Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
ISSN: 2167-7948
Case Report - (2012) Volume 1, Issue 2
Graves’ disease affects skeletal systems in different ways. Most commonly, it causes secondary osteoporosis complicated with fragile fracture in the background of vitamin D deficiency. Here, we are describing a case of Graves’ disease presenting as thyrotoxicosis with genu varum deformity.
<Keywords: Graves' disease; Vitamin D; Genu Varum
Graves' disease is the most common cause for thyrotoxicosis and usually presents with symptoms due to increased basic metabolic rate and sympathetic system overactivity. It affects all parts of the body including musculoskeletal system. There are various presentations of skeletal involvement like osteopenia/osteoporosis, osteomalacia, low trauma fracture, hypercalcemia, hypocalcemia etc. However, genu varum as the presentation of Graves' disease in adult patient is a rare clinical entity.
A 43 year old female with bilateral bowed legs with difficulty in walking presented to endocrinology clinic. These symptoms were progressive over last one year. She had also symptoms suggestive of proximal muscle weakness in lower limbs in form of difficulty in climbing up the stairs and standing up from sitting position. For past six months, additionally she had weight loss, hyperdefecation, palpitation, breathlessness on exertion and tremulousness of hands. She denied any history of trauma or fracture in the recent past. There was no similar illness in the family and her past history was not contributory other than hysterectomy (5 years back). She did not have history of intake of drugs like glucocorticoids, anti-epileptics and anti-tubercular drugs. She takes non-vegetarian diet & iodised salt and her lifestyle does not allow adequate sunlight exposure. Examination revealed waddling gait, thin built, pallor, sinus tachycardia, fine tremors of hands, diffuse soft goitre (Figure 1). There were no features suggestive of Ophthalmopathy or Dermopathy. Lower limb examination showed genu varum deformity without features of arthritis (Figure 2). Neuro-Muscular system examination elicited 3/5 power in pelvic girdle and 4/5 power in pectoral girdle. Systemic examination was otherwise unremarkable except ejection systolic murmur (grade– II) in pulmonary area. Trousseau's sign and Chvostek's sign were absent. Hemogram showed microcytic hypochromic anemia. Fasting plasma glucose, renal function test and urine routine examination were normal. Her corrected serum calcium was 9.5 mg% (9-11 mg%) and serum phosphorus was 4.5 mg% (3-5 mg%). Liver function test was normal except raised serum alkaline phosphatase- 146.9 IU/L (42-78 IU/L). Serum vitamin D level was 12.75 ng/ml (30-100 ng/ ml). Thyroid function test revealed primary thyrotoxicosis with serum free T3 11.08 pg/ml (2.3-4.2), free T4 3.32 ng/dl (0.8-2.5) and TSH <0.005 μIU/ml (0.27-4.2). X-ray of knee joint (Figure 3) showed varus deformity. Tc-99m thyroid Scintigraphy (Figure 4) was suggestive of Graves' disease. So, the final diagnosis of Graves' disease with moderate vitamin D deficiency with genu varum with microcytic hypochromic anemia was made. Subsequently, She was started on Antithyroid drug (Carbimazole- 20 mg), nonselective beta-blocker (Propranolol-40 mg), therapeutic dose of Cholecalciferol (60,000 units orally once per week for 12 weeks followed by once a month) and haematinic (iron & folic acid) supplementation. Conservative treatment (physiotherapy and analgesics) for genu varum was started with consultation of orthopaedic department. The patient was symptomatically better in the last follow up (six months after initiation of treatment).
Figure 1: Neck showing diffuse goitre.

Figure 2: Lower limbs showing genu varum deformity.

Figure 3: LX-ray of Right knee showing genu varum deformity.
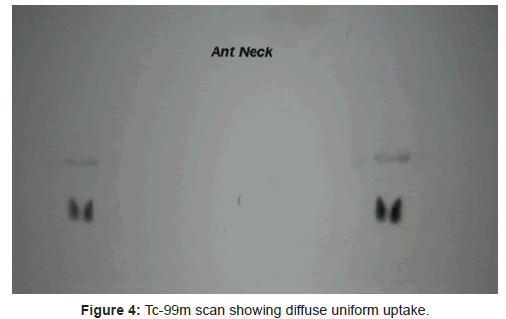
Figure 4: Tc-99m scan showing diffuse uniform uptake.
Thyrotoxicosis affects bone mineral metabolism in different ways. It is a known fact since 1891 when Von Rcklinghausen published the first paper [1]. It increases the rate of bone remodelling leading to net bone loss (Osteopenia/osteoporosis) and fragility fracture [2]. In addition, associated myopathy also contributes to fracture by increasing the risk of fall. Low serum vitamin D level has also been established in these patients [3]. Proposed mechanisms are: decreased synthesis in skin due to thyrotoxicosis-associated hyperpigmentation, decreased absorption due to steatorrhea and increased degradation due to hepatic enzyme stimulation. Serum calcium and phosphorous level may be low, normal or high depending on the severity of thyrotoxicosis and associated abnormalities [4,5]. Though bone mineral density is not available, low serum vitamin D with high alkaline phosphatase in presence of normal calcium/phosphorus level in the background of post-menopausal status is obvious in our patient.
Genu varum is a common manifestation of vitamin D deficiency during childhood [6]. However, it is usually due to injury, arthritis or may be the late manifestation of hypophosphatemic rickets in adults [7-10]. These can be excluded as etiology in our patient with normal serum phosphorus level in the absence of history of injury and features of arthritis. This deformity decreases the quality of life significantly in presence of myopathy and requires symptomatic treatment in most patients like the index case.
So, genu varum may be an intial clue for Graves' disease. By diagnosing early, we can avoid late life threatening cardiovascular complications of thyrotoxicosis like arrhythmia. This may be the first case establishing the relationship between Graves' disease and genu varum.