Andrology-Open Access
Open Access
ISSN: 2167-0250
ISSN: 2167-0250
Mini Review - (2014) Volume 3, Issue 2
Constitutional Delay of Growth and Puberty (CDGP) and hypogonadism are the two most common indications for Testosterone (T) therapy in adolescents. CDGP is a transient state of hypogonadotropic hypogonadism associated with prolongation of childhood phase of growth, delayed skeletal maturation, delayed and attenuated pubertal growth spurt. In pre-pubertal male with CDGP, T therapy can be used to induce pubertal development, accelerate growth and relieve the psychosocial complaints. However, some issues in the management are still unresolved. These include type, optimal timing, dose and duration of sex steroid treatment and the possible use of adjunctive or alternate therapy. In adolescents with permanent hypogonadism T therapy is used to induce then maintain pubescent development. Testosterone therapy enables the patient to decrease mood disturbances, fatigue, impaired virilization and osteoporosis. The use of anabolic drugs to enhance athletic performance has become a major concern for professional sport organizations, sport governing bodies and governments. This mini review aims at providing an update for androgen therapy in adolescents. Endocrinologists and physicians should be acquainted with the indications, the forms, optimal timing, monitoring, dose titration and possible side-effects of T therapy to accomplish the best pharmacological outcome. In addition, it is believed that through education and research we can mitigate the abuse of androgens by adolescent athletes.
<Keywords: Testosterone (T); Constitutional Delay of Growth and Puberty (CDGP); Hypogonadism; Growth; Insulin Growth Factor-I (IGF-I)
There are many indications for exogenous Testosterone (T) use in adolescents. Induction of puberty in males with Constitutional Delay of Growth and Puberty (CDGP) and replacement therapy for adolescents with hypogonadism constitutes the most common indications. In this mini-review the authors go through the physiologic role of androgen, pathological conditions that require its use and review some guidelines for its proper administration to adolescents.
Secretion of testosterone from birth to puberty
In males, T levels dramatically increase in the first day of life, and rapidly decline by the end of first week of life. T remains at low levels (20-50 ng/dL) (0.7-1.7 nmol/L) until “mini-puberty of infancy”, occurs between 20-60 days of life. The short-lived mini-puberty of infancy is gonadotropin-independent and T may reach the lower end of the adult range (300-450 ng/mL) (10.4-15.6 nmol/L). This T secretion induces an increase of the penile length during infancy [1-4]. After this period, Hypothalamic-Pituitary-Gonadal (HPG) activity becomes dormant with T levels undetectable or very low. The sensitive negative feedback mechanisms of the HPG work at maximum, and both the pituitary and gonads are capable of a functional response when stimulated during this inactive period. In males, pubertal onset occurs between 9 and 13.5 years [5]. Puberty is associated with increased frequency and intensity of LH pulses that changes gradually from nocturnal to a full 24 hour cycle, resulting in progressive rises in LH, FSH, and T [5,6]. Clinically, the first sign of true central puberty is testicular enlargement. Total T level follows a circadian rhythm in younger men, with T levels peak in the morning. This may lead to large discrepancies in T levels in the same adolescent when obtained in morning versus late afternoon. In mid-puberty, after considerable exposure to T, secondary sexual characteristics develop (pubic hair, axillary hair, voice deepening, acne) concomitant with achievement of the peak growth velocity and increased bine mineral accretion [5,6].
Mechanisms of testosterone action
Testosterone acts either directly on the androgen receptor, or acts in tissues that express the enzyme 5-alpha reductase, via conversion to Dihydrotestosterone (DHT), or acts on estrogen receptor, following conversion by aromatase to estradiol. T needs conversion to DHT for its action on the external genitalia (which includes the prostate gland) and sexual hair and requires conversion to estradiol for much of its action on bone (Figure 1). Therefore, in hypogonadal males, both androgen and estrogen levels are reduced. Androgen deficiency accounts for decreases in lean mass, muscle size, and strength whereas estrogen deficiency accounts for increases in body fat and both contribute to the decline in sexual function [7-14].
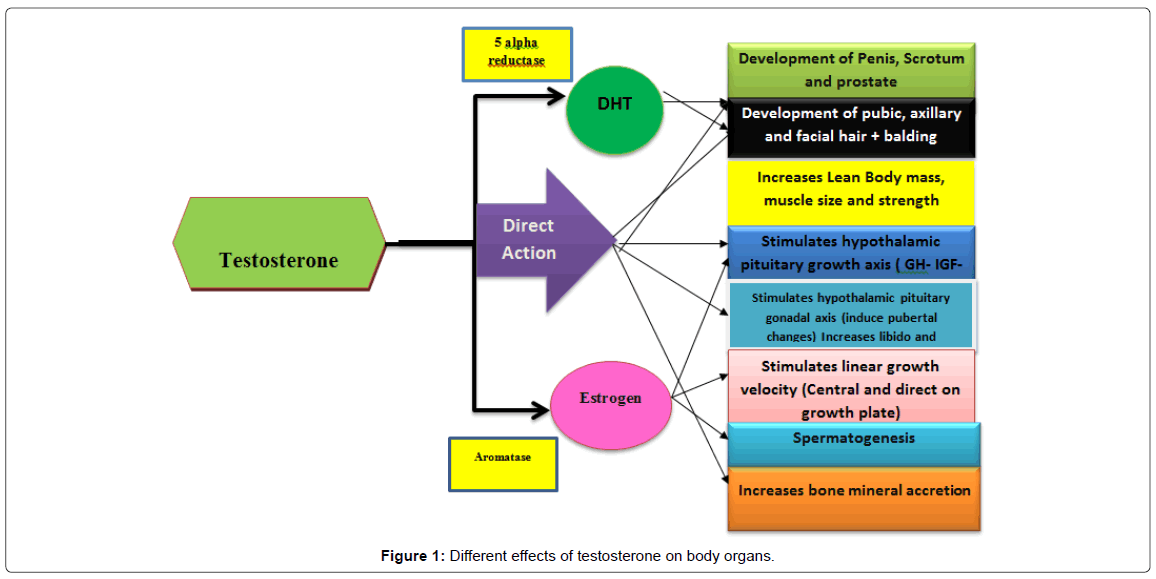
Figure 1: Different effects of testosterone on body organs.
Indications for T administration in adolescents
In adolescents, disorders of the HPG axis can manifest as complete failure of pubertal onset, a transient delay in pubertal onset or a delay in the progression of puberty, once initiated. The most common use for T in adolescents is for both pubertal induction in adolescents with CDGP and pubertal induction and maintenance in adolescents with hypogonadism.
Clinical and laboratory Assessment of CDGP (transient) versus permanent hypogonadism (Table 1) [15-20]
| Clinical/Lab test | CDGP | HH |
|---|---|---|
| Family history of delayed puberty | ++++ | +/- |
| History of orchitis or testicular trauma | None | + In hypergonado-trophic hypogonadism |
| History of Head trauma/irradiation/pituitarysurgery/encephalitis | None | + In hypogonadotropichypogonadism |
| body mass index (BMI) | Normal | Decreased in primary and secondary malnutrition and chronic disorders causing HH |
| General look | Normal | Syndromes associated with HH : e.gPraderWilli, Noonan syndromes |
| Galactorrhea | None | In hyperprolactinemia causing HH |
| Anosmia | None | In Kallman syndrome |
| Gynecomastia and small firm Testis | None | In klinefilter syndrome and |
| Testicular volume | >4 ml | <4 ml |
| Basal T | >1.7 nmol/L | <1.7 nmol/L |
| T response to HCG (1500 U EOD- IM X3) [13] | >8 nmol/L | <3 nmol/L |
| LH after GnRH test (Nafarelin 0.1 mg/m2) [14] | Increment>4.6 U/L | Increment<2 U/L |
| T after HCG x 3 days [12] | T>9 nmol/L | T<9 nmol/L |
| LH (4h) after decapeptyl (0.1 mg/m2) [15] | LH>8 U/L | LH<8 U/L |
| T (7th day) after HCG x3 (EOD) [15] | T>8 nmol/L | T<8 nmol/L |
| T after 24 h of IM Low dose HCG (15 U/kg-once) [16] | T>6 nmol/L | T<6 nmol/L |
| LH after low dose GnRH (10 mcg IV) [17] | ++ Response | No response |
+may be found in the condition.
Table 1: Different Clinical and lab tests to differentiate CDGP (transient) from permanent HH [15-20].
Permanent hypogonadism may be difficult to distinguish from CDGP. CDGP is a transient state of Hypogonadotropic Hypogonadism (HH) associated with prolongation of childhood phase of growth, delayed bone age, delayed or attenuated growth and low insulinlike growth factor-1 secretion (IGF-I). There is frequently a family history of constitutional growth delay. After late occurrence of normal pubertal development 40 % or more these boys would have an Adult Height (AH) that does not reach the mid-parental adult height for the individual [21]. Because of their relatively small size and lack of sexual characteristics in comparison with their adolescent peers, some suffer negative psychological effects. Their delayed puberty also may increase their risk to develop decreased bone mass [22].
Transient delayed puberty with low T, LH, FSH and delayed bone age may occur in many clinical conditions including malnutrition (primary or secondary to a chronic systemic illness), inflammatory bowel disease, renal disease, cystic fibrosis, malnutrition, and anorexia nervosa. These clinical conditions should be ruled out before the diagnosis of CDGP [6,23,24].
Detailed history and physical examination, including auxological parameters and bone maturation are necessary to evaluate adolescents with delayed puberty. Familial history of delayed puberty is useful to support the diagnosis of CDGP whereas history of anosmia or undescended testes suggests the diagnosis of Kallmann’s syndrome. History of head trauma or midline facial defect, visual field defect, headache, irradiation proposes pituitary disorder. History suggestive of eating disorder (bulimia-nervosa) and intake of drugs that interfere with testosterone (opiates, steroids) intake shall be asked. Evidence of other endocrine deficiencies such as central hypothyroidism or secondary adrenal insufficiency, visual field disturbances, headaches, or seizures may also be associated with pituitary tumors or other central disorders [25-27] (Table 1).
Careful physical examination should include measurement of testicular size and consistency, palpation of the spermatic cord and presence of scrotal mass, fluid or varicocele. The majority of testicular mass (85%) consists of germinal tissue, a reduced germinal cell mass would be associated with a reduced testicular size and a soft consistency. Testicular volume>4 ml suggests CDGP, whereas volume<4 ml suggests HH [14,16] If the germinal epithelium is damaged before puberty, the testes are generally small and firm. If post-pubertal damage occurs, the testes are usually small and soft [17]. The amount and distribution of body hair, including beard growth, axillary hair and pubic hair, should be noted. Any decrease in body hair or decrease in beard growth should also be noted. The presence and degree of gynecomastia should be recorded. The presence of galactorrhea would suggest pronounced hyper-prolactinemia [18-20].
Laboratory investigations are helpful to rule out some chronic systemic conditions that may present only by delayed growth and puberty (e.g. chronic renal insufficiency, malabsorption, and inflammatory bowel disorders). Endocrine evaluation includes measurement of basal serum levels of LH, FSH, T, TSH and prolactin. A low T level with low LH and FSH values indicate Hypogonadotropic Hypogonadism (HH). Low T with elevated FSH and LH values help to distinguish primary testicular failure (hypergonadotropic hypogonadism) from secondary testicular failure (hypergonadotropic hypogonadism). Basal testosterone level>1.7 nmol/L suggests CDGP whereas level <1.7 nmol/L suggests HH [15-25]. Further studies can help differentiate between CDGP and HH. These include Human Chorionic Gonadotropin (hCG) and/ or GnRH/GnRH analog tests. Extended tests using HCG has increased positive predictive value to 92%. A single simple discriminatory test is to measure serum inhibin B. Value of serum inhibin-B<35 pg/mL has a 93% positive predictive to diagnose HH versus CDGP [26,27].
GH-IGF-I axis should be evaluated in short patients (HtSDS<-2 SDS) with decreased growth rate, after priming with sex steroids. Results of IGF-I and IGFBP3 levels should be interpreted using skeletal age rather than chronologic age [25-28].
In adolescents with secondary hypogonadism Magnetic Resonance Imaging (MRI) of the sella turcica may be necessary to evaluate hypothalamic-pituitary anatomy and rule out tumors, infiltrations, cysts or malformations. In adolescents with primary testicular failure a karyotype is necessary to exclude Klinefelter syndrome [29].
In summary, detailed history taking, physical examination and targeted lab and imaging investigations allow proper diagnosis of hypogonadism and its cause.
Why to treat CDGP?
1. Many boys with CDGP do not attain their mid-parental height and a good percentage of them end short for general population.
2. Some of them have combined CDGP and familial short stature
3. There is some evidence that this transient, state of hypogonadism might adversely affect the total bone mass of adults who had CDGP
4. The psychological stress experienced by the child or his parents. This may lead to incompetence and vulnerability, impaired selfesteem, reluctance to participate in athletic activities, social isolation, impaired academic performance, substance abuse and disruptive and suicide behavior have been reported in many studies [25-28,30].
Treatment, effects and monitoring of androgen therapy in CDGP:
In peripubertal male with CDGP, T therapy can be used to induce pubertal development, accelerate growth and bone mineral accretion and ameliorate the psychosocial aspect of the adolescents [31,32]. Depot T injection is still the most common drug used to treat this condition. Different T doses have been used by many authors with apparently satisfactory results. Short-course low-dose depot T IM is an effective, practical, safe, well-tolerated and inexpensive regimen (Table 2) [31-33]. Acceleration of the onset of central puberty occurs in the majority of adolescents with CDGP with enlargement of the testes during or in the 3-4 months following short course (4-6 months) confirming the start of normal spontaneous gonadotropins secretion by the pituitary. However, some patients with CDGP require longer and/ or repeated courses of T to induce onset of true puberty (18 months) until maturation of their hypothalamic-pituitary-gonadal axis evolves [23-28]. In the majority of patients 6 months of therapy appear to be enough to induce puberty [32,33].
| Dose/route | Duration (mo.) | Growth | HtSDS during treatment | Final Ht/Bone age during treatment | Puberty |
|---|---|---|---|---|---|
| T 50 mg IM | Monthly x 4 months | Increased | Increased | Not affected | Accelerated |
| T 1mg/Kg IM | Monthly x 20 months | Increased | Increased | Not affected | Accelerated |
| T 40 mg PO | Daily x 6 months | Increased | Increased | Not affected | Accelerated |
Ht SDS: Height standard deviation score; T: testosterone; PO: orally.
Table 2: Testosterone therapy for boys with CDGP [31-33].
The clinical challenge is to modify T replacement to induce puberty and optimize total skeletal growth without inducing accelerating the bone age or adversely affecting spermatogenesis. T therapy should be adjusted to simulate the physiologic (gradually increasing) levels of T from Tanner II (average 60-150 ng/dL) to Tanner III (150-250 ng/ dL) (5.2-8.6 nmol/L)to Tanner IV (250-500 ng/dL) (8.6-17.3 nmol/L) to Tanner V (500-750 ng/ dL) (17.3-26 nmol/L) (Table 3) [34]. In order to do that it the authors of this review advise to start with lower dose (e.g. 30-50 mg/month or 15-25 mg every 2 weeks monthly) using one of the long-acting esters (enanthate or cypionate) and gradually increasing the dose by 5 mg every 2 months [14].
| Testosterone dose IM/month | Serum T 7th day | Serum T 15th day | Serum T 30th day |
|---|---|---|---|
| 50 mg | 540 ng/dL | 140 ng/dL | 67 ng/dL |
| 100 mg | 586 ng/dL | 156 ng/dL | 54 ng/dL |
| 200 mg | 1500 ng/dL | 350 ng/dL | 125 ng/dL |
Table 3: Average serum concentrations of T after T depot injection [34].
Measurement of serum T levels is the most cost-effective way of monitoring T replacement therapy. In patients being treated with T enanthate or cypionate, serum T levels should be in the mid-normal range (as required) 1 week after the injection. If nadir levels 14 days after the injection are low, the interval between injections may be shortened (Table 3) [34-36]. Serum T concentration = or >100 ng/dL (3.5 nmol/L) 4 weeks after the injection points out to enough endogenous production of T and proves maturation of the HPG axis [34-36]. Although serum T measurement can be measured for better titration of the dose, the majority of clinicians do not measure T level to follow therapy in boys with CDGP.
An Aromatase Inhibitor (AI), e.g., letrozole (2.5 mg/PO) in addition to T (1 mg/kg/month for 6 months) appears to improve (increase) the adult height to approach mid-parental height versus T plus placebo. Several AIs are available in the market however many of the AIs agents are not FDA approved and there are still a number of safety concerns [37,38].
Low-dose oxandrolone (Table 4)
| Stanhope et al.[38] |
Stanhope et al.[39] |
Stanhope et al.[39] |
Papadimitriou [40] | Wilson [41] | Wilson [41] |
|---|---|---|---|---|---|
| 24 | 10 | 9 | 46 | 20 | 20 |
| 14.4 | 14.3 | 14.4 | 11.9 | 11-14.7 | 11-14.7 |
| Oxandrolone 2.5 mg/d for 3-6 months |
Oxandrolone 2.5 mg/d for 3 months |
Placebo | 0.05 mg/kg/day for a year | 0.1 mg/kg/d for 1 year | placebo |
| 2.4 y | 1.7 | 2.3 | 1.9 | ||
| 3.8 cm/y | 4.5 | 5.1 | 4 | ||
| 8.1 cm/y | 9.6 | 5.2 | 7.5 | 9.5 | 6.8 |
| 7.4 cm/y | 8.6 | --- | 7.6 | Increased | Not increased |
| 8.4 ml | 4.9 | 4.7 | --- | --- | --- |
| 9.3 ml | --- | --- | Same as controls | Same as treated | |
| 10.5 ml | --- | --- | --- | --- | |
| ND | 1 | 0.9 | --- | --- | |
| 1.25 | 0.88 | --- | --- | ||
| 1.33 | --- | --- | --- |
GV: growth velocity, B: before treatment, A: after treatment, IGF-I: insulin-like growth factor-I.
Table 4: Summary of different studies about oxandrolone use in CDGP [39-41].
Stanhope et al. [39] treated 24 boys with CDGP with oxandrolone (2.5 mg daily) for 0.21 to 0.65 years. The mean increment of growth velocity was 4.4 cm/year during treatment, which was maintained at 3.7 cm/year after treatment. There was no significant change in height for bone age standard deviation scores. Another randomized double blind study included 19 boys with CDGP who were randomized to treatment and placebo groups. Ten boys received oxandrolone, 2.5 mg per day (mean dose 0.072 mg/kg/day), and nine boys were treated with placebo. Mean growth velocity increased from 4.5 cm/year in the oxandrolone treated group to 9.6 cm/year in three months, and this was sustained at 8.6 cm/year after cessation of treatment. In the placebo treated group, growth rate showed no alteration from 5.1 cm/year to 5.2 cm/year [40]. Boys in the untreated group were then treated with oxandrolone, 2.5 mg a day (mean dose 0.073 mg/kg/day) for three months and growth velocity accelerated to 8.6 cm/year. Serum IGF-I increased significantly in the treatment group but not in the placebo group [40] In another study oxandrolone was used in 46 patients with a relatively smaller dose (0.05 mg/kg) for longer period (0.9 year) in younger age (11.9 y) with CDGP. Growth velocity increased from 4 cm to 7.5 cm during treatment and was sustained at 7.6 cm/y after stopping the treatment [40]. Oxandrolone treatment at higher dose (0.1 mg/kg/day) for one year in 20 boys with CDGP increased significantly growth velocity compared to controls not taking oxandrolone (9.5 cm vs 6.8 cm /year) [40]. Long-term use of low-dose oxandrolone (for 30-36 months) in 18 boys with CDGP increased GV to 7.7 cm/yr compared to controls 5.1 cm/y. The total gain in the treatment period was higher in the treatment group (25.5 cm) versus controls (19.8 cm). However the final height of both groups did not differ significantly [41,42].
A study on small number of boys with CDGP compared the effect of low dose oxandrolone (2.5 mg /day) versus T 50 mg IM monthly for a year on the pituitary growth and gonadal axis. In the oxandrolone group LH and testosterone parameters decreased at 3 months followed by a rebound increase at 6 and 12 months. SHBG levels were markedly reduced at 3 months (P = 0.006) At 6 months, an increase in GH pulse frequency but not amplitude occurred. IGF-I levels were increased at both 3 and 12 months. In T group, pituitary-testicular suppression was not apparent, but GH levels increased with an increase in GH amplitude at 3 and 12 months. In summary oxandrolone transiently suppressed the pituitary-testicular axis and altered GH pulsatility whereas T increased GH via amplitude [43]. A double-blind, placebocontrolled compared letrozole (aromatze inhibitor) to oxandrolone effects upon growth and puberty of children with CDGP. Ninety one boys with CDGP (12.6-14.6 years old) with predicted short stature were treated with letrozole (2.5 mg/day), oxandrolone (2.5 mg/day), or placebo, for 2 years. Oxandrolone, and to a lesser degree letrozole, significantly increased the height standard deviation score and bone age compared to placebo. Letrozole differed from oxandrolone and placebo in significantly increasing the adult height (PAH) (p<0.05) [43]. A substantial weight gain in adolescents and gains in lean body mass (LBM) and muscle size in old patients with a relatively short course of therapy proved an anabolic effect of oxandrolone on muscles. [36,41,42] In girls with Turner syndrome adding oral oxandrolone 0.1 mg/kg/day to GH therapy for 2-5 years increased growth of these girls compared with those on GH therapy alone [44].
In summary, oxandrolone, when used in an appropriate regimen, is an effective, safe treatment for boys with CDGP. It use in low dose for 3-12 months is associated with mean increment of growth velocity during treatment, which is maintained after treatment, with no significant change in height for bone age standard deviation scores. Oxandrolone does not cause virilization. The possible use of oxandrolone earlier in the course of CDGP represents an advantage of this therapy and allows the use of other form of therapy later on if puberty is delayed.
The use of dihydrotestosterone (DHT) (Table 5)
| DHT dose | Duration | Effect on linear growth | Effect on GH-IGF-I axis |
|---|---|---|---|
| 50 mg IM q 2 weeks [45] | 4 months | Not known | No change |
| 50 mg IM q 2weeks [46] | 2.5 months | Increased growth velocity | Decreased GH and IGF-I secretion |
Table 5: Effect of dihydrotestosterone on linear growth and GH-IGF-I Axis.
Dihydrotestosterone (DHT) therapy (50 mg IM every 2 weeks, for 4 months) in adolescents with CDGP was associated with appearance of secondary sex characteristics (Tanner II), increased lean body mass and decreased of body fat percentage with no change in IGF-I, mean nocturnal GH, and estradiol (E2) concentrations. In theory, lack of E2 effect may increase the potential for final height, as with adding aromatase inhibitor; however, studies about the effect on AH are lacking [45].
A study compared the effects of T vs DHT in the treatment of CDGP in 9 adolescents with CDGP (Tanner stage 1 or 2) were studied before and during treatment with T enanthate (group A) or DHT heptanoate (group B). After 2.5 months of treatment, the GV was 12.6 ± 2.8 cm/yr (n = 3) in group A and 8.9 ± 1.7 cm/yr (n = 6) in group B. In group A, the integrated concentration of GH (ICGH) increased from 3.12 ± 0.90 to 13.67 ± 6.0 micrograms/L (P<0.05), and plasma insulin-like growth factor-I (IGFI) increased from 126.7 ± 2.5 to 350.3 ± 20.3 micrograms/L (P<0.01). In group B, ICGH decreased from 4.32 ± 0.61 to 2.39 ± 0.42 (P<0.025), and IGF-I decreased from 218.3 ± 39.2 to 184.0 ± 15.8 (P = NS). The suppressive effect of DHT on GH secretion may be due to either suppression of estradiol production or a direct effect [46].
Hypogonadism
The second common indication for T use is to induce and maintain pubertal development in adolescents with hypogonadism. Hypogonadism refers to a decrease in either of the two major functions of the testes: T production and sperm production (spermatogenesis). These abnormalities can result from disease of the testes (primary hypogonadism) or disease of the hypothalamic pituitary axis (secondary hypogonadism). A simple classification of hypogonadism is presented in Table 6. When hypogonadism develops before the age of puberty, the manifestations are those of impaired puberty, including small testes and phallus, scanty or absent pubic and axillary hair, disproportionately long arms and legs (from delayed epiphyseal closure) and persistently high-pitched voice [47].
| Hypergonadotrophichypogonadism | HypogonadotrophicHypogonadism | Mixed |
|---|---|---|
| Klinefelter syndrome Orchitis Congenital or acquired anorchia Autoimmune destruction of autoimmune destruction of steroid producing cells Testicular tumors Chemotherapy Trauma Androgen receptor defects; 5–alpha reductase deficiency; Cryptorchidism; Mumps orchitis; |
Pituitary: Hypopituitarism Pituitary tumors Hypothalamic : Kallmann syndrome (congenital absence of GnRH) Constitutional delay in growth and development (transient) Chronic illnesses Malnutrition (transient) Obesity (transient) |
Thalassemia major Hemochromatosis (iron deposits in the pituitary and/or Leydig cells) Sickle cell disease PraderWilli Syndrome Glucocorticoid treatment |
Table 6: Classification of hypogonadism in adolescents.
Androgen treatment represents a main aspect of clinical management of boys with hypogonadism from adolescence onwards. In irreversible cases of hypogonadism, T is required as a replacement and should be continued for pubertal maintenance.
The different goals of T therapy can be summarized in the following:
1. To induce sex-specific secondary sexual characteristics, and then maintain them in adulthood,
2. To optimize pubertal growth spurt and have physiologic body proportions (not to be eunuchoid),
3. To obtain adequate lean muscle mass a, fat mass and optimal bone mineral mass accretion,
4. To develop adequate external genital appearance (penile size and scrotum) and internal genitalia growth,
5. To reduce cardio-vascular and metabolic syndrome risk by optimization of lipid profile; and
6. To induce sex-specific psychosocial and psychosexual maturation, and assure normal social/sexual life and well-being [46-49].
Testosterone is the only sex steroid hormone suitable for treatment in hypogonadal boys, as it fulfills the physiological requirements. However, the optimal regimens for androgen replacement therapy during adolescence remain to be defined. The new testosterone formulations (patch, gel, trans-buccal, and long-acting) have been designed for use in adults and the available dosages are probably too high to induce and manage puberty in adolescents properly. No evidence based guidelines are available on the best hormone formulations, routes of administration and doses for puberty induction [50-53].
| Form/name | Adolescent dose | Adult dose | References/Comments/side effect |
|---|---|---|---|
| Intramuscular | |||
| Testosterone enanthate | 50 mg IM monthly for 6 months in CDGP. See doses for HH |
200-250 mg/2-3 weeks | http://www.drugs.com/pro/testosterone-enanthate.html The primary adverse effect associated with injected testosterone involves fluctuating mood, energy level, and libido caused by testosterone levels that rise rapidly upon injection and then fall too low before the next dose. |
| Testosterone cypionate | 50 mg IM monthly for 6 months in CDGP. See doses for HH |
200-250 mg/2-3 weeks | http://www.drugs.com/pro/testosterone-cypionate.html |
| Testosterone undecanoate | ---- | 1000 mg/12 weeks (range 10-14 weeks) | Local pain; lack of experience and difficulty to adjust the dose in adolescents |
| Subcutaneous | |||
| Testopel® | Each contains (75mg testosterone and is ready for implantation. | 150mg to 450mg subcutaneously every 3 to 6 months. | http://www.testopel.com/ Pellet implantation is much less flexible for dosage adjustment than is oral administration of or intramuscular injections of oil solutions or aqueous suspensions. Therefore, great care should be used when estimating the amount of testosterone needed |
| Topical | |||
| Androgel ® | 1% testosterone, 0.5g per day for CDGP The dose to be escalated as needed to higher doses (1 g/day and 2.5 g/day) toward adult doses at the end of puberty or for HH (5 g/day through 10 g/day). AndroGel® is available in a metered-dose pump, which allows physicians to adjust the dosage of the medication. |
5-10 g/day | http://www.androgel.com/default.aspx http://www.fda.gov/downloads/AdvisoryCommittees/ CommitteesMeetingMaterials/PediatricAdvisoryCommittee/UCM167749.pdf Side effects of transdermal gels include adverse reactions at the site of application, acne, headache, and hair loss (alopecia). Transfer of the gel to the skin of children and women should be avoided. |
| Patch | |||
| Androderm® patch | •Androderm® is available in2 strengths, 2-mg and 4-mg. total dose of 5 mg/day. The Androderm® patch is applied to the abdomen, lower back, thigh, or upper arm and should be applied at the same time every evening between 8 p.m. and midnight | The recommended starting dose for Androderm® therapy is one 4-mg patch, applied nightly. | http://www.healthcommunities.com/testosterone-deficiency/treatment.shtml Side effects associated with transdermal patch therapy include itching, discomfort, and irritation at the site of application. Some men may experience fluid retention, acne, and gynecosmastia |
| Buccal | |||
| Striant® | A tablet-like buccal system that adheres to the gum or cheek. It is placed in the mouth where the gum meets the upper lip and dissolves into a gel that remains in place for 12 hours. It is applied twice per day. Each releases 30 mg of testosterone | 1-2 cps/day | http://www.actientpharma.com/filebin/pdf/products/58816-10_ Striant_full_PI_4pager.pdf http://dailymed.nlm.nih.gov/dailymed/archives/fdaDrugInfo.cfm?archiveid=3389 Gum or Mouth Irritation, bitter taste, gum pain, tenderness or edema may occur in some patients. |
| Oral | |||
| Testosterone undecanoate (Andriol®) | ------- | 40mg orally per day | The fluctuating levels between doses leads to symptomatic variations and prevents true physiologic simulation in CDGP. Not effective in initiating sexual development but adequate for maintenance therapy |
Table 7: Testosterone preparations and doses in adolescents [47-56].
In prepubertal adolescents with hypogonadism the challenge is to successfully simulate the physiology with low initial doses of T followed by gradual up-titration to adult-range replacement. This can be accomplished by using the proper T preparations with tailoring of the dose to attain the mid-normal range of serum T for the proper Tanner stage of pubertal development [34], with any of the approved formulations, chosen on the basis of the patient’s preference, consideration of pharmacokinetics, treatment burden and cost. T replacement in adolescents may be accomplished by injectable long acting esters (enanthate or cypionate) and even longer acting (undecanoate), by patches or drug “reservoirs”, buccally, by implants and more recently by the cutaneous administration of gels to various skin areas. A survey among US pediatric endocrinologists showed that the majority (88%) began androgen replacement therapy with low doses of testosterone esters, while only a minority used the recent transdermal patch or gel formulations. Similar results have recently been found in Italy (low dose testosterone esters 89%; patch or gel formulations 11%) [50-55].
These lipophilic esters are given via intramuscular injection in an oily solution every two to four weeks, allowing for some freedom from daily dosing. However, these T esters do not mimic the natural pattern of daily testosterone secretion and usually result in supra-physiological levels during the first few days following injection with waning over the subsequent 2 to 3 weeks. In addition, the injections are painful and disliked by many adolescents [49,53,55]. Nevertheless, T esters, such as enanthate 25-50 mg monthly given intramuscularly for 4-12 months, are commonly used to induce male pubertal development [51,54,55]. Thereafter, the doses are gradually increased up to 75-100 mg/week or 150-250 mg/2-4 weeks). The following schedule may be proposed [51- 57]: first year: 25 mg every 2-4 weeks; second year: 50 mg every 2 weeks; third year: 100 mg every 2 weeks; fourth year onward: 200 mg every 2 weeks or switched to adult dosage [51-53].
Recommended regimens for testosterone replacement therapy in adult males after induction of complete puberty include
1. 150 to 200 mg administered every 2 weeks, or 75-100 mg of testosterone enanthate or cypionate administered IM weekly.
2. One or two 5 mg testosterone patches applied nightly over the skin of the back, thigh, or upper arm, away from pressure areas
3. 5 to 10 g of testosterone gel applied daily over a covered area of skin or
4. 30 mg of a bioadhesive, buccal testosterone tablet applied to buccal mucosa twice daily Testosterone pellets
However, it appears that a protocol of twice monthly injections of low doses of T with a gradual and periodic increase in the dose would approach the physiological level of serum T appropriate for the early and middle stages of puberty in males with hypogonadism. After gradual increase of T dose for 2-3 years, the dose of T should be adjusted to keep testosterone levels between 400 and 700 ng/dl 1 wk after the injection. Oral testosterone undecanoate (Andriol®) has been proposed to induce puberty at the starting dose of 40 mg/daily in the morning. Unfortunately, the fluctuating levels between doses leads to symptomatic variations and prevents true physiologic simulation [56].
Transdermal T delivery systems have not been studied well in children <18 years of age, so their use in pediatrics is off-label [57]. A scrotal and non-scrotal patches contains fixed doses per patch suitable for adult male T replacement, they are not suitable during the transition from prepubertal to adult when relatively small doses of T are required for adolescent development [53-57]. A patch is worn, either on the scrotum or elsewhere on the body (abdomen, lower back, thigh, or upper arm) 12 or 24 hours. The most common side effects associated with transdermal patch therapy include itching, discomfort, and irritation at the site of application. Less frequent side effects include fluid retention, acne, and gynecosmastia [58,59].
New gel formulation that provide 10 mg testosterone/puff (0.5 g of gel/puff; biodisponibility 12%) (Tostrex® or Tostran®, ProStrakan LTD), has been commercialized. These gels are conveniently delivered with doses titrated by metered-dose pump; which allows physicians to adjust the dosage of the medication, gel packets, or tubes. Gels are applied once daily to the clean dry skin of the upper arms or abdomen. When used properly, these gels deliver testosterone for 24 hours. The gel must be allowed to dry on the skin before dressing and must be applied at least 6 hours before showering or swimming. Side effects of transdermal gels include adverse reactions at the site of application, acne, headache and hair loss (alopecia) [60-62].
Other less popular forms of delivery include buccal tablets and subdermal pellets. Striant® (testosterone buccal system) mucoadhesive CIII is a hormone-replacement treatment that delivers testosterone twice daily through a tablet-like buccal system that adheres to the gum or cheek. As the product absorbs moisture, it gradually releases testosterone directly into the bloodstream, bypassing the gastrointestinal tract and the liver. Most of the adult patients obtained normal testosterone levels using Striant®. Side effects are usually mild and transient and resolve within 2 weeks. They include gum or mouth irritation, pain, and swelling (edema), bitter taste and headache. Abnormal breast development (gynecomastia) may also occur. Patients should report persistent gum abnormalities to their physician [63-66].
Although uncommon, some side effects are reported with the use of different methods of T therapy and should be tracked in adolescents on T therapy. These are summarized in (Table 8) [67-72].
| Risks/side effects | Comments |
|---|---|
| Benign prostatic hypertrophy | No clear evidence |
| Cardiovascular | In 2014 (June), the FDA announced that all approved testosterone products must carry a warning about an increased risk for blood clots (Venous Thromboembolism (VTE), including Deep Vein Thrombosis (DVT) and pulmonary embolism. Men should discuss their treatment and possible risks with their health care provider. Edema with or without congestive heart failure may be a serious complication in patients with preexisting cardiac, renal, or hepatic disease. No clear effect on these cardiovascular risk factors: total cholesterol, high-density lipoprotein cholesterol, C-reactive protein, or insulin sensitivity |
| Liver disease | Usually does not occur at physiologic doses; oral formulations should be avoided in men for this reason Long-term therapy with testosterone enanthate, which elevates blood levels for prolonged periods, has produced multiple hepatic adenomas |
| Polycythemia | More common in men taking higher doses |
| Virilization(alopecia, hirsutism, acne) | Usually dose and duration related |
| Gynecomastia | Frequently develops and occasionally persists in patients being treated for hypogonadism. |
| Sleep apnea | In some patients especially those with risk factors such as obesity |
| Priapism | Rare but may occur with injectable T preparations in adolescents. |
| Mood changes | Increased aggression and mood swings |
Table 8: Potential risks and side effects of testosterone treatment [68-73].
What and when to monitor after initiating T therapy
Adolescents receiving testosterone therapy should be monitored using a standardized plan (Table 9). Clinical monitoring should depend on whether T therapy is given to males with CDGP or to those with permanent hypogonadism, (anorchia or Klinefelter syndrome). In males with CDGP a significant increase in testicular size appears to be a good clinical parameter of successful pubertal induction. In hypogonadal adolescents, T therapy leads to the development of secondary sexual characteristics (penis and scrotum) and increases hair growth in several androgen-sensitive areas. It increases linear growth, fat-free mass, muscle strength and bone density and decreases fat mass. In hypogonadal adults T therapy leads to improvements in overall sexual activity scores, frequency of sexual thoughts and fantasies and increase in attentiveness to erotic stimuli, and an increase in the frequency and duration of nighttime erections.
| Test/examination | Frequency | Comment |
|---|---|---|
| History and physical examination | Every three to four months for the first year, then annually | — |
| Testosterone levels | Until stable normal range | Only necessary with injections |
| Liver function | Every three to six months | Only necessary with oral preparations |
| Prostate-specific antigen | Every six to 12 months | Annually, if unchanging |
| Digital rectal examination | Every six to 12 months | Annually, if unchanging |
Table 9: Recommended monitoring adolescents on testosterone therapy.
Biochemically serum T level should be monitored every 3 to 6 months after initiation of testosterone therapy to achieve serum testosterone level in the mid-normal range for the appropriate pubertal stage. In adults therapy should aim to raise serum testosterone level into the mid-normal range (from 400 ng/dL: 14.1 nmol/liter to 700 ng/dL: 24.5 nmol/liter). Monitoring can be done as following: (Table 10) [17,72,73]. Measurement of Bone Mineral Density (BMD) every 1-2 years (especially in those with osteoporosis or low BMD before therapy) is recommended [73-75].
| Form of Testosterone Used | Time to measure T serum level |
|---|---|
| After IM T depot injection | 1 week after injection |
| After Testosterone pellets | 1 wk after the injection |
| After transdermal patches | 3–12 h after application |
| After transdermal gels | At least 1 wk after patient has been on treatment. |
| After buccal testosterone bio adhesive | Immediately before or after application of fresh system |
| After oral testosterone undecanoate | 3 to 5 h after ingestion |
Table 10: Time to measure serum T after using different forms of T preparations.
Human Chorionic Gonadotrophin (HCG), GnRH and FSH therapy in adolescents with Hypogonadotropic Hypogonadism (HH)
HCG therapy can be used in to induce puberty in adolescent boys with CDGP, constitutional delayed puberty. In 12 adolescents with CDGP, HCG, 2500 U/m2 was injected intramuscularly twice weekly for 6 months. All adolescents with CDGP had increased growth rate (from 4.1 to 10.3 cm), testicular volume and T secretion after 6 months of HCG therapy. Growth rate and pubertal development were maintained for a year after stopping HCG [76].
Male adolescents with onset of Hypogonadotropic Hypogonadism (HH) before completion of pubertal development may have testes generally smaller than 4 ml and usually require therapy with both HCG and human menopausal gonadotropin (or FSH) to induce spermatogenesis. The initial regimen of HCG is usually 1,000 to 2,000 IU administered intramuscularly two times a week. The clinical response is monitored, and testosterone levels are measured every 2 to 3 months. Dosage adjustments of HCG may be needed to determine an optimal schedule [18,77-80].
Kim et al. studied the effect of HCG therapy (1,500-2,000 IU) administrated intramuscularly, 3 times per week, for 8 weeks in 20 idiopathic HH patients with micro-penis (Age 12:24 years). The mean serum T level was significantly increased after HCG treatment with increased penile and testicular volumes. There were no remarkable adverse effects of the HCG treatment [81].
If the patient is fully virilized and 8-12 months of HCG therapy have not led to the production of sperm, then FSH therapy should be initiated. FSH is available as Human Menopausal Gonadotropin (hMG). Once a pregnancy has occurred, the FSH therapy can be stopped and spermatogenesis can be maintained with HCG alone [18,77,81].
GnRH is a feasible way to induce testicular growth as well as spermatogenesis in hypogonadotrophic male patients, even in patients in whom gonadotrophin treatment has failed. In one study GnRH was administered intravenously in a dose of 2-20 micrograms per pulse every 90 minutes in 38 patients with HH. After GnRH discontinuation, HCG treatment was instituted, 1500-3000 IU (IM) twice weekly. During treatment plasma levels of LH, FSH and testosterone increased with increased testicular volume from 2.4 to 4.8 ml to 11.5-18.1 ml by the end of treatment. GnRH treatment mean lasted between 46 and 75 weeks in the different groups. On HCG therapy, testicular development was either maintained or improved. Semen analysis revealed the presence of spermatogenesis in 31 out of the 38. In 19 adolescent patients with growth potential, an adequate height velocity was observed during GnRH treatment. A GnRH treatment schedule with an increasing pulse frequency and pulse dose can imitate the ‘physiological’ pubertal changing pattern of gonadotrophins just as well as the use of sex steroid [82-84].
In summary; although physiologically potent, HCG, GnRH and FSH are infrequently use outside of clinical research protocols and for stimulating spermatogenesis in males with hypogonadotropic hypogonadism because they are time-consuming, expensive and require multiple injections.
Adolescent athletes and use of testosterone as anabolic agent and in body building
Epidemiological data are available for anabolic steroids in adolescent high school athletes (4-12%), but not specifically in high level athletes. They are used by athletes to induce muscle hypertrophy and increases in strength in athletes who take anabolic steroids especially in weight lifters, and endurance and sprint athletes. None of these studies are controlled. In addition, many adolescents use androgens to “look good” (muscular physique) [85,86].
In addition, information on doses and modes of administration of anabolic- androgenic steroids used by athletes to increase their performances is relatively scant. It is known that body builders follow a typical pattern called “stacking”, based on administration of several oral and injectable anabolic-androgenic steroids during cycles lasting 4-12 weeks. The advantage of this practice has been demonstrated recently [87]. The drug dosages range from 250 mg to 3500 mg per week and are therefore up to 40 times the recommended therapeutic dosage.
There are many health dangers from the use and abuse of anabolic steroids. In the prepubertal adolescent, acceleration of epiphyseal maturation of the long bones and short stature occurs. Other side effects include: infertility, gynecomastia, testicular atrophy, malepattern baldness, unfavorable lipid profiles, hepatic dysfunction and severe nodular acne. Psychologically administration of anabolicandrogenic steroids may affect behavior and high T levels are associated with masculine behaviour, aggressiveness and increase of sexual desire. Euphoria, confusion, sleeping disorders, pathological anxiety, paranoia and hallucinations are other side effects of using anabolic-androgenic steroids [88-90]
Anabolic steroids are banned by all major sports bodies including the Olympics, the NBA, the NHL, and the NFL. The World Anti- Doping Agency (WADA) maintains an extensive list of all banned performance-enhancing substances [89-92].
Testosterone therapy is recommended for adolescents with CDGP to induce puberty and in those with permanent HH to induce then maintain pubescent development. Short course of small doses of testosterone depot (30-50 mg IM monthly) for 4-6 successfully induces pubertal development, accelerate growth and bone mineral accretion, in the majority of patients with CDGP and in some reports improves the psychosocial complaints of the adolescents. Some patients need a more prolonged course (12-18 months) of T therapy. In adolescents with permanent HH T replacement therapy improves overall sexual activity, increases the frequency and duration of nighttime erections, and decrease the risk of future problems with fertility, mood disturbances, fatigue, impaired virilization and osteoporosis. Many other forms of T are now available for use including T patch and gel. Side effects may occur but they are generally infrequent. Endocrinologists, pediatricians and physicians should be familiar with the forms of T available, optimal timing, dose titration, monitoring of therapy and possible side-effects to accomplish the best pharmacological outcome. In addition, it is believed that through education and research we can mitigate the abuse of androgens by athlete adolescents.