains. Unethical practices in many parts of world such as the lack of drug susceptibility testing prior to DOTS are also responsible for the emergence of drug-resistant MDR and many cases of XDR. Further studies in humans have validated immunological impairment associated with DOTS [20-22]. Treatment of MDR-TB further complicates issues of patients compliance as most second-line drugs are lesser effective and display more toxicity than drugs that constitute the basic DOTS regimen. Because antibiotics are the backbone of TB treatment, complementing DOTS with an adjuvant or immunomodulator might be able to reduce or avoid the harmful long-term effects associated with TB treatment regimens.
We searched articles from Pubmed and Google with combinations of the keywords “Tuberculosis”, “Adverse effects of DOTS therapy”,“Toxic effects of ATT” and “adverse effects of second-line drugs”. We also identified relevant articles by the authors’ names and from review articles.