Journal of Medical Diagnostic Methods
Open Access
ISSN: 2168-9784
ISSN: 2168-9784
Case Report - (2016) Volume 5, Issue 3
Carotico-cavernous fistula (CCF) is a rare entity referring to abnormal communication between cavernous sinus and carotid arterial system (either internal or external or both) directly or through their branches. Though majority of cases have been reported secondary to head trauma yet spontaneous cases have also been described. We present an interesting case of CCF that developed secondary to blunt ocular trauma not yet described in the medical literature.
Keywords: Cavernous; Carotid; Ocular; Trauma
Carotico-cavernous fistula (CCF) is a rare arteriovenous malformation involving the cavernous sinus and either internal or external carotid artery or both or their branches. It may be further classified in to direct or indirect types based on presence or absence of direct communication with intra-cavernous part of internal carotid artery (ICA). Direct CCF is secondary to aneurysmal rupture of ICA or closed head trauma involving base of skull, hence commoner in young male working outdoors with usually acute presentation while indirect CCF is usually spontaneous occurring in elderly especially postmenopausal females following a more indolent course than direct type [1]. Though ocular trauma is also commonly seen in day-to-day practice yet it has not been described as a cause of CCF. In this article, we are describing a rare case of CCF that developed secondary to ocular trauma with its pathogenesis.
A 36 yr-old female presented with pulsating headache and proptosis of left eye during last few days. History taking revealed blunt injury to left eye by an umbrella-stick 3-4 months back that gave rise to severe and sudden orbital pain with reduced visual acuity in left eye. Since then she was having reddening of eyes and orbital swelling. She took local treatment for the same for few weeks without any imaging investigation during which her eyelid swelling subsided and visual acuity slightly improved but reddening of eyes increased. During last few weeks she felt that her left eye is protruding out with limitations of ocular movements.
Clinical examination revealed chemosis, increased intraocular pressure, mild external ophthalmoplegia and mild 6th cranial nerve palsy with normal fundoscopic examination. No local bruit was noted. Laboratory examinations including complete blood counts and thyroid functions test were unremarkable.
Magnetic resonance imaging (MRI) brain and orbits was then advised for further evaluation of cause of proptosis. Noncontrast MRI revealed enlarged left cavernous sinus with multiple flow voids and dilated superior and inferior ophthalmic veins with soft tissue stranding in intraconal and extraconal orbital fat without obvious signs of any obvious mass lesion. Contrast-enhanced images with MRA revealed enlarged cavernous sinus; dilated superior and inferior ophthalmic veins with their draining tributaries and multiple, tiny, dilated arteries within the early enhancing left cavernous sinus. No evidence of any obvious dilatation of right orbital or intercavernous veins or aneurysm was noted. Based on imaging findings, diagnosis of carotico-cavernous fistula (type B) was made which is rarer than other types.
Patient was then immediately referred to higher neurointerventional centre for further management.
CCF is an abnormal communication between the carotid arterial system and the cavernous sinus. Barrow classification of CCF is as follows [2]:
Type A: direct connection from cavernous ICA Type B: connection from meningeal branches of ICA Type C: connection from meningeal branches of ECA Type D: connection from meningeal branches of ICA and ECA
Type A CCF is commonest (~75%) and is high-flow fistula while Type B, C and D CCFs are low-flow fistulae with Type C being commoner.
CCF leads to increase pressure in cavernous and communicating sinuses leading to alteration of flow direction/drainage with consequent symptoms [3]. Commonest cause of Type A is head trauma or rupture of cavernous ICA aneurysm [2,4]. Etiology of Types B, C and D (dural CCFs) is unclear with postulated mechanism being tearing of small meningeal vessels with or without thrombosis leading to neovascularization and fistula formation. Miscellaneous causes include abnormal arteries as in Ehlers-Danlos syndrome, pseudoxanthoma elasticum, fibromuscular dysplasia, etc. and hypercoagulable states as PT mutations, pregnancy, etc.
However, none of the previously reported cases have preceded ocular trauma as seen in our index case. The postulated mechanism is that blunt ocular trauma probably lead to sudden and significant increase in intraocular pressure that was transmitted through ophthalmic veins to the cavernous sinus leading to tear of small meningeal vessels leading to fistulous arteriovenous communication between the meningeal branches of ICA and cavernous sinus.
Clinical presentation is usually pulsatile exophthalmos, chemosis with or without subconjunctival hemorrhage, proptosis, progressive visual loss, pulsatile tinnitus, signs of raised intracranial pressure and complications of CCF like subarachnoid or intracerebral bleed, otorrhagia or epistaxis [3-6] (Figure 1).
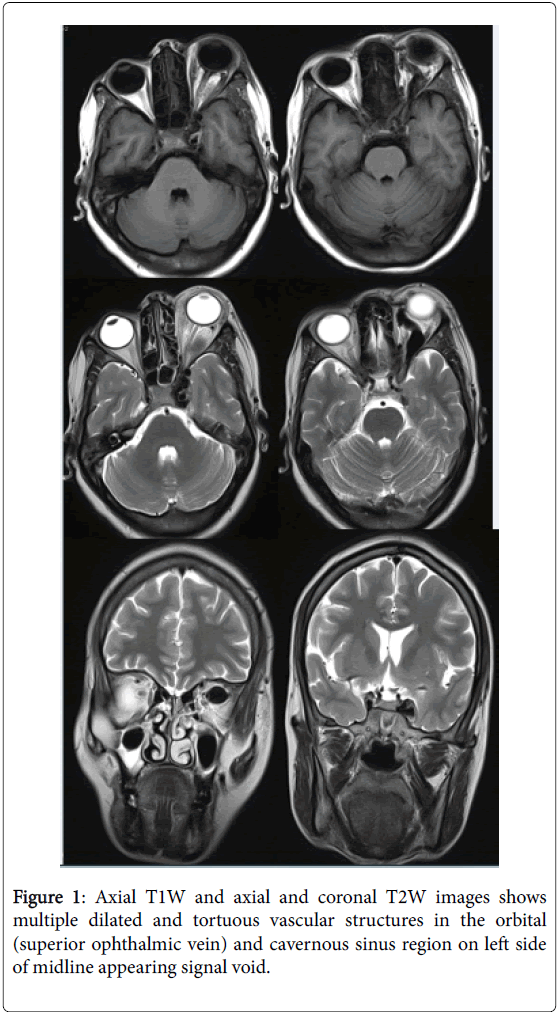
Figure 1: Axial T1W and axial and coronal T2W images shows multiple dilated and tortuous vascular structures in the orbital (superior ophthalmic vein) and cavernous sinus region on left side of midline appearing signal void.
Computed tomography or magnetic resonance angiography (CTA / MRA) are the preferred noninvasive method of diagnosis. They show enlarged cavernous sinus with convex lateral margin and dilated superior ophthalmic veins. They may also reveal signs of orbital edema, slight enlargement of ipsilateral extraocular muscles due to venous congestion or complications of CCF as described above. Thrombi may be seen as filling defects in the cavernous sinus.
They have lower sensitivity for types B to D than with Type A. CTA is optimal for Type A while MRA is superior in Type B, C and D and in demonstrating venous channels which are very important in predicting prognosis and optimal method of management [7,8].
True FISP imaging, susceptibility weighted, High-Resolution Time- Resolved MR-Angiography with Stochastic Trajectories (TWIST) and Extended Parallel Acquisition Technique (ePAT 6) sequences have been reported to be quite useful in MRA [9-11]. Early CCF may even require careful evaluation of source images rather than maximum intensity projection images [12].
Though CTA / MRA may be useful in planning management but cerebral angiography is still considered as a gold standard for diagnosis of CCF especially in pretreatment planning which shows filling of venous sinuses during the arterial phase, retrograde flow from cavernous sinus to ophthalmic veins and enlarged draining veins [13,14].
Though transcranial and orbital Duplex ultrasound may allow visualisation of arterialized cavernous sinus and superior ophthalmic vein and in flow measurements but not very useful in making a specific diagnosis [15].
Transarterial embolisation with wide variety of embolising material is management of choice for high-flow, direct CCF while low-flow, indirect CCF may either undergo spontaneous closure or may require transarterial as well as transvenous approach [16] (Figures 2 and 3).
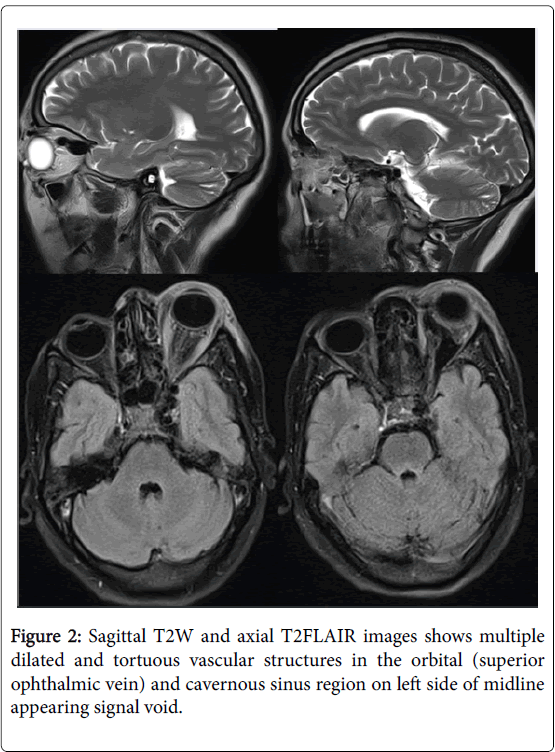
Figure 2: Sagittal T2W and axial T2FLAIR images shows multiple dilated and tortuous vascular structures in the orbital (superior ophthalmic vein) and cavernous sinus region on left side of midline appearing signal void.
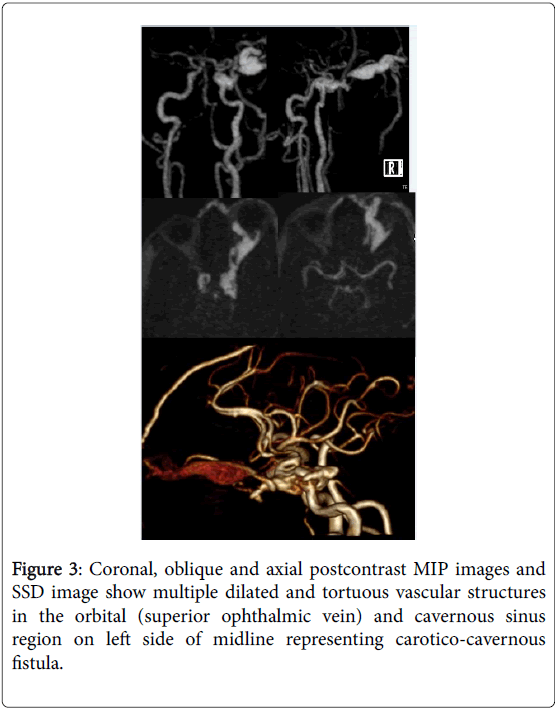
Figure 3: Coronal, oblique and axial postcontrast MIP images and SSD image show multiple dilated and tortuous vascular structures in the orbital (superior ophthalmic vein) and cavernous sinus region on left side of midline representing carotico-cavernous fistula.
CCFs are usually of high-flow type secondary to cranial trauma presenting with ipsilateral ocular pain, increased intraocular pressure and proptosis. However, slow-type of CCF may also be secondary to ocular trauma as seen in our case. Though, cerebral angiography is gold standard especially prior to coil embolisation of fistula but a combination of dilated superior ophthalmic vein and dilated cavernous sinus with internal flow voids is diagnostic of CCF on CTA / MRA. Endovascular treatment is the treatment of choice for high-flow fistula.