Journal of Cell Science & Therapy
Open Access
ISSN: 2157-7013
ISSN: 2157-7013
Case Report - (2015) Volume 6, Issue 5
Introduction: Carcinomas of the colon and rectum are the third most common cancer entity in the world and bear a high risk of synchronous (25%) or metachronous (50%) hepatic tumor seeding. For therapeutic decisions the differential diagnosis between benign and malignant hepatic lesions in the computer tomography scan is of major importance. We herein discuss congenital hepatic cysts derived from the primitive foregut as potential differential diagnosis for hepatic metastases from a colorectal primary tumor.
Case presentation: A caucasian, 56-year old female patient with the initial diagnosis of an adenocarcinoma of the rectum had initially been treated by an anterior rectum resection and hemihepatectomy due to synchronous hepatic metastases (pT3 pN1(2/13), G2, pM1(HEP), L1, V0, pR0) in a curative intention. The follow-up staging after 2 years showed recurrent liver metastases. A local resection of the hepatic foci was performed. One of three lesions was classified as a classical ventral foregut derived bronchogenic cyst located subcapsularly in the liver. A follow-up resection of pulmonary metastases was performed 13 months later. The patient is still alive and healthy 68 months after the primary operation.
Conclusions: For the diagnosis and treatment of hepatic metastases of colorectal carcinomas it is very useful to know potential differential diagnoses in radiographic imaging. Foregut derived cysts can be histologically subclassified into Ciliated Hepatic Foregut Cysts and Bronchogenic Cysts. While Ciliated Hepatic Foregut Cysts are known to be located in the liver, we present the rare case of a Bronchogenic Cyst, which was located in the liver parenchyma.
Keywords: Bronchogenic cyst; Colorectal carcinoma; Hepatic metastases; Ciliated hepatic foregut cyst
BC: Bronchogenic cyst; CEA: Carcinoembryonic antigen; CHFC: Ciliated Hepatic Foregut cyst; CT: Computer Tomography; FOLFIRI: Therapy Scheme for Adjuvant Chemotherapy of Colorectal Cancer, Consisting of FOL=Folinic acid, F=Fluorouracil, IRI=Irinotecan; FOLFOX: Therapy scheme for adjuvant chemotherapy of colorectal cancer, consisting of FOL=Folinic acid, F=Fluorouracil, OX=Oxaliplatin; TNM: TNM classification of malignant tumours; TTF-1: Thyroid transcription factor; 1UICC; Union international contre le cancer
Colorectal adenocarcinoma
Colorectal carcinoma is the third most common malignant disease worldwide [1]. Based on the primary depth of tumor invasion, the occurence of loco-regional lymphnode metastases and of distant tumor metastasis colorectal adenocarcinomas can be graduated according to TNM- or Union internationale contre le cancer (UICC-) classification system. The five-year-survival rate decreases with higher tumor classification (Table 1).
| Tumor stage (Union internationale contre le cancer – UICC) | Five-year-survival |
|---|---|
| Stage I (T1, T2, N0, M0) | 97.10% |
| Stage IIA (T3, N0, M0) | 87.50% |
| Stage IIB (T4, N0, M0) | 71.50% |
| Stage IIIA (T1 / T2, N1, M0) | 87.70% |
| Stage IIIB (T1 / T2, N2, M0) | 75% |
| Stage IIIB (T3, N1, M0) | 68.70% |
| Stage IIIC (T3, N2, M0) | 47.30% |
| Stage IIIC (T4, N1, M0) | 50.50% |
| Stage IIIC (T4, N2, M0) | 27.10% |
| Stage IV (T1-4, N1-2, M) | 5 – 9% |
Table 1: 5-year-survival in relation to cancer-stadium (UICC) [2,3].
The liver is the most common site for metastatic spread. In approximately 25% of the cases metastases can be found synchronously [1], in nearly 50% liver metastases appear metachronously after primary tumor resection [4]. Despite pulmonary and hepatic spreading a radical surgical resection of the hepatic metastases can be performed in a curative manner in 10-25% of the patients [5]. Surgical treatment of liver metastases of colorectal carcinomas is complex and should be discussed in a multidisciplinary team including surgeons, oncologists and interventional radiologists. Surgical resection of hepatic metastases should be performed whenever a curative result is possible. This is based on recent studies, where patients with R0 resected liver metastases reveal a 5-year-survival of nearly 40% (versus 5% with irresectable metastases) and a 10-year-survival of 25% [4,6-8].
On computer tomography (CT) imaging hepatic metastases of colorectal carcinomas show a contrast enhancement, which can be asymmetric and extremely variable. Usually metastases are silhouetted against the surrounding liver parenchyma as hypovascularized and hypodense lesions. While healthy liver parenchyma is mainly perfused by the portal vein, liver metastases are contrasted during the arterial perfusion phase during the CT-scan. This fact leads to a minor contrast enhancement and hypodensity in the portal vein phase with a peripheral enhancement in contrast to the surrounding parenchyma. Furthermore liver metastases of colorectal carcinomas can show cystic or calcified degeneration [5] (Table 2).
| Differential diagnosis of hepatic lesions | CT-radiographic finding and contrast enhancement |
|---|---|
| Metastases | Hypodense lesion, asymmetrical contrast enhancement in arterial phase |
| Hepatocellular carcinoma | Hypervascular lesion in arterial phase, whereby the lesion shows a contrast washout in the portal venous phase |
| Cholangiocellular carcinoma | Delayed contrast enhancement |
| Lymphoma | Primary hepatic lymphoma: Either low density lesion in both contrast-enhanced and non-contrast-enhanced CT-scan or bearing a contrast-enhancing rim Secondary hepatic lymphoma: Blood vessel floating sign and enhancement |
| Subcentimeter focal lesions | Difficult to charakterize by radiographics, whereas over 80 % are benign |
| Haemangioma | Arterial hyper-enhancement in all phases or globular, peripheral or discontinuous enhancement in portal venous phase |
| Focal steatosis | Nodular appearance, hypodense lesion due to fatty infiltration |
| Cysts | Hypodense lesions with no contrast enhancement |
| Focal nodular hyperplasia | Iso- / hypodens lesion with contrast enhancement in the arterial phase, persistent hypervascularisation in portal venous phase and central scar |
| Hepatocellular adenoma | Hypodens lesion with hyperdens intersets, hyperdens and often inhomogen in the arterial phase, in portal venous phase iso- / hypodens |
| Hepatic abscess | Depending mainly on the cause. Pyogenic abscesses are well-defined hypodense lesions with rim enhancement |
| Biliar hamartoma | Contrast-enhancement of the stromal components of the tumor |
| Haemangioendothelioma | Hypodense mass in unenhanced CT-scan, resemble contrast-enhancement of haemangioma |
Table 2: Differential diagnosis of liver metastases originating from colorectal carcinomas in CT-scan potential intrahepatic lesions [5,9-14].
Cysts derived from the primitive foregut
While the tracheobronchial system derives from the primitive ventral portion of the foregut [15] the intestine and the liver originate from the primitive caudal foregut.
Bronchogenic cysts (BC) are malformations developing during the genesis of the respiratory tract. The location of BCs significantly depends on the embryological stage during which the abnormality occurs. The most common locations of BCs are supradiaphragmatic in the mediastinum and inside the lung parenchyma [15]. 60 to 90% of the cysts are mediastinal, arising in the early embryological stage, whereas abnormalities in late stages lead to a more peripheral cyst location, i.e. in the lung parenchyma [15-18]. Besides these typical and well-known locations for BCs, review of literature reveals some other less common locations: BCs can be atypically located in the neck [19], in the skin [20] and in the pericardium [21,22]. Subdiaphragmatic locations are extremely rare: In some cases BCs are discovered in the retroperitoneum [22] and in the abdominal cavity [17]. Two different explanations for this abnormal subdiaphragmatic location of a BC can be found in the current literature: (1) The malformation loses the connection to the tracheobronchial tree and migrates through the pericardioperitoneal canal from the thoracic cavity into the abdomen before the fusion of the pleuroperitoneal membranes takes place. (2) alternatively a miss-differentiation of the abdominal foregut could explain this rare localization of a BC [22,23].
Symptoms and complications of BCs are dyspnoe, recurrent airway infections, bleedings, risk of malignant transformation, displacement and compression of surrounding tissue. In most cases BCs are asymptomatic and thus are diagnosed incidentally [24].
Histologically the wall of BCs consists of ciliated respiratory epithelium, i.e. pseudostratified ciliated columnar cells, cartilage, elastic fibers, bronchial gland cells and smooth muscle bundles and is either filled with mucus, fluid or air, if it is connected to the tracheobronchial system [15,18,25]. Normally in CT-scans the bronchogenic cyst appears as a solitary mass with a thin cyst wall and a density of -10 to +10 hounsfield units similar to that of water. Protein-rich fluid inside the cyst or calcifications increase the density. The cyst shows no contrast enhancement [15,26,27].
In contrast to BCs another kind of ciliated foregut cysts can appear in the liver. These ciliated hepatic foregut cysts (CHFC) are benign congenital unilocular malformations derived from the primitive foregut. Most commonly they can be detected in the medial segment of the left hepatic lobe (segment 4). In close relation to BCs, CHFCs consist of four layers: ciliated pseudostratified columnar epithelium with admixed mucous cells, subepithelial connective tissue, smooth muscle cells, which are arranged in one to three layers, and a surrounding fibrous capsule. The cysts themselves are filled with mucus. Either budding from the hepatic diverticulum or from the nearby enteric foregut seems to be the mechanism of CHFC development [27].
Histologically BCs and CHFCs show a bunch of similarities: The epithelium of CHFC is similar to bronchial epithelium, but lacks cartilage and respiratory glands. Consequently these two characteristics together with ciliated columnar epithelium define a BC, whereas the presence of two or three layers of smooth muscle cells is typical for enteric differentiation and defines a CHFC [27,28]. Additionally, bronchus-derived tissue shows no positivity for carcinoembryonic antigen (CEA) in immunohistochemistry, which is the case for CHFC [29].
We present the case of a caucasian, 56-year old female patient with the first diagnosis of a rectal adenocarcinoma 7 centimeters distant from the anus two years prior to the finding of a bronchogenic cyst inside the liver parenchyma. The initial staging CT-scan (Figure 1) showed synchronous hepatic metastases in both left (segment two and three) and right hepatic lobes (segment seven (8.5 cm), five, six and eight). After neoadjuvant chemotherapy surgical resection of the rectal carcinoma was performed by an anterior rectum resection and two hepatic metastases in segment two and three were resected. Because the main metastatic mass was located in the right hepatic lobe, embolization of the right portal vein was accomplished by interventional radiologists to induce hypertrophy of the left lobe. Six weeks later a right hemihepatectomy was performed. The pathological examination of the specimen led to the initial tumor stage pT3 pN1(2/13), G2, pM1(HEP), L1, V0, pR0 (local and hepatic). The patient was treated with an adjuvant chemotherapy according to the FOLFOX scheme. On follow-up two years after the initial operation imaging studies revealed new suspicious masses in segment one and four (Figure 1). Furthermore pulmonary metastases were detected which led to a conversion of the chemotherapy to FOLFIRI + Erbitux. According to a radical surgical approach surgical resection of liver segments one and remaining four was performed, whereas segment two and three were tumorfree in intraoperative ultrasonic examination. During intraoperative ultrasound examination one further suspicious lesion between the left and middle hepatic vein was explored and resected. Metastases of a colorectal adenocarcinoma could be pathological confirmed in the remaining segment one and four, whereas the definite pathologic diagnosis of the mass between the left and the middle hepatic vein was a ciliated foregut cyst. In immunohistochemical staining the tissue of the cystic lesion was negative for CEA and the gland cells showed high positivity for thyroid transcription factor 1 (TTF-1), thus proofing the origin from tracheobronchial tissue (Figure 2).
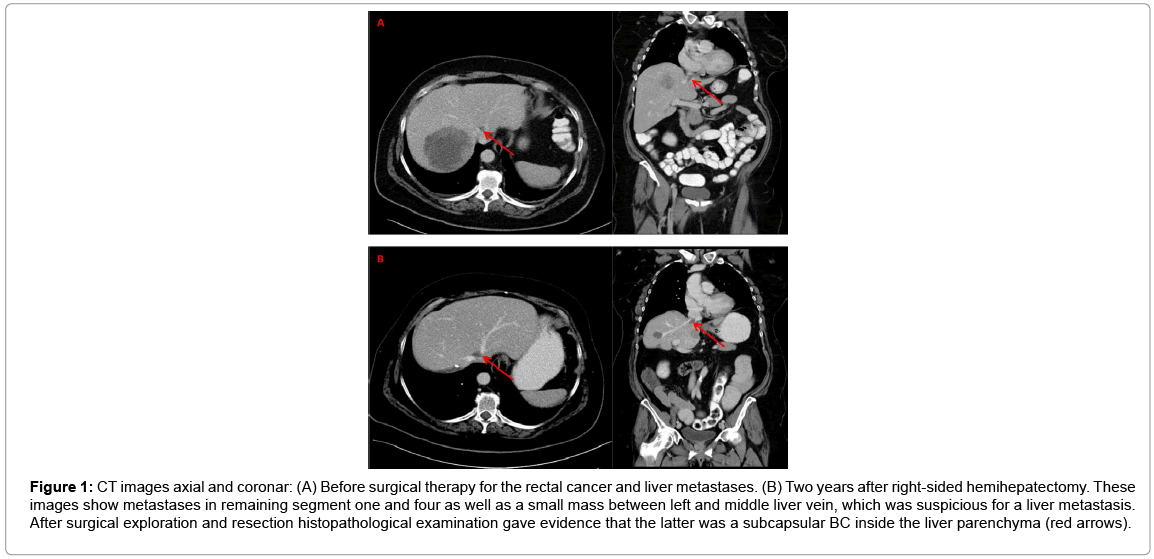
Figure 1: CT images axial and coronar: (A) Before surgical therapy for the rectal cancer and liver metastases. (B) Two years after right-sided hemihepatectomy. These images show metastases in remaining segment one and four as well as a small mass between left and middle liver vein, which was suspicious for a liver metastasis. After surgical exploration and resection histopathological examination gave evidence that the latter was a subcapsular BC inside the liver parenchyma (red arrows).
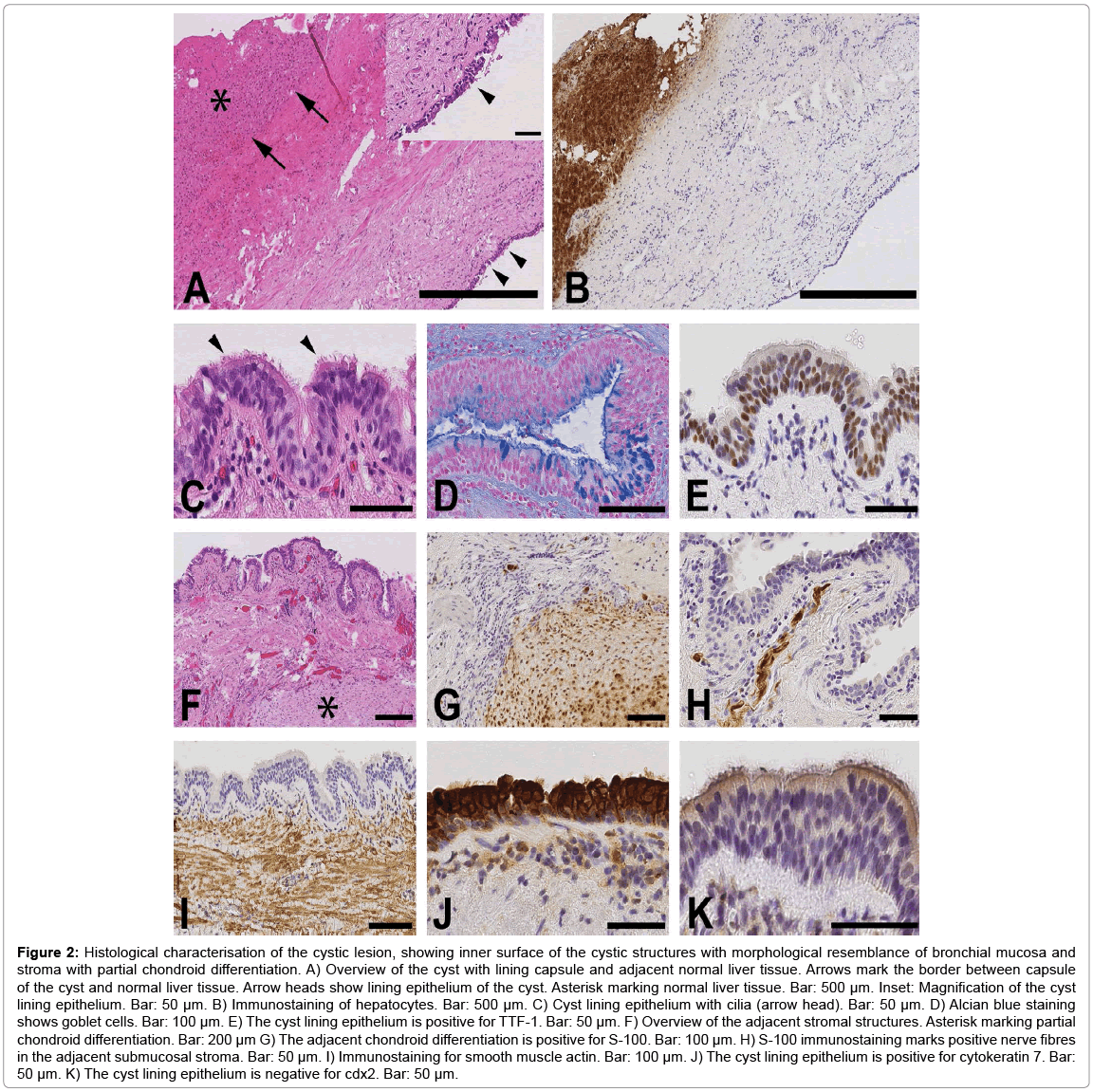
Figure 2: Histological characterisation of the cystic lesion, showing inner surface of the cystic structures with morphological resemblance of bronchial mucosa and stroma with partial chondroid differentiation. A) Overview of the cyst with lining capsule and adjacent normal liver tissue. Arrows mark the border between capsule of the cyst and normal liver tissue. Arrow heads show lining epithelium of the cyst. Asterisk marking normal liver tissue. Bar: 500 μm. Inset: Magnification of the cyst lining epithelium. Bar: 50 μm. B) Immunostaining of hepatocytes. Bar: 500 μm. C) Cyst lining epithelium with cilia (arrow head). Bar: 50 μm. D) Alcian blue staining shows goblet cells. Bar: 100 μm. E) The cyst lining epithelium is positive for TTF-1. Bar: 50 μm. F) Overview of the adjacent stromal structures. Asterisk marking partial chondroid differentiation. Bar: 200 μm G) The adjacent chondroid differentiation is positive for S-100. Bar: 100 μm. H) S-100 immunostaining marks positive nerve fibres in the adjacent submucosal stroma. Bar: 50 μm. I) Immunostaining for smooth muscle actin. Bar: 100 μm. J) The cyst lining epithelium is positive for cytokeratin 7. Bar: 50 μm. K) The cyst lining epithelium is negative for cdx2. Bar: 50 μm.
In long-term follow up the liver showed no new lesions. The solitary pulmonary metastasis of the right upper lobe showed incomplete remission under chemotherapy and was thus resected by video-assisted thoracoscopic surgery 38 months after initial resection of the primary cancer. The patient is alive and healthy, 68 months after first diagnosis of metastasized rectal carcinoma.
Rectal cancer is one of the most common malignant diseases. Approximately 70% of the patients with advanced colorectal cancer will develop liver metastases. Among these patients, almost 25% have metastatic spreading exclusively into the liver. Current literature indicates that resection of metastases should be performed whenever possible, as it dramatically improves five-year-survival [3].
In our case a progressed rectal carcinoma with multiple hepatic metastases and local lymphnode infiltration was diagnosed. After induction chemotherapy, surgical therapy with anterior rectum resection and a resection of the liver metastases was performed. Two metastatic lesions were resected out of segment two and three to get the left hepatic lobe free of tumor, whereas the main metastatic mass was located in the right one. Embolization and right hemihepatectomy was the next step of the treatment strategy in our case. After two years the remaining liver was re-infiltrated by suspect tumor masses, whereby one of three did not represent a metastasis of rectal cancer but a cystic lesion located in the remaining segment four. Retrospectively this cystic lesion could be seen in CT-scans even on initial preoperative staging imaging studies. Following surgical therapy composed of radical tumor exstirpation, hemihepatectomy and resection of isolated hepatic and pulmonary metastases for two times the patient is still alive and in good condition six years after diagnosis of advanced rectal cancer.
In this patient the size of the cystic tumor between the left and middle hepatic vein was about 13 mm, which makes radiologic diagnosis very complex. According to the patient´s medical history it was assumed that the lesion was suspicious for another liver metastasis. A variety of differential diagnoses for hepatic lesions with different characteristics in radiologic imaging are described in Table 1: haemangioma, focal steatosis, cysts, focal nodular hyperplasia are frequent intrahepatic benign lesions, metastases, hepatocellular carcinoma, cholangiocellular carcinoma are known for common malignant lesions inside the liver and have to be kept in mind by the treating surgeon. One morphologic characteristic of hepatic metastases on the CT-scan is a mostly asymmetric and highly variable contrast enhancement [5]. Thereby it can be difficult to differentiate small lesions under a size of 1 cm by CTimaging (Table 2). Two years after hemihepatectomy resection of both the histopathologically confirmed metastatic spread in the remaining segment one and four as well as the cystic lesion between the left and middle hepatic vein was accomplished.
After first histopathological examination the pathologists revealed the diagnosis of a ciliated foregut cyst for the mass in segment 4 (between the left and middle hepatic vein), which can be subdivided into BC and CHFC. CHFCs are rare entities. Due to the typical subcapsular location of the cystic lesion between the left and middle hepatic vein in the remaining segment 4 (Figure 1), a CHFC was the most probable diagnosis [27]. After further histological processing the cyst showed resemblance of bronchial mucosa with ciliated epithelial cells, connective tissue and smooth muscle cells. Furthermore it showed stroma with partial chondroid differentiation. In immunohistochemical staining the cyst showed no positivity for CEA, whereas Terade et al. described CHFC to be more positive in CEA than bronchial epithelia [29]. Furthermore the gland cells inside the cyst were positive for TTF-1, as a biochemical marker for a primary bronchial origin (Figure 2) [30].
The diagnosis of an intrahepatic BC was made due to the lack of malignancy and the characteristic histopathological pattern: ciliated epithelial cells, connective tissue, smooth muscle cells and stroma with partial chondroid differentiation, negativity for CEA and positivity for TTF-1 in immunohistochemistry (Figure 2). BCs are known as intrathoracic malformations of the primitive ventral foregut derived during the development of bronchi and lung [7] and can also appear inside the abdominal cavity [17,22]. For the first time we describe and confirm that BCs can appear subcapsularly inside the liver parenchyma.
Similar to the development of intraabdominal BCs and CHFCs an outpouching of the primitive hepatic foregut with metaplastic mutation or an abnormal bronchiolar budding through the (open) pericardioperitoneal canal are the most reasonable hypotheses for the genesis of the herein described intrahepatic BC [22,24].
(1) BCs are known as residual malformations of the primitive foregut and normally appear intrathoracally in the lung and mediastinum whereas other locations are rare. (2) An intraabdominal and retroperitoneal location of BCs was reported, but an intrahepatic BC had never been described before. (3) In our case we present a BC, which appeared in the liver parenchyma and mimicked a hepatic metastasis of a rectal carcinoma both in the preoperative staging-CT and during intraoperative ultrasound examination. For the oncologic surgeon BCs, located inside the liver thus represent one potential differential diagnosis for hepatic metastasis of colorectal origin.
Written informed consent was obtained from the patient for publication of this Case report and any accompanying images. A copy of the written consent is available for review by the Editor of this journal.
MR and AH are equally contributed to this manuscript. MR, AH and A-LA aquisted the clinical data, AB and SG made histological staining and interpreted them. JPH, JB and WP revisited the manuscript critically and gave important intellectual content. Each author participated sufficiently in the work and gave final approval for publication.