Journal of Biomedical Engineering and Medical Devices
Open Access
ISSN: 2475-7586
ISSN: 2475-7586
Research Article - (2016) Volume 1, Issue 1
Keywords: Medical devices; Dialysis; Pharmacotherapy; Cerebral cortex; Cerebrospinal fluid; Rats; Monkey
The thesis of this paper is that bioengineered cranial bones with multiple intelligent functions can be developed for the effective treatment of currently intractable brain disorders with predominantly cerebral cortical pathology. These disorders include treatment-resistant neocortical epilepsies, cortically localized strokes, malignant tumors and traumatic injuries, as well as dementias, such as Alzheimer’s disease, with neurodegeneration in the archicortical – association cortical memory system. The reason is that the proximity of the neurocranium to the cortex offers natural expansion of its protective function to therapeutic interventions via a bioengineered structure.
What is the demand for such bioengineered cranial structures? According to the World Alzheimer Report 2014 [1], dementias, mostly Alzheimer’s disease, affect about 44 million people worldwide with annual societal costs about $600 billion. None of the approved drugs for Alzheimer’s disease effectively alleviate its devastating cognitive symptoms [2]. According to the 2014 report from American Heart Association “on average, every 4 minutes, someone dies of a stroke” in the US with 45% of stroke-related deaths occurring in the hospital despite the availability of treatments [3]. Among discharged stroke survivors “~45% return directly home, 24% are discharged to inpatient rehabilitation facilities, and 31% are discharged to skilled nursing facilities” [3] constituting evidence of ineffective care for stroke. Also, in the last 10 years, traditional chemotherapy and neurosurgery hardly improved the grim statistics of malignant brain tumors, especially gliomas, of which median survival rates have been 12-15 months in ~17,000 new American patients per year [4]. It is also true that oral pharmacotherapy and resective neurosurgery are still the prevalent treatment options for epilepsy ever since Sir Charles Locock’s pioneering bromide therapy and Sir Victor Horsley’s revolutionary surgical procedures in the 19th century. These treatments changed medicine and their advanced forms now bring relief from seizures to about 70% of patients with epilepsy, but the remaining ~30%, tens of millions worldwide, are resistant to oral or intravenous antiepileptic drugs and/or are unsuitable for resective surgery [5,6]. Thus, a huge need developed for new treatments such as ingenious novel techniques of embolectomy and thrombolysis for ischemic stroke [7], implanted chemotherapy wafers for brain tumors [4,8] and the responsive neurostimulator for epilepsy [9,10]. Our proposal extends prior and current efforts of other teams who have pioneered the use of intracranial drug delivery systems for brain disorders [4,8,11-25].
Three facts support the feasibility of a bioengineered, multifunctional neurocranium to treat currently intractable cerebral cortical disorders. First, this is consistent with the seemingly universal law that permeates the evolution of living organisms and human culture by adding increasingly more functions to the original protecting/separating role of walls, wherever these walls are. This is as manifested in the orchestrated acts of different ion channels, transmitter receptors, immune receptors, transporters, adhesive molecules, secreting vesicles, and other molecular machines enriching the neuronal membrane as in the emerging effort by smart house technology to transform the walls of buildings from mere protective blocks to intelligent structures optimizing lighting, temperature, acoustic environment, security, entertainment, communication and health monitoring for those who live inside. Certainly, adding intelligent functions to the bony elements of the braincase for medical purposes is analogous to the mentioned, though seemingly distant, examples. Second, as shown in Figure 1, the ~6 mm thick cranial bones can readily accommodate bioengineered intelligent components without resulting in anatomical deformation, while the ~5 mm deep subarachnoid space filled with cerebrospinal fluid (CSF) is sufficient to connect the bioengineered implant to the cerebral cortical tissue. Thus, the proposed therapeutic system naturally fits in human anatomy. Third, this engineered therapeutic system is related to several existing implantable medical devices, from cardiac pacemakers and cochlear implants through deep brain stimulation and intrathecal pump systems to many other analogous devices for diseases untreatable by traditional drugs or surgery [21,26,27]. Considering the almost 50-year experience with these implantable medical devices it is reasonable to conclude that novel devices can be added to the existing ones, as we suggest for bioengineered cranial bones with multiple intelligent functions to advance neurological and psychiatric patient care.
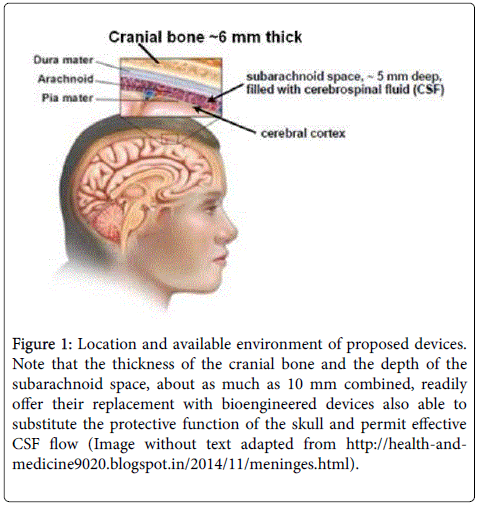
Figure 1: Location and available environment of proposed devices. Note that the thickness of the cranial bone and the depth of the subarachnoid space, about as much as 10 mm combined, readily offer their replacement with bioengineered devices also able to substitute the protective function of the skull and permit effective CSF flow (Image without text adapted from http://health-andmedicine9020. blogspot.in/2014/11/meninges.html).
The foundations of the medical approach examined in this article have already been laid down: the clinically tested Responsive Neurostimulator (RNS system) by NeuroPace Inc. (Mountain View, CA) and our preclinically tested Subdural Pharmacotherapy Device (SPD) are implantable in an under the cranial bones for therapeutic purposes.
The RNS device
The RNS device, approved by the FDA in 2013, is entirely implanted in the cranial bone overlaying the epileptic seizure focus or foci. Thus, it adds a new, therapeutic, function to the implanted patients’ protective cranial bones. The RNS system comprises (a) a microprocessor/microcontroller for online EEG analysis, seizure detection and the generation of 0.5 mA -12 mA electrical impulses of 1-333 Hz, as needed, in response to seizure detections, (b) subdural electrodes with or without depth electrodes to record the EEG signals and deliver electrical impulses, and (c) a power source [9,10]. Clinical trials in 256 patients with a median follow-up period of 5.4 years showed that although no seizure freedom was achieved in the implanted and neurostimulated patients throughout the entire trial period and 18% of patients (“non-responders”) experienced increased seizure frequency, the epileptic condition improved in as much as 82% of the patients [9,10]. Comparing seizure frequencies between Treatment (neurostimulated) and Control (implanted but not neurostimulated) groups, the former had a 37.9% reduction, significantly greater than the 17.3% reduction found in the control group [9,10]. Overall, the RNS-treatment proved to be safe and to increase quality of life [9,10]. These successful clinical tests presage worldwide spread of the NeuroPace system and proliferation of new studies to improve and expand on this technology.
The SPD apparatus
The design of our bioengineered cranial implant, the Subdural Pharmacotherapy Device (SPD; Figure 2) in continuation of our US Patents No. 6,497,699; 8,868,176; 9,042,974 and 9,233,237 shows that it can perform multiple site-specific functions [6,30-40]: (1) Delivery of medication into the site of pathology, be it a seizure focus, malignant tumor, area of a cerebrovascular insult, traumatic injury or neurodegeneration. (2) Drainage (dialysis) of harmful endogenous molecules and potential neurotoxins to clear the treated cells’ environment. (3) Sampling for routine chemical and proteomic analyses of patient-specific biomarkers to tailor delivered drugs for localized precision medicine. (4) Recording EEG for feedback from treated tissue to assess in real time the safety and efficacy of the SPD treatment. (5) Bi-directional wireless communication between implant and physician, assuring immediate recognition of local side-effects and adjustment of the SPD as needed. Because of the site-specificity of this “pharmacodialysis” treatment [30] and because it uses electrophysiological feedback along with neurochemical biomarkers to adjust the right drugs ranging from neurotransmitter receptor agonists and antagonists to gene function modulators, this is an intelligent system with the potential to significantly improve, even restore, health in patients with predominantly cortically localized epilepsies, strokes, injuries, tumors and dementias. Preclinical studies have extensively demonstrated the safety and antiepileptic efficacy of this cranially implantable apparatus (see next section). Its main advantage over electrical stimulators is that it can modulate the specific neurochemical and molecular mechanisms that regulate neuronal output patterns as well as the interactions of neurons with glial cells, local blood flow and the immune system, increasing therapeutic efficacy.
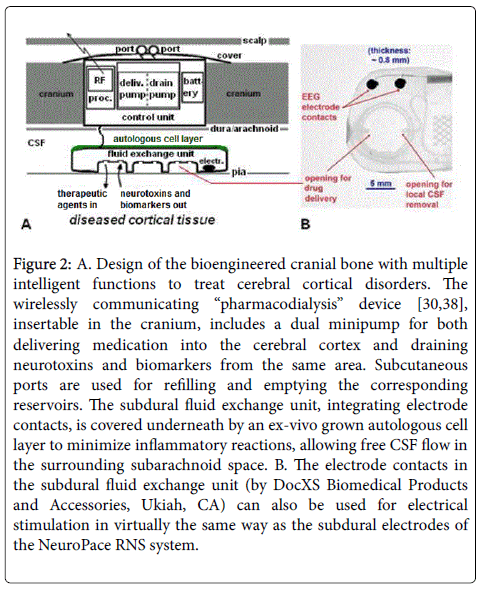
Figure 2: A. Design of the bioengineered cranial bone with multiple intelligent functions to treat cerebral cortical disorders. The wirelessly communicating “pharmacodialysis” device [30,38], insertable in the cranium, includes a dual minipump for both delivering medication into the cerebral cortex and draining neurotoxins and biomarkers from the same area. Subcutaneous ports are used for refilling and emptying the corresponding reservoirs. The subdural fluid exchange unit, integrating electrode contacts, is covered underneath by an ex-vivo grown autologous cell layer to minimize inflammatory reactions, allowing free CSF flow in the surrounding subarachnoid space. B. The electrode contacts in the subdural fluid exchange unit (by DocXS Biomedical Products and Accessories, Ukiah, CA) can also be used for electrical stimulation in virtually the same way as the subdural electrodes of the NeuroPace RNS system.
However, the SPD is still in the preclinical phase and needs to be improved before clinical trials. Since it uses drug delivery, molecular drainage and electrophysiological recording, it is the most complex experimental medical device to date and as such potentially prone to malfunction. Thus, SPD-like devices must be perfected and undergo thorough preclinical testing.
Efficacy studies
Is medication delivered transmeningeally through the subarachnoid space, as shown in Figure 2, indeed be able to prevent focal neocortical seizures? To answer this question it was sufficient to use rats not implanted with the cranial device, rather with an “epidural cup” only. Accordingly, each rat was implanted with such a cup made from 200 μl, capped, plastic test tubes, with the cup gently laid on the dura mater in a 4.5 mm diameter craniotomy over the right parietal cortex, followed by securing the cup to the skull with dental cement [28,33]. This allowed the manual delivery of drugs transmeningeally, through the dura and pia maters, into the examined rat’s cerebral cortex and to test the pharmacological effects of these compounds. The experiments showed that transmeningeal pentobarbital immediately stopped acetylcholine (Ach)-induced focal neocortical seizures and completely prevented seizures if given before seizure induction. It is important to note that the very small targeted pentobarbital doses caused no behavioral alterations whatsoever, despite the well-known sleeppromoting effects of orally, intravenously or intracerebroventricularly administered pentobarbital and other barbiturates [33].
The epidural cup method could also be used for comparative transmeningeal efficacy studies in rats. Muscimol, a GABAA-receptor agonist was by far the most effective and practical transmeningeally delivered compound, since it is also water-soluble at physiological pH and stable in effective (0.1 mM-1.0 mM) solutions [6,28,33], prompting us to select muscimol for seizure-prevention. Since epidural cups are not acceptable clinically, whereas the cranially implantable pharmacodialysis device (SPD) shown in Figure 2 is too large for implantation in rats, we used the SPD in chronically surviving monkeys to deliver muscimol transmeningeally into the frontal cortex, the site of the most treatment-resistant focal epilepsies in humans. Thus we could collect clinically relevant information on the safety and efficacy of our muscimol-delivering pharmacodialysis device preparatory for potential clinical trials. This novel neurotherapeutic technology is highly effective in preventing focal frontal cortical seizures [6,35-37], illustrated here in Figure 3.
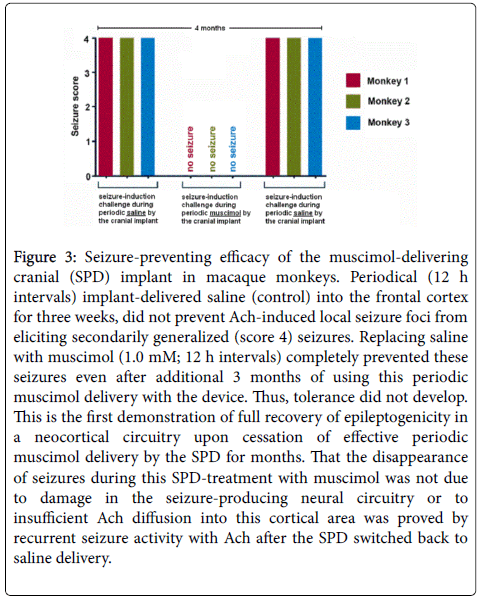
Figure 3: Seizure-preventing efficacy of the muscimol-delivering cranial (SPD) implant in macaque monkeys. Periodical (12 h intervals) implant-delivered saline (control) into the frontal cortex for three weeks, did not prevent Ach-induced local seizure foci from eliciting secondarily generalized (score 4) seizures. Replacing saline with muscimol (1.0 mM; 12 h intervals) completely prevented these seizures even after additional 3 months of using this periodic muscimol delivery with the device. Thus, tolerance did not develop. This is the first demonstration of full recovery of epileptogenicity in a neocortical circuitry upon cessation of effective periodic muscimol delivery by the SPD for months. That the disappearance of seizures during this SPD-treatment with muscimol was not due to damage in the seizure-producing neural circuitry or to insufficient Ach diffusion into this cortical area was proved by recurrent seizure activity with Ach after the SPD switched back to saline delivery.
But were these results indeed relevant to humans? In a corresponding human study we found [40] that before the neurosurgical resection of the neocortical seizure focus irrigation of the epileptic tissue with lidocaine (as muscimol was not approved for this study at that time) significantly reduced epileptiform EEG activity. This study demonstrated for the first time that transmeningeal drug delivery can produce antiepileptic effects in the convoluted human neocortex, even in the frontal cortex so prone to generate intractable focal seizures in epileptic patients.
Safety studies
In monkeys we extensively documented that transmeningeal drug delivery by our cranial implant left the animals’ overall behavior and health status intact as long as the studies lasted, often for more than one year [35-38]. Tolerance or toxic effects did not develop to targeted local muscimol, owing to its low concentration and absence of systemic appearance. However, as in clinical practice with oral antiepileptics, abrupt cessation of SPD-treatment induced withdrawal seizures, a problem eliminated by tapering muscimol concentrations. Further, as with all intracranial medical devices, the SPD induced sterile inflammatory tissue reactions in the implantation site, but without any clinical symptoms. When monkeys learned locations of baited food-ports, avoiding non-baited ones in a test chamber, their spatial memory was unchanged after SPD implantation and use [38]. Figure 4 and the corresponding Supplemental Video show an implanted monkey climbing in the test chamber, displaying behaviors indistinguishable from normal, while their SPD-transmitted local EEG recordings also reflected normal neural activity in the implanted/ treated area.
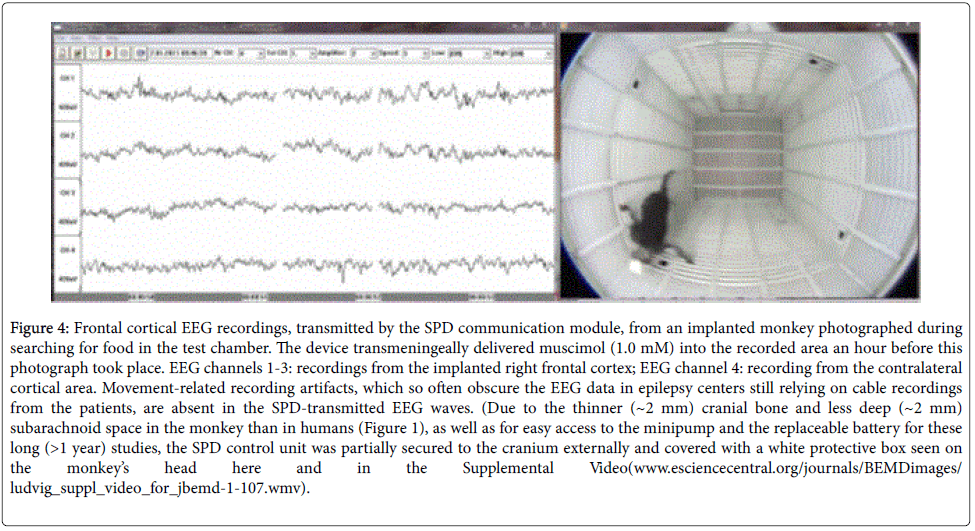
Figure 4: Frontal cortical EEG recordings, transmitted by the SPD communication module, from an implanted monkey photographed during searching for food in the test chamber. The device transmeningeally delivered muscimol (1.0 mM) into the recorded area an hour before this photograph took place. EEG channels 1-3: recordings from the implanted right frontal cortex; EEG channel 4: recording from the contralateral cortical area. Movement-related recording artifacts, which so often obscure the EEG data in epilepsy centers still relying on cable recordings from the patients, are absent in the SPD-transmitted EEG waves. (Due to the thinner (~2 mm) cranial bone and less deep (~2 mm) subarachnoid space in the monkey than in humans (Figure 1), as well as for easy access to the minipump and the replaceable battery for these long (>1 year) studies, the SPD control unit was partially secured to the cranium externally and covered with a white protective box seen on the monkey’s head here and in the Supplemental Video(www.esciencecentral.org/journals/BEMDimages/ludvig_suppl_video_for_jbemd-1-107.wmv).
The idea of using bioengineered cranial bones with multiple intelligent functions for the therapy of currently untreatable brain disorders is merely an extension of our and others’ two-decade-long concept of intracranial drug delivery systems. Such systems have been proposed and tested experimentally, with some even used clinically, by many investigators whose achievements inspired our work. Thus, the following published animal and human studies of implantable drug delivery systems to treat otherwise unmanageable epilepsy [11,14,15,22-25], stroke [16], Alzheimer’s disease [13], malignant brain tumors [8,12] and Parkinson’s disease [18,20] are discussed below.
Medical prospects
Epilepsy: Based on clinical results with the RNS device [9,10] and the preclinical results in nonhuman primates with the antiepileptic SPD, we anticipate that further improvements on these devices will lead to the first generation of bioengineered, multifunctional cranial bones providing seizure-freedom without side-effects to epilepsy patients resistant to systemic antiepileptic drugs and unsuitable for resective neurosurgery. A potential approach might be to combine the RNS and SPD systems, as this would offer the use of both responsive neurostimulation and periodic, responsive or non-responsive, neurochemical treatment via drug delivery and proconvulsant molecule clearance in the treated seizure focus or foci. The treatment could start with routine neurostimulation and either be continued alone in highly responsive patients or alternated with a neurochemical protocol in the nonresponders, especially after the neurochemical profile of their seizure focus or foci is available through analyses of the SPD-collected biomarkers. The device shown in Figure 2 has all components for this combination therapy. Specifically, as the SPD subdural unit integrates both fluid delivery/drainage ports and EEG electrode contacts (Figure 2) the latter can also be readily used for RNS-type electrical stimulation of the treated area. Ideal candidates for this RNS-SPD combination therapy would be patients whose frequent weekly or daily seizures require complete seizure-freedom for them to experience meaningfully improved quality of life. This medical objective would be more likely to be met by combining RNS-SPD as above than with the sole use of either system. The risk of infection introduced with SPD use could be eliminated by quarterly percutaneous refilling and emptying of the delivery and drain pumps (Figure 2) by specially trained staff using continuously updated methods to maintain the sterility of the SPD refilling and emptying kits and decontaminating and cleansing the ~2 cm2 area on the scalp overlaying the subcutaneous refilling and emptying ports.
Ischemic and hemorrhagic cortical strokes: The basics of using bioengineered cranial bones with multiple intelligent functions in stroke have already been described [34]. For people with ischemic stroke who have missed the therapeutic window for tPA and/or embolectomy, have contraindications for undergoing these procedures, or who have severe residual hypoperfusion due to insufficient recanalization, and those with hemorrhagic strokes, a viable therapeutic option would be to replace their cranial bone over the area of stroke with a bioengineered, multifunctional bone. Such a devicecarrying bone can deliver necessary neurotrophic factors and edema reducers along with drugs and vectors into the penumbra to promote neuroregeneration, neuroplasticity and neurogenesis. Coupling this treatment with drainage of harmful and regeneration-inhibitory extracellular molecules from the damaged tissue (Figure 2) would be especially beneficial for stroke patients with decompressive hemicraniectomy, hematoma evacuation or other neurosurgical procedures which could readily be complemented by replacing the bone flap with a bioengineered multifunctional one.
Dementias: There are problems with current systemic pharmacotherapy for dementias including Alzheimer’s disease. First, systemic drug administration has systemic side-effects often causing discontinuation of the treatment. Second, many drugs, including neurotrophic proteins, do not cross the blood-brain barrier and thus lack efficacy. Third, systemic drugs cannot specifically target the hippocampal-association memory circuitry responsible for the predominant symptom in Alzheimer’s disease, memory impairment. Fourth, no systemic drug administration can clear the hippocampalassociation cortical extracellular space from all potentially neurotoxic molecules ranging from amyloid beta oligomers and proinflammatory cytokines to extracellular tau. Bioengineered cranial bones with their multiple intelligent functions can eliminate these problems through localized delivery of therapeutic agents, including proteins, into the hippocampal – association cortical memory circuitry, drainage of potentially neurotoxic endogenous molecules and recording local electrophysiological patterns to guide the treating physician to adjust optimized delivery/drainage parameters [40].
Glioma and other malignant brain tumors: Post-surgical drugreleasing wafers (e.g., the Gliadel® wafer) and Convection-Enhanced Delivery (CED) devices have already been tested with promising, though not consistent results [4,8,12]. As SPD-like bioengineered cranial bones use dual minipumps, offering both deeper drugpenetration into the surrounding tissue than wafers and the additional function of carcinogenic molecule drainage which CED devices do not have, our proposed system could also be used for completing cortical glioma resection with adjuvant resection-cavity treatment to prevent the lethal recurrence of the malignant tumor.
Parkinson’s disease: Intracranial drug delivery, specifically lidocaine and muscimol delivery into the subthalamic nucleus [18] and glial cellline derived neurotrophic factor (GDNF) delivery into the putamen [20], was shown to result in clinical improvement in patients with Parkinson’s disease. Bioengineered, multifunction cranial bones with the ability of delivering these and other drugs, including transcription modulators, while also draining such harmful extracellular molecules as α-synuclein and proinflammatory cytokines [30] not only in the subthalamic nucleus and putamen but also in the motor cortex may further increase the efficacy of intracranial pharmacotherapies for Parkinson’s disease.
Other conditions: The proposed methodology has the potential to be extended to patients suffering from traumatic brain injury, multiple sclerosis, depression, schizophrenia or even drug addiction. It remains to be seen whether drug delivery via bioengineered cranial bones can also be used for therapeutic gene modulation with curative intent.
Challenges
The engineering challenge is to downscale the current device (Figure 5) about 30% for easy implantation, in the neurocranium giving the patient a flawlessly functioning and cosmetically acceptable implant. Use of 3D-printing for shaping the system to the curvature of the skull will be beneficial. As indicated in Figure 2, the subdural bidirectional pump unit needs to be partially covered with “a nonproliferating layer of ex-vivo grown autologous cells to prevent inflammatory reactions without interfering with fluid movement in the fluid-exchanging ports and tubes” [37]. A titanium case allowing leakage-free connection between the control unit and the subdural fluid exchange unit awaits construction.
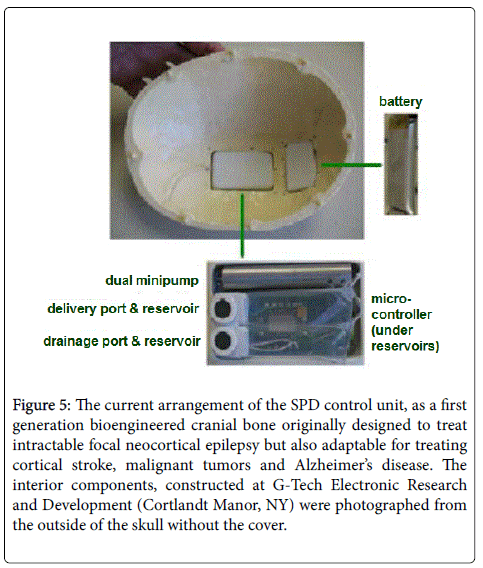
Figure 5: The current arrangement of the SPD control unit, as a first generation bioengineered cranial bone originally designed to treat intractable focal neocortical epilepsy but also adaptable for treating cortical stroke, malignant tumors and Alzheimer’s disease. The interior components, constructed at G-Tech Electronic Research and Development (Cortlandt Manor, NY) were photographed from the outside of the skull without the cover.
Scientific challenges include understanding cellular and molecular mechanisms mediating optimal therapeutic effects of this technology and possible interactions between the bioengineered cranial bone and the underlying cortical tissue. Furthermore working out an appropriate combination (or “cocktail”) of intracranially delivered small molecules, peptides, proteins and large molecules, with or without gene transcription- modulatory capabilities with or without vectors and/or nanoparticles will be challenging. These goals, preparing effective and safe devices for clinical use, will require large implantable mammals, such as monkeys and sheep.
The main clinical challenge is to identify candidates for implantation of the bioengineered, neurotherapeutic cranial bone. New phenotyping from advanced epidemiological studies of patient populations with treatment-resistant neurological and psychiatric disorders should enable creating a registry of patients for enrollment in clinical trials without patient or physician delay, using the full power of information technology in the 21st century.
Ethical challenges, guided by the World Medical Association (WMA) Declaration of Helsinki-Ethical Principles for Medical Research Involving Human Subjects, which includes language regarding animal welfare, will require a re-orientation based on educating the Public about the indispensable value of neuro-behavioral experiments in large animals to turn the prevailing public and political opposition to such research. The extremely complex interactions between the bioengineered neurotherapeutic bone and underlying brain tissue (Figure 2) cannot be simulated with computers and cannot be tested in vitro . Our suggested respectful experiments in implantable large mammals are absolutely necessary to prevent harming patients and are, indeed in agreement with the principles of the Declaration of Helsinki.
Intractable neurological and psychiatric disorders with predominantly cerebral cortical pathologies may be treated and even cured using bioengineered cranial bones with multiple intelligent functions. The functions include site-specific and long-term transmeningeal delivery of drug combinations acting on affected synapses and genes, and contemporaneous selective drainage of endogenous neurotoxins, together optimized via EEG feedback from the afflicted tissue. These concepts build on the pioneering efforts of many teams, including but not limited to us and our former colleagues. We have patented: 1) a cranially insertable dual function minipump for delivery and drainage of molecules, 2) a subdural membrane capable of directing delivered drugs and drained molecules transmeningeally in affected cortical areas in a spatially controlled manner for more than one year without the need of tissue-damaging cannulas or catheters, and 3) methods assuring durable clog-free function and selective realtime EEG feedback from the treated tissue to optimize treatment parameters. We and colleagues demonstrated the safety and antiepileptic efficacy of this complex procedure in a series of long-term experiments on nonhuman primates, proving that bioengineered cranial bones with multiple intelligent functions described here have realistic medical/therapeutic potential.
The data for Figure 3 was generated with the superb assistance of Dr. Hai M. Tang and Shirn L. Baptiste. The device shown in Figure 5 was partially designed and completely produced by Geza Medveczky, Richard Rizzolo and Sandor Toth. Supporting clinical advice regarding the antiepileptic potential of the SPD was given to the authors by Drs. Werner K. Doyle, Orrin Devinsky, Ruben I. Kuznieczky and Jacqueline A. French. Work on the SPD was supported by Epilepsy Research Foundation grant # 140929 to NL and funds from Finding A Cure for Epilepsy and Seizures (FACES).