Journal of Pharmaceutical Care & Health Systems
Open Access
ISSN: 2376-0419
ISSN: 2376-0419
Research Article - (2015) Volume 0, Issue 0
The Ugandan government has experimented with various supply chain models for delivery of essential drugs and supplies. In 2010, the dual pull-push system was adopted; however drug stock outs are still a common occurrence in health facilities. This study on availability of essential medicines during the dual Pull-Push system in Kaliro District was undertaken, to be used as an indirect or direct indicator of effectiveness of the dual pull-push system of drugs acquisition in the district. The study combined quantitative and qualitative methods; the study mainly based on; document review (stock cards, delivery notes,) and key informant interviews. Results showed that average stock-out duration of essential medicines and supplies was 23.89% (20.47 % for essential medicines and 27.32% for medical supplies). ACT Artemether/lumefantrine 20/120 mg tablets had the highest percentage stock-out followed by Cotrimoxazole 480mg tablets (51.6 and 32.4 %, respectively). Among the short falls of the system were; drug requisitions based on neither morbidity nor consumption methods of quantification, delays during distribution, supplying medicines with short shelf life, rare condition drugs or low usage drugs. In conclusion, the trend of essential medicines and supplies availability during the dual pull-push system seemed to be declining since its initiation in 2010. It is thus recommended that national medical stores involve stakeholders at all stages of medicines and supplies planning, especially the district health officers, who are the final consumers in the supply chain. The government can also adopt a revolving drug fund system, in the form of ‘Special Pharmacies and drug stores’ to enhance availability of essential drugs in public facilities and thus improve the quality of health care.
The concept of essential medicines was introduced by the world health organization (WHO) in 1977 [1]. Generally one third of the world’s population lacks access to needed medicines. This lack of access is even worse among the world’s poorest countries in Asia and Africa. In such countries, upto 50% of the total population lacks this access [2]. In Uganda, essential drugs are managed as a dual pull-push system. The government of Uganda purchases essential drug kits from the international market. In addition, the government purchases other required drugs both locally and internationally in bulk. Once in country, the national medical stores (NMS) pack them into kits and label them for each clinic. The amount per kit is determined periodically using morbidity and demographic data. The kits are distributed quarterly to the districts, which in turn ensure that they are directly delivered to the clinics as soon as they are received. Patient load and stock-out data is reported on a monthly basis to the central level. The NMS uses this data to review the order quantities for each of the kits and make adjustments accordingly. The current maximum is set at 5 months and minimum at 2 months for both the districts and the clinics [3]. For quantification and determining orders for drugs and other health commodities (not including equipment), the Uganda health system relies on dispenseto- user data gained from health unit monthly reports. The reports, part of the health management information system (HMIS), list rates of consumption for a variety of health commodities, and also note the number of stock-out days. However, the accuracy of the dispense-touser data is questionable. Facilities do not always order correctly or on time. Moreover, since the quantification and health commodity order system does not account for stock on hand at the facilities, the district level does not have an accurate view of the health commodities that are available, or in danger of stock-out. Furthermore, the quantification utilizes dispense-to-user data from previous months, and health commodity ordering does not accurately forecast the future needs of a facility [4]. The availability of pharmaceuticals has been identified as a significant predictor of perceived quality of health facilities [5]. A relationship exists between perceived quality of a health facility and a patient’s choice to utilize or not to utilize the facility. Studies have shown that as availability of pharmaceuticals decreases, patients reduce their positive perception of the facility [6]. It has been recommended that investment should be made to strengthen the monitoring system of pharmaceutical procurement and more autonomy should be given to facilities to monitor their stock [7]. Availability of funds, transport, staff training and supervision have been identified as key issues which should be addressed for maximal benefits from the pull system of drugs availability [8]. The drug supply chain management in Uganda has been noted to be characterized by parallel processes and information systems that result in poor quality and inefficiencies. The governance issues affecting the drugs supply chain management in this country include the lack of follow up on initial policy intentions and a focus on narrow, short-term approaches. The Ugandan government has experimented with various supply chain models for delivery of essential drugs and supplies. In 2010, the dual pull-push system was adopted; however drug stock outs are still a common occurrence in health facilities. This study on availability of essential medicines and supplies during the dual pullpush system was undertaken to evaluate the effectiveness of the system of drugs acquisition in Kaliro District, Uganda.
Ethical considerations
The ethical approval to conduct the study was granted by Kampala International University, School of Pharmacy Research and Ethics Committee. The District Health Officer for Kaliro district approved the study to be conducted in the health facilities that are situated in the district. All participants gave an informed consent before interviews were conducted. All other ethical issues pertaining to maintaining of confidentiality were strictly adhered to and observed during the study.
Study design
The study combined both Quantitative-Qualitative retrospective and prospective methods. The study employed two methods of data collection; Document review (Stock cards and delivery notes) and researcher guided key informant interviews. The study design used was adopted from the World Health Organization study protocol. Availability of essential medicines was measured by establishing the average number of days when the essential drugs stock-out.
Study area
The study was conducted in Kaliro district. Kaliro was created by an act of parliament in July 2005 and became operational in September 2005. It is bordered by Lake Kyoga in the North, Iganga District in the South, Namutumba District in the East and Kamuli District in the West (Figure 1). Administratively, it has one county, Bulamogi, comprising of six lower local governments. Of these, one is a self-accounting town council and five sub counties with a total of 34 parishes and 294 villages. Generally, the standard of living is very poor with most people living below a dollar a day. The means of livelihood is predominantly subsistence farming. The major foods grown are cassava, potatoes, maize and rice (all grown at subsistence scale).
Figure 1: Map showing location of Kaliro District.
Kaliro District is served by a total of 20 health facilities. Of these, 13 are government health units and 7 are non government. Of the government facilities, there is one health centre four (Bumanya HC IV) which is the last referral facility, 5 health centre IIIs and 7 HC IIs. Of the NGO/Private facilities, one is a HC III (Budini) and 6 are Health centre IIs.
Sample size determination
Health unit sample size determination was proportionate sampling, so as to include all health care levels; one Health Center IV, three Healths Center IIIs and three Health Center IIs, were randomly selected. The key informants were identified through snowball sampling. Six tracer medicines and four supplies were adapted from the MOH indicator drugs to measure availability of medicines and health supplies to provide priority healthcare.
Study population
Seven health centers were selected using a stratified approach, so as to include all health care levels; one HC IV, three HC IIIs and three HC IIs. Two key informants from the district health office, were purposively selected and interviewed, namely; the district health officer and the district stores’ in-charge. A total of nine (one from HC IV, four from HC III and four from HC II) healthcare unit in-charges and healthcare staff working at the drug stores were purposively selected and interviewed.
Data collection
Stock cards, delivery notes and delivery schedules were reviewed; key informant interviews were conducted.
Stock cards: Stock cards were reviewed for consumption period of 4 years; this is the period during which the dual push-Pull system (2010-2014) was in operation. The study was guided by a preadopted list of six essential drugs adopted from Uganda ministry of health; that drugs represented the different program areas and where present at all health care levels, were used as tracer drugs for this part of the study: artemisinin-based combination therapy (ACTs such as Coartem; (lowest weight brand)), sulfadoxine pyrimethamine (malaria treatment), co-trimoxazole (antibiotic for bacterial infections, particularly for HIV/AIDS patients, in four sizes), oral rehydration salt (diarrhoea treatment), medroxyprogesterone injection (birth control), and measles vaccine.
Key informant interviews: Qualitative data was collected using key informant interviews. Quantitative data was collected using data interview guides. The topics that were discussed with the key informants included: factors affecting availability of drugs, methods of drug quantification used, the drug ordering system.
Data analysis: All Data was transcribed and entered in Microsoft Word. Qualitative analysis was performed for theme identification using a content analysis approach. Results were presented in tables, graphs, charts, and pyramids. Descriptive statistics, correlation, multivariate analysis was done. The data was analyzed using SPSS IV.
Seven health facilities were visited; one HC IV, three HC IIIs and three HC IIs. Two key informants from the district Health office, were interviewed; the DHO and the district stores’ in-charge. A total of nine health unit in-charges and healthcare staff working at the drugs’ stores were purposively interviewed (one from HC IV, four from HC III and four from HC II).
Average duration of stock outs of essential medicines and supplies
The average stock-out duration of essential medicines and supplies was 23.89% (20.47% for essential medicines and 27.32% for medical supplies) as can be seen in Table 1.
| Days out of stock for 2010/11 | % out of stock for 2010/11 | Days out of stock for 2011/12 | % out of stock for 2011/12 | Days out of stock for 2012/13 | % out of stock for 2012/13 | Days out of stock for 2013/14 | % out of stock for 2013/14 | |
|---|---|---|---|---|---|---|---|---|
| Item | ||||||||
| ACT Artemether/lumefantrine 20/120mg Tab (Child dose) | 134 | 37.3 | 144 | 40 | 235 | 65.4 | 229 | 63.7 |
| Cotrimoxazole 480mg Tab | 116 | 32.21 | 124 | 34.6 | 116 | 32.2 | 110 | 30.6 |
| Medroxy progesterone 150mg/ml | 48 | 13.5 | 41 | 11.4 | 31 | 8.9 | 26 | 7.2 |
| Measles vaccine inj1M/SC | 17 | 4.8 | 15 | 4.3 | 6 | 1.9 | 10 | 2.8 |
| Oral rehydration Salts | 80 | 22.4 | 75 | 20.8 | 192 | 18.8 | 63 | 17.6 |
| Sulphadoxine-pyrimethamine 500/25mg Tab (SP) | 26 | 7.4 | 18 | 5.2 | 16 | 4.6 | 13 | 3.7 |
| Syringes 2cc needle disposable 21G | 169 | 46.9 | 163 | 45.5 | 158 | 44.1 | 164 | 45.7 |
| Cotton | 62 | 17.3 | 56 | 15.8 | 52 | 14.5 | 46 | 12.8 |
| Surgical gloves latex- 7.5 | 107 | 29.8 | 129 | 35.9 | 105 | 29.4 | 94 | 26.3 |
| Malaria rapid diagnostic test | 78 | 21.8 | 78.3 | 21.7 | 59 | 16.7 | 46 | 12.9 |
Table 1: Average duration of stock outs of essential medicines and supplies.
Availability of essential medicines and supplies in Kaliro district
The average availability of key medicines in the public health facilities was 76.11% (79.53% for essential medicines and 72.68 for medical supplies) as can be seen in Graph 1.
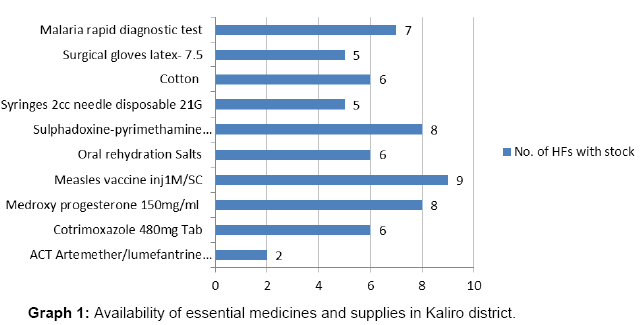
Graph 1: Availability of essential medicines and supplies in Kaliro district.
Essential medicines that commonly stock out in the district
ACT Artemether/lumefantrine (20/120 mg) had the highest percentage stock-out followed by Cotrimoxazole 480mg tablets (51.6% and 32.4 %, respectively). Table 2 below shows essential medicines that commonly stock out in the district.
| Item | No. of HFs out of stock last 1 month | % of HFs out of stock last 1 month | No. of HFs out of stock since 3 months | % HFs out of stock last 3 month |
|---|---|---|---|---|
| ACT Artemether/lumefantrine 20/120mg Tab (Child dose) | 6 | 15 | 7 | 12 |
| Cotrimoxazole 480mg Tab | 5 | 12 | 7 | 12 |
| Medroxy progesterone 150mg/ml | 3 | 7 | 4 | 7 |
| Measles vaccine inj1M/SC | 2 | 5 | 1 | 2 |
| Oral rehydration Salts | 4 | 10 | 7 | 12 |
| Sulphadoxine-pyrimethamine 500/25mg Tab (SP) | 3 | 8 | 2 | 4 |
| Syringes 2cc needle disposable 21G | 6 | 15 | 9 | 16 |
| Cotton | 3 | 8 | 6 | 11 |
| Surgical gloves latex- 7.5 | 4 | 10 | 6 | 11 |
| Malaria rapid diagnostic test | 4 | 10 | 7 | 13 |
Table 2: Essential medicines that commonly stock out in the district.
Factors influencing availability of essential medicines and medical supplies
The respondents identified factors affecting availability of essential medicines and medical supplies as; Drug requisitions based on neither morbidity nor consumption methods of quantification, Requisitions are based on credit available, poor distribution of logistics, such delays during distribution, Supplying medicines with short shelf life, rare condition drugs or low usage drugs, pushing some medicines more that can be utilized by a specified health unit, sometimes the requisitions are not fully honored as requested by the health units and population difference in the catchment areas.
It was also noted that the lead time was either inconsistent and thus made it hard to tell when the drugs would be delivered or was too long, to sustain a supply till its next replenishment, more so the supplier did not consider individual unit consumption rates.
The average availability of key medicines in the public health facilities was lower than that observed in a study conducted in Malaysia, or in the study conducted in another part of Uganda [8,9]. The average stock-out duration was also notably higher as compared to that of the studies above. The difference could possibly be attributed to the differences in the etiological differences in the locations from which theses studies were conducted. In this study ACT Artemether/ lumefantrine (20/120 mg) had the highest percentage stock-out followed by Cotrimoxazole 480mg, unlike what was noted by another study [8], which noted Quinine tablets had the highest percentage stock-out in the push system followed by ciprofloxacin and while diclofenac injection had the highest percentage stockout in the pull system followed by ferrous sulphate tablets. Since ACT Artemether/ lumefantrine (20/120 mg) tablets are used in the treatment of malaria, the stock-outs of this drug could have had a severe impact on the health of the population within the district. This is because fever-related illnesses, malaria included, have been identified to be major causes of mortality especially in children less than five years old in low-income countries like Uganda [10].
The factors that affected availability of essential medicines and medical supplies were quite diverse, while some varied from facility to facility. Some factors were consistently mentioned in most of the facilities. These included lack of consistency in the schedules of delivery, lack of consideration of the unique peculiarities that exist at the different health facilities among others. Lack of strong governance and coordination of the national system were also quoted to be adversely affecting the availability of essential medicines and supplies. These findings are consistent with other studies done elsewhere that found similar factors to be attributable to weak healthcare systems [11-17]. In this study, it was observed that the lead time for delivering drugs to the healthcare facilities was either inconsistent, or thus made it hard to tell when the drugs would be delivered or was too long to sustain a supply till its next replenishment. Such unreliability in obtaining drugs and medical supplies has been shown to result in the provision of untimely and suboptimal emergency obstetric care (EmOC) services at a rural district in Tanzania [18]. Authors of the study conducted in Tanzania recommend that multiple approaches be used in addressing the challenges within the health system that prevent access to essential drugs and supplies for maternal health. Inadequate availability of drugs has been reported to result into hindrance in providing simple clinical pain and symptom control protocols in Kenya and Uganda [19]. This further leads to unnecessary distress among patients. In another study conducted in Mozambique, it was noted that stock-outs of essential health products at health facilities disproportionately affects those living far from district capitals and near facilities with few health staff [20]. The authors of the study recommended that increased investment in public sector human resource capacity for healthcare could be employed as an intervention that could potentially decrease such stock-outs of essential health products. Interventions which have been put in place to strengthen most health systems usually ignore the interconnections between system components. Due to this phenomenon, populations’ access to medicines is usually addressed through fragmented, mostly vertical approaches that majorly focus on supply, unrelated to the wider issue of access to health services and interventions [21]. In another study conducted in South Africa, it was found out that among other things, logistical bottlenecks in the medicines supply chain hampered availability of medicines [22]. In that study, the authors also found out that poor public transport networks affected accessibility to medicines. In our study, the logistical bottlenecks were also identified as contributing factors in hampering the availability of medicines to the study area population. However, in our study, poor public transport network was not cited by the respondents as a hindrance factor to accessibility to essential medicines and supplies. Facility opening hours has been also noted to be a barrier to availability of medicines in Kenya [23]. This is in contrast to our findings in which such a factor was not cited as a barrier to medicines availability. Another study covering three countries, namely Ethiopia, Malawi and Rwanda found out that product availability was a challenge for every community case management (CCM) program [24]. The authors of the study point out that attempts to find affordable, simple and sustainable solutions to the supply chains must take into consideration the evidence, country context and program structures. Other authors have pointed out that sustainable adequate funding and use of supply chain management techniques are equally important considerations that can ensure that patients have access to essential medicines [25]. In a study conducted in Ethiopia, which was done to investigate whether fee waiver could protect patients from the burden of having to pay for medicines, it was found that the waiver improved availability of the medicines [26]. However, the authors of the study point out that the revolving fund system has the potential of creating a parallel system, in which the poor would not be able to access the drugs if they are not available at a cheap price in the pharmacies. Findings from our study indicate that availability of essential medicines and supplies needs to be improved from the current levels. Also, the factors that influence drug availability in the dual pull-push system of drugs acquisition need to be addressed.
The trend of essential medicines and supplies availability during the dual pull-push system seems to be declining since its initiation in 2010. It is thus recommended that national medical stores involve stakeholders at all stages of medicines and supplies planning, especially the district health officers, who are the final consumers in the supply chain. The government can also adopt a revolving drug fund system, in the form of ‘Special Pharmacies and drug stores’ to enhance availability of essential drugs in public health facilities and thus improve the quality of health care.
We acknowledge financial support from the Belgian Technical Corporation – Uganda. We would also like to appreciate the cooperation received from Kaliro district Local government, and the District Health Officer of Kaliro.